Association between transfer for surgery and mortality and disability among neonates in high income countries—A systematic review with meta-analysis
Haribalakrishna Balasubramanian, Abhishek Srinivas, Prathamesh Khedkar, Anitha Ananthan, Diwakar Mohan, Nandkishore Kabra, Sanjay Patole

TL;DR
This study finds that transferring neonates with surgical conditions to another hospital does not increase their risk of death or disability.
Contribution
The study provides a comprehensive meta-analysis on the impact of neonatal surgical transfers in high-income countries.
Findings
Transfer for surgery was not associated with increased mortality in neonates with congenital diaphragmatic hernia.
Neurodevelopmental outcomes were comparable between transferred and co-located care neonates.
Evidence certainty was low due to observational study designs and heterogeneity.
Abstract
Birthing in a hospital with on-site surgical facilities (co-located care) is considered preferable for neonates with surgical conditions. However, it may not always be feasible. Whether transfer of surgical neonates from birth hospital to a surgical facility affects the outcomes of this cohort is unclear. We conducted a systematic review to investigate the association of birth location/transfer with all-cause mortality and disability among neonates with congenital/acquired surgical conditions. Data Sources from PubMed, Embase, CINAHL, and Web of Science were searched till December 2024. Studies from high-income countries (HICs) comparing infants transferred to a surgical center for surgery versus infants born and operated in a co-located care facility were included. Random effects model was used for meta-analysis. The quality of studies and certainty of evidence were assessed using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
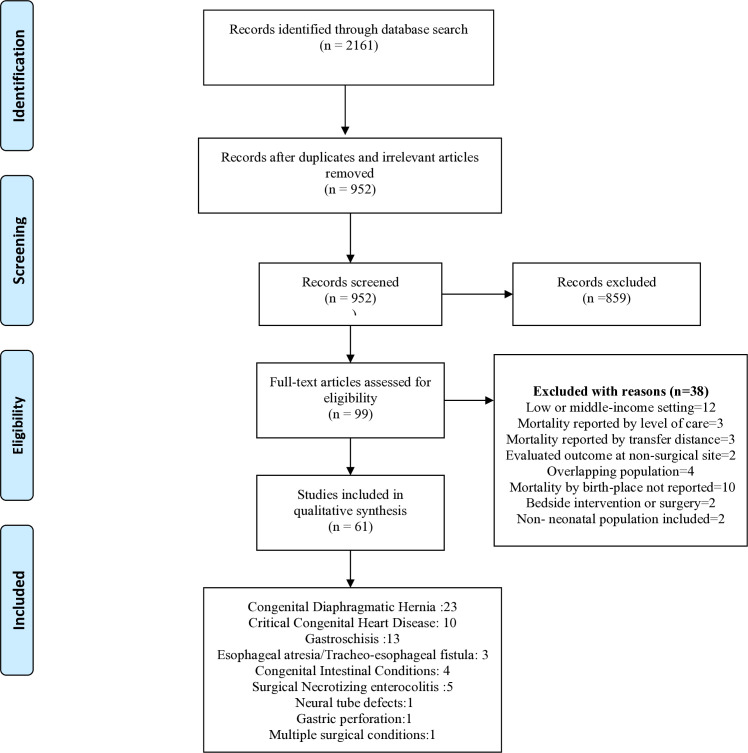 Fig 1
Fig 1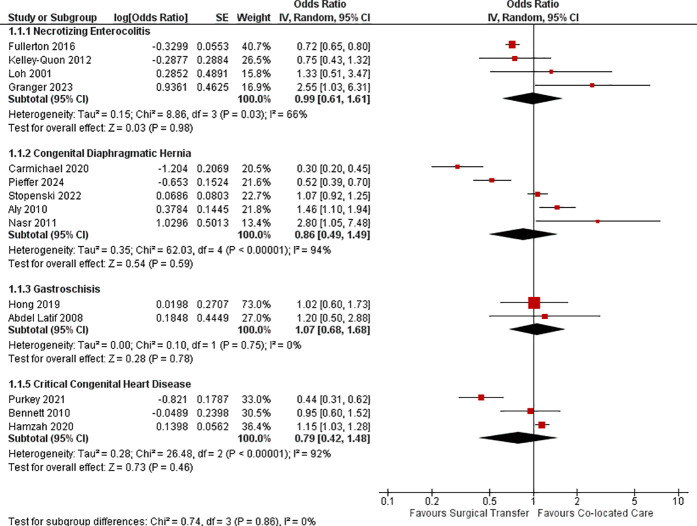 Fig 2
Fig 2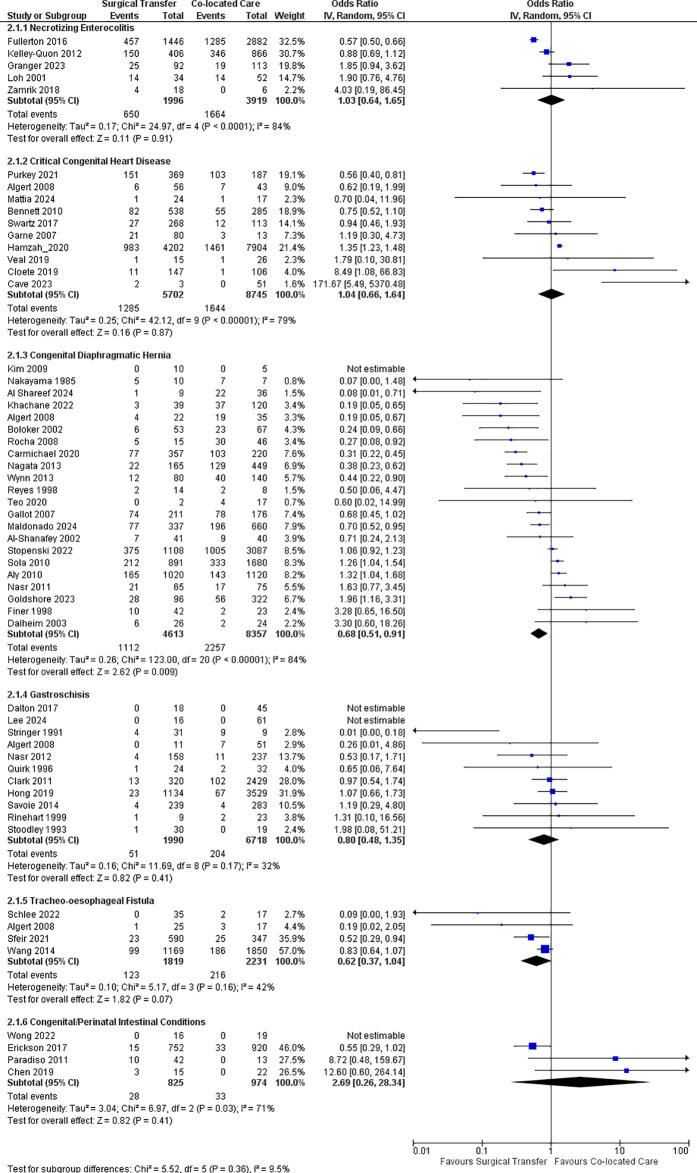 Fig 3
Fig 3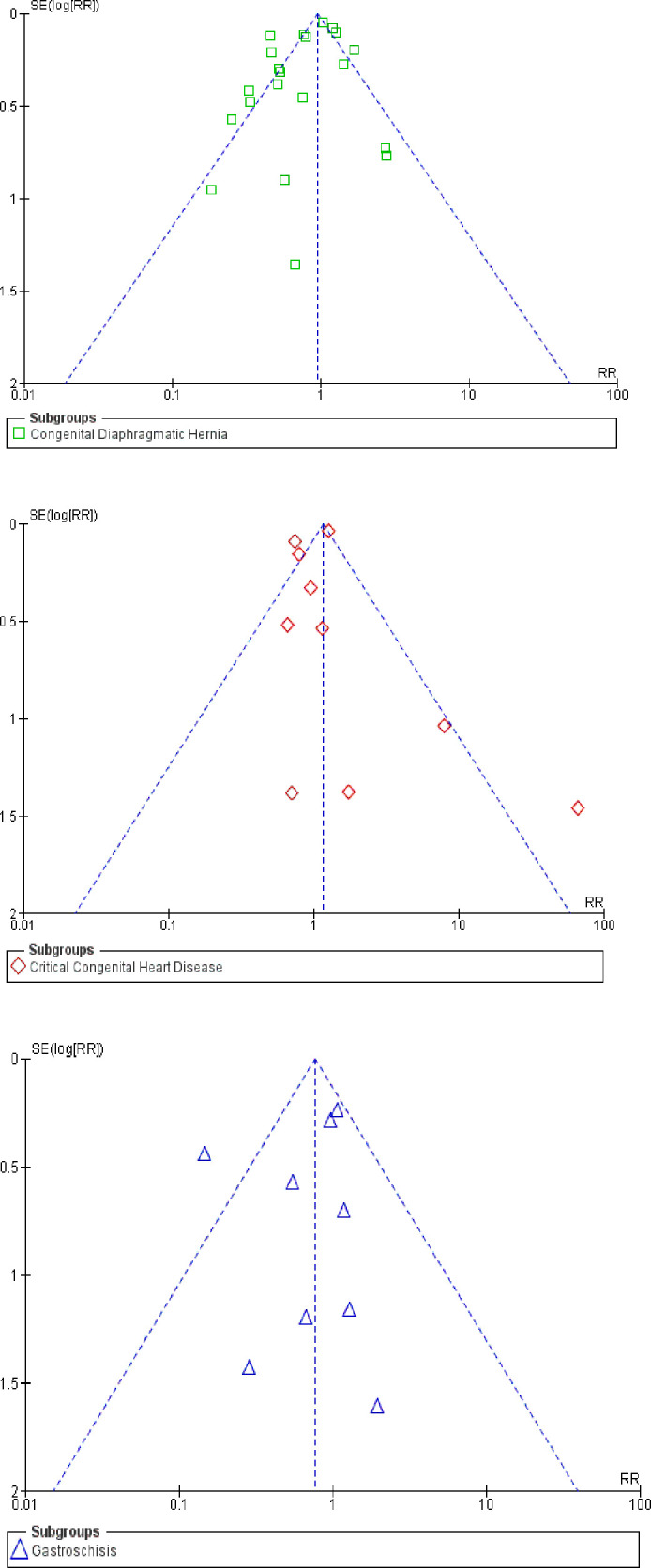 Fig 4
Fig 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Congenital Anomalies and Fetal Surgery · Esophageal and GI Pathology
Introduction
Infants requiring surgical intervention during the neonatal period are at higher risk of mortality and morbidities. Whilst birthing in a hospital with on-site surgical facilities (co-located care) is considered preferable for such infants to optimize care, it may not always be feasible. Nearly 40–45% of neonates with major surgical conditions need transfer from the birth location to a surgical facility for specialist care [1,2]. Unlike very preterm neonates without surgical conditions [3–5], the association of birth location with adverse outcomes is not clear among neonates with various surgical conditions. A systematic review that covered gastroschisis, tracheoesophageal fistula (TEF) and congenital diaphragmatic hernia (CDH) reported that the evidence in this area is conflicting [6].
Granger et al. reported outcomes after surgically managed necrotising enterocolitis (NEC) and focal intestinal perforation (FIP) in infants <32 weeks requiring transfer to or presenting in a single surgical center. Being transferred was associated with increased all-cause mortality and mortality attributable to NEC or FIP, but no differences in neurodevelopmental outcomes among survivors [7]. Other investigators report that survival and early postoperative mortality was not affected by the distance from hospital of birth to a surgical center in neonates with critical cardiac conditions including hypoplastic left heart syndrome (HLHS) and transposition of great arteries (TGA) [2,8].
Considering that surgical neonates account for 20–60% of emergency neonatal transports [9,10], a comprehensive evaluation of outcomes associated with neonatal surgical transfers is required to guide perinatal care including triaging and neonatal retrieval priorities in this high-risk cohort. Apart from the severity of the underlying condition and retrieval distance, the standard of neonatal care at the hospital of birth, and importantly, during transport is critical for survival of neonates with major surgical conditions. Hospital mortality in this cohort varies from 4–40% in high income countries (HICs) [11,12] with better survival in centers with high operative case volumes [13,14]. Given the significance of the underlying issues, we aimed to systematically assess if transfer from the birth hospital to a surgical center is associated with mortality and disability among neonates with major surgical conditions in HICs.
Methods
We followed the Cochrane handbook of systematic reviews for observational studies [15] for conducting and the MOOSE (Meta-analyses Of Observational Studies in Epidemiology) guidelines for reporting this systematic review [16]. The protocol was registered in the international prospective register of systematic reviews (PROSPERO id: CRD42024565651).
Type of studies
Prospective or retrospective non-randomised (e.g., Cohort, case-control) studies conducted in HICs (World Bank classification 2024) [17] were included. We excluded studies conducted in low- and middle-income countries since protocols for regionalisation of care for surgical neonates may not be uniformly well established in such countries. Randomized controlled trials (RCTs) were eligible for inclusion but not expected for obvious reasons.
Search strategy
We searched PubMed, Embase, CINAHL and Web of science, Google scholar, and conference abstracts from conception till December 2024. Reference lists of included studies and related systematic and narrative reviews were searched to identify additional or ongoing studies. No language restrictions were applied. The search strategy is included in the supplement. (S1 File)
Inclusion criteria
We included studies that evaluated the impact of hospital transfer on neonates with major surgical conditions. We compared two groups of infants: (1) those transferred from the birth hospital to a surgical center (surgical transfer group); (2) infants born and operated in a hospital with surgical facility (co-located care group). We included infants that underwent open surgical procedures, minimal access surgeries or catheter-based interventions. Infants were categorized irrespective of the time of diagnosis (antenatal/postnatal) or presentation (congenital/ acquired) of the surgical condition.
Infants who underwent surgery beyond the neonatal period (>28 days) were included only if they were still in the hospital since birth when they underwent surgery.
Exclusion criteria
Elective inguinal hernia repairs and retinal laser photoablations were excluded. When two or more studies selected infants from the same hospital or database, with overlapping study time frames, we selected the largest and the most recent study reporting the desired outcomes for our analyses.
Surgical conditions
Our prespecified list of major congenital or acquired surgical conditions included:
(1) Gastrointestinal: (a) Congenital: Esophageal atresia (EA) with or without TEF, congenital diaphragmatic hernia (CDH), gastroschisis, exomphalos, intestinal atresia, meconium ileus/peritonitis, intestinal malrotation/volvulus, Hirschsprung disease, anorectal malformations. (b) Acquired: NEC, spontaneous intestinal perforation.(2) Cardiovascular: Critical congenital heart defects (CCHD) including TGA, HLHS, hypoplastic right heart syndrome, truncus arteriosus and other ductal dependent cardiac lesions(3) Neurological: Neural tube defects, congenital or acquired hydrocephalus(4) Others: Congenital pulmonary and airway malformations, urogenital malformations.
Outcomes:
The primary outcome for this systematic review was all-cause mortality (mortality during primary hospitalization or at latest follow up). Infants that died at the surgical center before surgery and infants with surgical diagnoses managed conservatively were included in outcome evaluation. Secondary outcome was long-term neurodevelopment including motor, language or cognitive impairment (assessed using validated neurodevelopmental tools), cerebral palsy, visual and hearing impairment, and autism.
Differences between the PROSPERO protocol and the final review
We stated in our protocol that infants operated beyond the neonatal period will be excluded, whereas in our final review, infants who underwent surgery beyond the neonatal period (>28 days) were included if they were still in the hospital since birth when they underwent surgery. We also prespecified that inguinal hernia cases will be excluded. In the actual review, although elective surgeries of uncomplicated inguinal hernias were excluded, inguinal hernias with complications such as obstruction, gangrene and incarceration that need emergency surgery were planned to be included.
Study selection and data extraction
Two authors independently screened studies to assess eligibility for inclusion in our review. Discrepancies in study selection were resolved in consensus with the third author. Authors (AS and PK) independently extracted information on prespecified outcomes of mortality and developmental disability and assessed the risk of bias (ROB) from the included studies. We extracted the following characteristics for each surgical condition: country, data source, study design and timeframe, proportion of infants with antenatal diagnosis and serious congenital/chromosomal anomalies, age at hospital transfer and surgery, definition of co-located care and surgical transfer. We collected information on pre and post-surgical mortality, pre-transfer mortality, palliative care, non-surgical management rates, and need for extracorporeal membrane oxygenation.
Statistical analysis
Meta-analysis was performed using the random effects model. Effect sizes were reported as odds ratios (OR) and 95% confidence intervals (CI). For studies reporting risk adjusted mortality, ORs and standard errors were logarithmically transformed and pooled using the generic inverse variance method. The I^2^ statistic was used to assess statistical heterogeneity. I^2^ values of 25% or less, 25% to 75%, and >75% were considered as having low, moderate, and high heterogeneity, respectively. The quality of included observational studies was assessed using the Newcastle-Ottawa Scale [18]. Publication bias was assessed using funnel plots if there were at least 10 included studies for a given surgical condition. We planned analysis of mortality by subgroups based on gestational age and severity of the surgical condition. Statistical significance was set at p < 0.05 and all tests were two-tailed. Revman Version 5.4 was used for all analyses. Certainty of evidence was assessed using GRADE recommendations [19].
Results
Our literature search yielded 2161 citations. After initial eligibility assessment, 99 articles were read in full text and a total of 61 studies from HICs reporting the effect of hospital transfers for surgical intervention were included (Fig 1).
PRISMA flow diagram for selection of studies.
The sample sizes of the included studies varied from 13 to 12,106 surgical infants. Algert 2008 evaluated outcomes separately for CDH, gastroschisis, exomphalos, TGA, esophageal atresia (EA) and neural tube defects with hydrocephalus [20]. Three studies reported long-term neurodevelopmental outcomes.
Four studies (Gastroschisis: 2, CDH:1, TGA:1) evaluated mortality but did not report point estimates for conducting meta-analysis. Included studies abstracted data from hospital medical records, population-level inpatient databases, disease registries or health provider surveys. The characteristics of included studies are summarized in Table 1 and additional study characteristics are shown in S1 and S3 Table. Characteristics of excluded studies were tabulated in S2Table.
Table 1: Characteristics of included studies.
CDH
A total of 24 studies [10, 20–42] involving infants with CDH were included. Twelve studies were multi-centric [10,20,23,25,26,29,33,35,36,39,40,42] and 12 were single-center studies [21,22,24,27,28,30–32,34,37,38,41]. Four studies excluded infants with associated cardiac and/or chromosomal anomalies [10,20,21,23].
Majority of studies reported in-hospital mortality as primary outcome while three studies reported mortality at 60 days and during infancy [20,26,42]. Most studies accounted for pre- and post-operative mortality in the analysis while one study [23] reported mortality only in infants undergoing surgical repair in either group. Kim et al. primarily evaluated thoracoscopic repair of CDH and reported 100% survival in both groups [32].
Risk-adjusted mortality was not significantly different between the transfer vs the co-located group [aOR 0.86 (0.49, 1.49), P = 0.59, I^2^ = 94%, 5 studies, 8366 infants [23,26,35,36,40] (Fig 2). Crude mortality was significantly lower in transfer vs co-located group infants [OR 0.68 (0.51, 0.91), P < 0.001, I^2^ = 84%, 22 studies, 12970 infants [10,20–24,26–35,37–42] (Fig 3). One study reported no significant difference in long-term neurodevelopmental outcome between the groups [41].
Forest plot for risk-adjusted mortality in surgical neonates.
Forest plot for crude mortality in surgical neonates.
CCHD
Eleven studies evaluated CCHD requiring cardiac surgery or interventional procedures during the neonatal period or primary hospitalization [20,43–52]. Six studies evaluated infants with TGA [20,44,46,48,51,52], two evaluated HLHS [47,49], three reported outcomes of more than one CCHD [43,45,50]. Eight studies were multicentric [20,43,45–47,49,50,52] and three were single center studies [44,48,51]. Five studies excluded infants with chromosomal or extra-cardiac anomalies [20,44–47].
In-hospital mortality was the primary outcome in three studies [46,47,52]. Four studies reported mortality at one year [20,46,49,51]. Other studies reported mortality at 90 [43,44] or 28 days [45,50]. Mortality before transfer was reported in only two studies [44,45]. The risk-adjusted and crude mortality at latest follow up was comparable between the transfer group and co-located group [aOR 0.79 (0.42, 1.48), P = 0.46, I^2^ = 92%, 3 studies,13485 infants [43,47,49]; OR 1.04 (0.66, 1.64), P = 0.87, I^2^ = 79%, 10 studies, 14447 infants [20,43–50,52].
Acquired intestinal surgical conditions
Infants with proven NEC or FIP referred for exploratory laparotomy or primary peritoneal drainage were evaluated in five studies [7,53–56]. Four studies were multi-centric. Four studies exclusively reported on infants with surgical NEC while one [7] included infants with either NEC or FIP.
Two studies reported mortality only among infants who underwent surgical intervention [53,56] while other three reported mortality among all co-located and transfer group infants. In-hospital mortality was the primary outcome in four studies, while one study reported mortality at one year [54]. The risk-adjusted and crude mortality were comparable between the two groups [aOR 0.99 (0.61, 1.61), P = 0.98, I^2^ = 66%, 4 studies, 5891 infants [7,53–55]; OR 1.03 (0.64, 1.65), P = 0.91, I^2^ = 84%, 5 studies, 5915 infants [7,53–56]. In one of the included studies, [53] 19% of the surgical transfers happened before diagnoses of NEC. Excluding it from the analysis did not alter the overall effect. Two studies that reported neurodevelopmental outcomes at two years found no difference between the two groups [7,56] (S4 table).
Gastroschisis
A total of 14 studies [20,57–69] were included of which seven were multi-centric [20,57,58,60,63,66,69] and seven were single center studies [59,61,62,64,65,67,68]. Two studies excluded infants with other anterior abdominal wall defects [65,66] and one excluded infants with complex gastroschisis [59]. One study included only antenatally diagnosed gastroschisis [63]. Risk-adjusted and crude mortality were not significantly different between the transfer and co-located group infants [aOR 1.07 (0.68,1.68), P = 0.78, I^2^ = 0, 2 studies, 5294 infants [57,60]; OR 0.80(0.48,1.35), P = 0.41, I^2^ = 32%, 11 studies, 8708 infants [20,58–60,62–68].
EA/TEF
Four studies were included [20,70–72]; three were multi-centric [20,71,72]. One study excluded long gap EA [70]. Three studies reported mortality among all infants in co-located and transfer group [20,71,72] while one study reported outcomes only among infants that were operated [70].
Mortality was reported during primary hospitalization [72] and at three months [71] and one year [20,70]. Mortality at latest follow-up was comparable between transfer and co-located group [aOR 0.97 (0.39, 2.39), P = 0.95, one study, 937 infants [71]; OR 0.62 (0.37, 1.04), P = 0.07, I^2^ = 42%, 4 studies, 4050 infants [20,70–72].
Congenital/perinatal intestinal conditions
Four studies were included [73–76]. Two studies were multi-centric [73,74] and two were single center studies [75,76]. Three studies evaluated infants with meconium ileus or perinatal intestinal perforation [73,75,76]; one study evaluated infants with intestinal atresia [74]. The primary outcome was in-hospital mortality in all these studies. Three studies reported mortality among all study infants, while one included only infants that underwent surgical repair [74]. In one study evaluating meconium ileus [75], nearly 50% of the infants initially designated for surgical repair were managed conservatively. In-hospital mortality was not significantly different between the study groups [OR 2.69 (0.26, 28.34), P = 0.41, I^2^ = 71%, 4 studies, 1799 infants [73–76].
Other surgical conditions
Kancherla 2021 [77] and Algert 2008 [20] studied neural tube defects and Yang 2015 [78] reported outcomes of neonatal gastric perforation (S4 table).
Assessment of study quality and certainty of evidence
Majority (n = 45/61) of the studies were judged as good quality based on assessment of the three domains a) selection of study population b) comparability of study cohorts c) outcome assessment and follow-up. 16 studies were rated low quality as they did not report mortality estimates adjusted for confounders and had unbalanced group sizes (Table 2).
Table 2: Risk of bias assessment.
The certainty of evidence was rated very low due to high risk of bias in observational studies, imprecision (wide 95% confidence intervals that included both benefit and harm) and inconsistency as evidenced by high statistical heterogeneity (Table 3). Publication bias was less likely given the visual impression of funnel plot symmetry (Fig 4).
Table 3: Certainty of Evidence.
Funnel plot for assessment of publication bias.
Sensitivity analyses
It is possible that temporal trends in transport related outcomes, severity of surgical condition, inclusion of low-quality studies and duplicate patient cohorts may impact the overall outcome estimates in our meta-analysis. Transport for neonatal surgery may putatively impact early postnatal outcomes than the outcomes through infancy.
We conducted five post-hoc sensitivity analyses: (1) excluding studies published before year 2000 (four studies each in CDH and gastroschisis). (2) excluding studies evaluating TGA among the CCHD category. (3) excluding studies of low quality. (4) including studies that only reported mortality at discharge. (5) to account for the possibility of double counting of infants across databases (Table 4). Our findings remained unchanged and robust to the sensitivity analyses.
Table 4: Sensitivity analysis.
Discussion
With a sample size of over 51,000 infants from total 20 HICs and spanning across a period of five decades, this is perhaps the first comprehensive and robust systematic review and meta-analysis evaluating the association between transport and death and disability in neonates with a range of major surgical conditions. Our assessment was restricted to HICs to ensure a comparable standard of care including transport for surgery for this high-risk cohort. Nearly 60% (36/61 studies) of the included studies extracted data from population-level databases or large collaborative neonatal or surgical networks, enhancing the validity of our findings. Our review captured survival beyond hospital discharge and through infancy, making the findings more relevant for infants with cardiac conditions requiring staged surgical repairs. Importantly, < 1% of infant deaths included in our analysis were due to palliation.
A recent systematic review of 19 cohort studies evaluated the association of birth-location with short-term outcomes for infants with gastroschisis, CDH and TEF [6]. Using a vote counting approach, they reported favourable outcomes with co-located care in seven studies and a lack of association of birth-place on outcomes in 12 studies. They misinterpreted the effect direction in three studies on CDH [20,26,33] and reported that birth in maternity unit with a co-located surgical center was associated with reduced mortality for CDH.
Reports from HICs indicate in-hospital mortality rates varying from 4–8% for gastroschisis [11], 12% for EA [79] and 25–30% for CCHD and surgical NEC [80,81]. Mortality ~70% has been reported in preterm very low birth weight infants with CDH [82]. Clinical risk prediction models may largely explain these disparities in survival and help standardize risk factors for mortality in various surgical conditions [83–87]. Many prediction models validated in contemporary surgical cohorts have not identified birth location as a significant risk factor for mortality [88–92]. Furthermore, mortality in CDH and surgical NEC has not reduced below 30% despite dedicated efforts [1,93,94]. These findings suggest that localisation of care may not independently influence mortality in most surgical infants.
A multi-center cohort study from the USA [2] evaluated survival in 790 infants with prenatally diagnosed HLHS after stage 1 palliation. The hospital length of stay, 30-day survival, or survival to discharge did not differ based on the distance from birth location to surgical center. In a Western Australian transport audit of 80 neonates with TGA transferred over ~3000 km distance to Melbourne for arterial switch repair, there was no mortality during transport and only one early post-operative death [8]. These two studies were not included in our review because they assessed the effect of transport distance rather than birth location, on mortality [2] or lacked a control group [8]. Nevertheless, their results provide further reassurance that transportation is unlikely to worsen outcomes in infants with critical surgical conditions.
Our findings that crude mortality of neonates with CDH was lower in the transfer group, warrants an explanation. Majority of these infants were likely diagnosed postnatally; such infants are known to have lesser pulmonary hypoplasia probably due to late onset of herniation during gestation [95].
Advocacy for a wider adoption of co-located care approach is often met with challenges. Parental choices, need for staying away from home during the vulnerable antenatal period, travel and cost constraints, surgeons’ preferences and insurance coverage patterns are known to influence regionalization practices for surgical neonates [96–98]. Furthermore, the discordance in availability of maternal and neonatal care and a surge in satellite NICUs around surgical centres may drive referral practices [99]. In the US, local care protocols for surgical neonates have been reported to vary significantly across states and lack consistency with surgical subspecialty standards endorsed by the American Academy of Pediatrics [100]. Thus, surgical transfers will continue to remain an important issue for healthcare providers and policy makers.
The limitations of our study need to be acknowledged. These include the potential for confounding by indication. Risk-adjusted mortality was reported in only 26% of the studies. The high statistical heterogeneity in our meta-analysis warrants caution in interpreting our findings. It may relate to the case mix from a wide range of patient populations studied. It is reassuring to note that our findings remained unchanged after excluding studies published before the year 2000, a potential source of heterogeneity. Inadvertent overlap of patients is a common occurrence in evidence synthesis involving public health records [101] and cannot be ruled out. Limited information was available on the impact of surgical transport on long-term neurodevelopment.
In summary, our systematic review and meta-analysis shows that transfer from the birth hospital to a facility for surgical intervention was not associated with increased risk of death in neonates with critical surgical conditions. Limited data was available on long-term disability. Considering the difficulties in conducting RCTs in this field, the findings from our comprehensive and robust systematic review provide the best available evidence for informing clinicians, parents, and health policy makers.
Supporting information
S1 ChecklistPRISMA 2020 checklist.(DOCX)
S1 FileSearch strategy.(DOCX)
S1 TableAdditional study characteristics of included studies.(DOCX)
S2 TableCharacteristics of excluded studies.(DOCX)
S3 TableDefinition of co-located care and surgical transfer.(DOCX)
S4 TableOutcomes described in the systematic review.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta VS, Harting MT, Lally PA, Miller CC, Hirschl RB, Davis CF, et al. Mortality in Congenital Diaphragmatic Hernia: A Multicenter Registry Study of Over 5000 Patients Over 25 Years. Annals of Surgery. 2023;277(3):520–7.34334632 10.1097/SLA.0000000000005113 · doi ↗ · pubmed ↗
- 2Patel M, Yu S, Romano JC, Bates K, Uzark K, Schumacher K, et al. Birth Location in Infants with Prenatally Diagnosed Hypoplastic Left Heart Syndrome. Pediatr Cardiol. 2022;43(2):301–7.34668072 10.1007/s 00246-021-02721-y · doi ↗ · pubmed ↗
- 3Amer R, Moddemann D, Seshia M, Alvaro R, Synnes A, Lee K-S, et al. Neurodevelopmental Outcomes of Infants Born at <29 Weeks of Gestation Admitted to Canadian Neonatal Intensive Care Units Based on Location of Birth. J Pediatr. 2018;196:31-37.e 1. doi: 10.1016/j.jpeds.2017.11.038 29305231 · doi ↗ · pubmed ↗
- 4Lapcharoensap W, Gage SC, Kan P, Profit J, Shaw GM, Gould JB, et al. Hospital Variation and Risk Factors for Bronchopulmonary Dysplasia in a Population-Based Cohort. JAMA Pediatrics. 2015;169(2):e 143676.10.1001/jamapediatrics.2014.367625642906 · doi ↗ · pubmed ↗
- 5Lasswell SM, Barfield WD, Rochat RW, Blackmon L. Perinatal regionalization for very low-birth-weight and very preterm infants: a meta-analysis. JAMA. 2010;304(9):992.20810377 10.1001/jama.2010.1226 · doi ↗ · pubmed ↗
- 6Nezafat Maldonado B, Singhal G, Chow L, Hargreaves D, Gale C, Battersby C. Association between birth location and short-term outcomes for babies with gastroschisis, congenital diaphragmatic hernia and oesophageal fistula: a systematic review. BMJ Paediatr Open. 2023;7(1):e 002007. doi: 10.1136/bmjpo-2023-002007 37474200 PMC 10357737 · doi ↗ · pubmed ↗
- 7Granger CL, Mukherjee K, Embleton ND, Tinnion RJ, Berrington JE. Impact of Transfer for Surgical Management of Preterm Necrotising Enterocolitis or Focal Intestinal Perforation. J Pediatr Surg. 2023;58(10):1976–81. doi: 10.1016/j.jpedsurg.2023.03.016 37100685 · doi ↗ · pubmed ↗
- 8Paul S, Resnick S, Gardiner K, Ramsay JM. Long-distance transport of neonates with transposition of the great arteries for the arterial switch operation: A 26-year Western Australian experience. J Paediatr Child Health. 2015;51(6):590–4. doi: 10.1111/jpc.12782 25425073 · doi ↗ · pubmed ↗