The Rare Co-occurrence of Clostridioides difficile Infection and Pseudomonas Meningitis in an Infant: A Case Report
Ia Khurtsilava, Darejan Kanjaradze, Ekaterine Gozalishvili, Tamar Gachechiladze, Teimuraz Mikeladze

TL;DR
A five-month-old infant had rare co-infections of C. difficile and Pseudomonas meningitis, highlighting the importance of early diagnosis and treatment in infants.
Contribution
This case report emphasizes the rare but critical co-occurrence of CDI and Pseudomonas meningitis in infants and the need for prompt recognition.
Findings
The infant showed improvement after treatment for C. difficile but required further intervention for Pseudomonas meningitis.
Neuroimaging and lumbar puncture were essential for diagnosing Pseudomonas meningitis in this case.
Early and aggressive treatment improved outcomes despite the rare and complex infections.
Abstract
This case report presents a five-month-old infant who developed clinically manifested Clostridioides difficile (C. difficile) infection (CDI) and Pseudomonas aeruginosa (P. aeruginosa) meningitis. Initially diagnosed with pseudomembranous enterocolitis and treated with oral vancomycin, the child showed gastrointestinal improvement but continued to experience persistent fever, prompting further evaluation. Neuroimaging revealed ventriculomegaly, leading to a lumbar puncture that confirmed bacterial meningitis. Empiric antibiotics were initiated, and amikacin was added following CSF culture results that identified P. aeruginosa, resulting in significant clinical improvement. This report highlights the diagnostic challenges of P. aeruginosa meningitis in infants, particularly when complicated by secondary infections like CDI. Our objective is to raise awareness about the fact that although…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
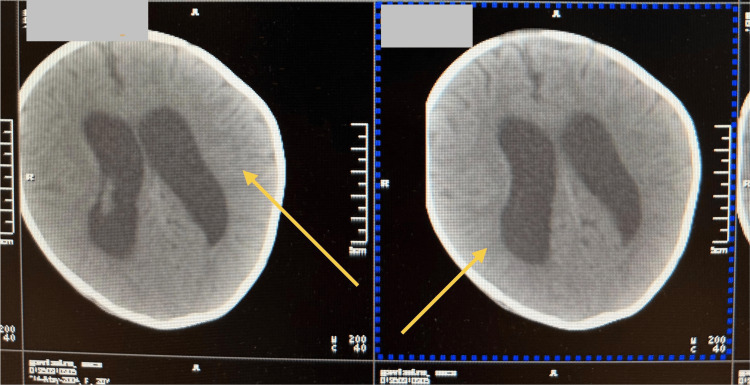 Figure 1
Figure 1| Test | Result | Reference range |
| Morning cortisol, nmol/L | 1152 | 171–536 |
| ALT, U/L | 36.3 | <60 |
| AST, U/L | 45.7 | <84 U/L |
| Creatinine, µmol/L | 34.2 | <80 |
| CRP, mg/L | 22.8 | <6 |
| 17-OH progesterone, ng/mL | 4.69 | 1.8-20.0 |
| Total protein, g/L | 52.0 | 66–87 |
| Albumin, g/L | 34.0 | 35–52 |
| Initial CBC | CBC before discharge | ||
| Parameter | Result | Result | Reference range |
| Hb, g/L | 91 | 102 | 110–140 |
| RBC, × 10¹²/L | 3.5 | 3.9 | 4.1–5.5 |
| PLT, × 10⁹/L | 544 | 339 | 150–450 |
| WBC, × 10⁹/L | 9.3 | 6.8 | 5.0–15.0 |
| Granulocytes, % | 54.4 | 26.3 | ~50–70 |
| Agranulocytes, % | 41.8 | 63.3 | ~30–50 |
| Monocytes, % | 3.8 | 10.4 | 2–10 |
| HCT, % | 28.1 | 32.2 | 33–39 |
| MCV, fL | 79.7 | 82.3 | 77–95 |
| RDW-CV, % | 14.4% | 15.6 | 11.5–14.5 |
| RDW-SD, fL | 46.7 | 52.0 | 37–54 |
| Initial CSF fluid | CSF fluid result after treatment | ||
| Parameter | Result | Result | Reference range |
| Color | Clear | Clear | Clear |
| Specific gravity | 1.015 | 1.015 | 1.006–1.007 |
| pH | 7.5 | 8.5 | 7.35–7.40 |
| Protein, g/L | 13.1 | 1.45 | 0.22–0.33 |
| Glucose, mmol/L | 0.863 | 1.49 | 2.8–3.9 |
| Cytosis | 1194 | 5 | <32 |
| Erythrocytes (RBCs), cells/µL | 10-12 | 1–2 | 0–5 |
| Leukocytes (WBCs), cells/µL | High | 8–9 | 0–5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Streptococcal Infections and Treatments · Botulinum Toxin and Related Neurological Disorders
Introduction
Bacterial meningitis is a severe and potentially fatal infection characterized by inflammation of the meninges, the protective membranes surrounding the brain and spinal cord [1]. It is a medical emergency requiring prompt diagnosis and immediate treatment to minimize morbidity and mortality. The causative bacterial pathogens vary by age group, with Group B Streptococcus being the most common in infants younger than two months, while Streptococcus pneumoniae is the leading cause in most other age groups. Among individuals aged 11 to 17 years, Neisseria meningitidis is the most frequently identified pathogen [1,2].
Gram-negative bacilli such as Klebsiella spp., Escherichia coli (E. coli), Enterobacter spp., and Pseudomonas aeruginosa (P. aeruginosa) are less common, with E. coli and P. aeruginosa being the most prevalent among them [1,2]. Nosocomial bacterial meningitis often results from invasive procedures, traumatic head injuries, and intraventricular catheters (IVS). Though rare, they are often associated with serious conditions and risk of complications, and high mortality rates. Diagnosis can be challenging, especially in small children, due to the absence of classical neuroinfection symptoms, leading to potential delays in treatment and worsening patient outcomes. Managing P. aeruginosa meningitis is also difficult due to the limited number of effective antimicrobial agents and their poor penetration through the blood-brain barrier.
Clostridioides difficile (C. difficile) infection (CDI) has traditionally been associated with adult and elderly populations, particularly those with recent antibiotic exposure or hospitalization. However, there is growing evidence that suggests that CDI is also a significant concern in pediatric patients, including young infants and children. While asymptomatic colonization with C. difficile is common in neonates, distinguishing between colonization and true infection remains a challenge [3,4]. This case report describes an infant who developed clinically manifested CDI, was successfully treated, and was later diagnosed with P. aeruginosa meningitis.
Case presentation
A five-month-old severely dehydrated child was brought to the pediatric emergency department. The mother reported that over the past few days, the child had experienced countless episodes of diarrhea, and their pediatrician had prescribed oral vancomycin (60 mg/day orally) after confirming the presence of C. difficile toxin. On examination, the child had bluish/purplish skin discoloration, dry and scaly mucous membranes, weak peripheral pulses, decreased skin turgor and elasticity, and a mildly sunken anterior fontanelle. The Pediatric Glasgow Coma Scale (PGCS) score was 8. The vital signs were as follows: heart rate (HR): 174 bpm; respiratory rate (RR): 62 breaths per minute; SpO₂: 81%; blood pressure (BP): 47/28 mmHg; capillary refill time (CRT): six seconds; temperature (T): 38.4°C; and weight: 4800 grams.
The child’s condition was assessed as hypovolemic shock, and immediate fluid resuscitation was initiated. Initial blood gas and electrolyte analysis revealed severe acidemia and significant electrolyte imbalances (venous PH: 6.9, NA: -168, K: 3.5, Cl: 127). Despite multiple fluid boluses, the patient remained hemodynamically unstable, prompting the initiation of a dobutamine infusion, and the patient was switched to mechanical ventilation. Initial laboratory tests were performed on the day of admission and the next morning (Tables 1, 2). History revealed that over the past three months, the patient had experienced multiple episodes of fever requiring hospitalization with various diagnoses, including pertussis, bronchiolitis, and sepsis. During these hospital stays, broad-spectrum antibiotics were administered. Four days ago, the family had deliberately left the pediatric clinic and consulted their pediatrician, who ordered a C. difficile toxin test. The patient was subsequently diagnosed with pseudomembranous enterocolitis.
The day of admission to our clinic marked the 14th day of persistent fever and diarrhea. No blood or mucus was present in the stool during admission. Blood cultures were negative, and no evidence of systemic bacterial infection or endocrine causes of the electrolyte imbalance was found. Neurological infection remained a concern despite the absence of classical signs and symptoms. Initially, lumbar puncture was deferred due to the patient's hemodynamic instability, and subsequently, the parents repeatedly refused to give consent for the procedure. There was some clinical improvement, the stool pattern normalized, and the child began to eat adequately; however, the patient’s condition remained concerning. Episodes of fever persisted. Oral vancomycin was discontinued.
Neuroimaging (neurosonoscopy) revealed ventriculomegaly (anterior horn width D: 14.07 mm, S: 12.84 mm). CT scan of the head also documented ventriculomegaly (Figure 1). After several conversations, the parents ultimately agreed to give their consent for a lumbar puncture (Table 3). The procedure confirmed bacterial meningitis. Empirical antibiotic treatment for meningitis was initiated with vancomycin (60 mg/kg/day) and meropenem (40 mg/kg/day). CSF culture grew P. aeruginosa 10^5 CFU/ml. Amikacin (21 mg/kg/day) was added to the treatment regimen.
CT of the head showing ventriculomegalyCT: computed tomography
Antibiotic therapy was continued for 21 days, and a repeat lumbar puncture showed no abnormalities and no bacterial growth. During the antibiotic course, the patient became afebrile within 48 hours and showed marked clinical improvement. The patient was discharged with a follow-up visit scheduled in two weeks. At the follow-up visit, the child had no complaints, was feeding well, with normal stool and urination patterns. No neurological deficits were observed, though a mild developmental delay was noted. Four months after discharge, the parents contacted us and informed us that minimally invasive neurosurgery had been performed due to hydrocephalus. Otherwise, the child is doing well, with no significant complaints. The child is developing normally, gaining weight adequately, and has no neurological deficits.
Discussion
CDI in infants presents a diagnostic and therapeutic challenge due to the high rates of asymptomatic colonization in infants and the immature gut receptor expression, which may confer reduced sensitivity to C. difficile toxins [3,4]. We discussed a case of a five-month-old infant who developed severe diarrhea and dehydration following previous hospitalizations and multiple courses of broad-spectrum antibiotics, eventually being diagnosed with pseudomembranous enterocolitis. This aligns with the findings of Li et al., who reported a similar pattern in a one-month-old infant developing symptomatic CDI after extensive antibiotic exposure [3].
CDI in infants is often overlooked or misattributed to other causes due to its rare symptomatic manifestation and overlapping clinical signs with other gastrointestinal disorders. However, the presence of persistent diarrhea, clinical deterioration, and a positive C. difficile toxin assay in our patient supported the diagnosis of true infection rather than colonization. As in the case report by Tibesar, our patient was diagnosed with pseudomembranous colitis, supporting the concept that CDI, while rare, can indeed manifest in neonates and infants and should not be dismissed solely due to age [4]. Further complicating the clinical picture, the patient in this case also developed P. aeruginosa meningitis. P. aeruginosa meningitis in pediatric patients is exceedingly rare, as outlined by Cotran-Lenrow et al., who reported a case of community-acquired infection in a child without prior neurosurgical intervention [1,2]. Although the exact origin in our case remains unidentified, the possibility of nosocomial colonization followed by hematogenous spread cannot be excluded, especially in the setting of prolonged antibiotic therapy and compromised mucosal barriers.
Diagnosis of bacterial meningitis in infants is particularly challenging due to nonspecific symptoms and the difficulty in performing lumbar punctures in critically ill patients. In our case, diagnostic delay occurred due to both clinical instability and parental hesitancy regarding invasive procedures. Nonetheless, neuroimaging findings prompted re-evaluation, and CSF culture eventually confirmed P. aeruginosa as the causative pathogen. This shows the importance of staying alert and being persistent in diagnostic efforts, even when the usual signs of meningitis are absent. Management of P. aeruginosa meningitis is complicated by the pathogen’s inherent resistance to many antibiotics and poor CNS penetration of most effective agents. The successful use of amikacin in our case contributed to clinical recovery, emphasizing the importance of targeted therapy based on culture and sensitivity results. The resolution of infection and favorable short-term outcome following a 21-day antibiotic course further highlight the importance of individualized, aggressive management strategies.
Conclusions
This report emphasizes the rarity and diagnostic challenges associated with CDI and P. aeruginosa meningitis in infants, particularly in those with prior antibiotic exposure and repeated hospitalizations. While CDI is typically associated with adults, infants can develop clinically significant infections, despite often having asymptomatic colonization. Furthermore, although extremely rare, infants may also develop meningitis caused by uncommon pathogens. Lastly, the report highlights the importance of prudent antibiotic use in pediatric populations to prevent both CDI and nosocomial infections like those related to P. aeruginosa.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Community-acquired Pseudomonas aeruginosa meningitis in a pediatric patient Cureus Cotran-Lenrow A Tefera LS Douglas-Vail M Ayebare A Kpokpah LN Davis BP 015202310.7759/cureus.42376 PMC 1044554937621787 · doi ↗ · pubmed ↗
- 2Case report: a domestic sponge brush used to clean a milk feeding bottle: the source of neonatal meningitis caused by Pseudomonas aeruginosa Front Pediatr Mizuno S Matsuzaki S Yokoyama K Hamahata K Yoshida A 725940920213463162310.3389/fped.2021.725940 PMC 8495192 · doi ↗ · pubmed ↗
- 3Clostridioides difficile infection in infants: a case report and literature review Gut Pathog Li Z Dong N Hao J 311520233738661210.1186/s 13099-023-00552-1PMC 10311876 · doi ↗ · pubmed ↗
- 4Clostridium difficile infection in a very young infant with pseudomembranous colitis noted on endoscopy Case Rep Gastroenterol Tibesar E 5225261420203325069210.1159/000508916 PMC 7670329 · doi ↗ · pubmed ↗