Comparative efficacy and safety of two radiotherapy protocols for ovarian ablation in patients with metastatic breast cancer
Tasneem Hossain, Erika Galietta, Alessio G. Morganti, Abul Farah Md. Kamal Uddin, Shahida Alam, Altaf Hossain, Sonya Begum, Qazi Mushtaq Hussain, Nowshin Taslima Hossain

TL;DR
This study compared two radiotherapy protocols for ovarian ablation in metastatic breast cancer patients and found both to be equally effective and safe.
Contribution
The study provides evidence that shorter and more flexible radiotherapy regimens are viable for ovarian ablation in resource-limited settings.
Findings
Both RT regimens achieved similar rates of amenorrhea and postmenopausal hormone levels.
No grade ≥3 toxicity was observed in either treatment group.
Common postmenopausal symptoms like hot flushes were similar between the two arms.
Abstract
The present study aimed to evaluate the efficacy and safety of radiotherapy (RT) for ovarian ablation (OA) in patients with metastatic breast cancer by comparing two RT protocols: 15 Gy in 5 fractions (arm A) vs. 20 Gy in 10 fractions (arm B). For this purpose, the present study enrolled 68 patients, divided equally into two study arms. The patients were followed-up for 24 weeks post-intervention. The primary endpoint was the efficacy of RT in inducing OA, assessed through amenorrhea and hormone levels [follicle-stimulating hormone (FSH) and estradiol]. Toxicities were evaluated using the Common Toxicity Criteria for Adverse Events version 5.0, and post-menopausal symptoms were assessed using the Menopause Rating Scale. The results revealed that there was no significant difference between the two study arms (A vs. B) in the rate of amenorrhea development and persistence (85.7 vs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
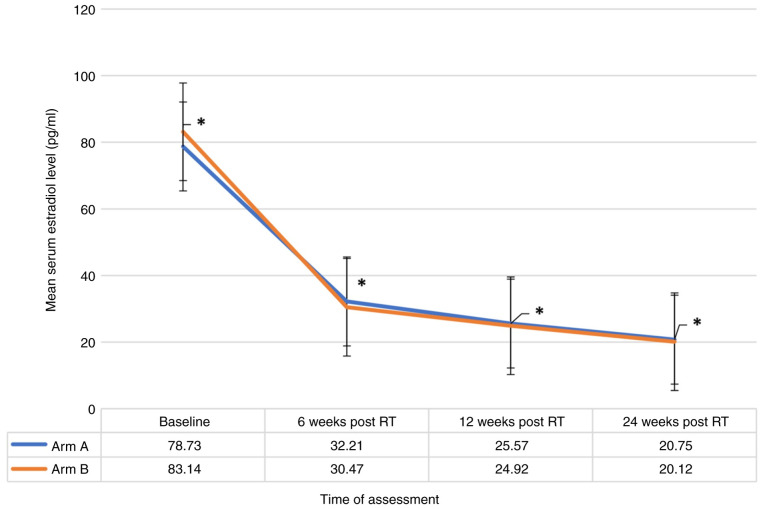 Figure 1
Figure 1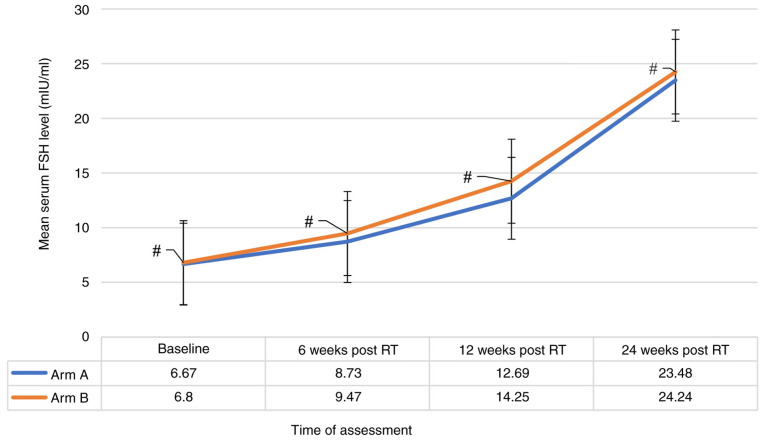 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound and Hyperthermia Applications · Ovarian cancer diagnosis and treatment · Reproductive Biology and Fertility
Introduction
Breast cancer (BCa) remains one of the most prevalent tumors affecting women worldwide. According to the World Cancer Research Fund, BCa is the most commonly occurring type of cancer among women and the second most common type of cancer overall, with over two million new cases recorded in 2018(1). In particular, the incidence rate of BCa in Bangladesh according to GLOBOCAN is 105.6 per 100,000 individuals per year (2). This high incidence rate implies the importance of effective treatment modalities.
Ovarian ablation (OA), a critical therapeutic approach, particularly in hormone-receptor-positive metastatic BCa, functions by reducing estrogen production. In fact, estrogen plays a crucial role in the proliferation of hormone-receptor-positive BCa cells. OA can be achieved through several methods: Surgical oophorectomy, radiation-induced OA or pharmacological agents, leading to ovarian suppression. Each method has its distinct mechanisms and implications (3).
Radiotherapy (RT), as a means of OA, has been used for a number of decades due to its non-invasive nature and potential efficacy. RT involves the application of ionizing radiation to the ovarian tissue, leading to follicular destruction and consequently, estrogen deprivation. Moreover, RT is often preferred for OA in low-middle-income countries (LMICs) due to its cost-effectiveness, particularly in comparison to surgical methods or hormonal treatments, such as luteinising hormone-releasing hormone analogs. In fact, RT provides a practical alternative in settings where medical or surgical facilities are limited, reducing the need for postoperative care. Additionally, the simplicity and one-time expense of RT make it more feasible and financially viable for both healthcare systems and patients in resource-constrained environment.
However, the lack of clear guidelines on the optimal dose and fractionation of RT poses challenges. The variability in practice and the absence of a standardized protocol underscore the need for comparative studies (3). Given this background, the present study aimed to compare two different RT protocols for OA in patients with metastatic BCa: A dose of 15 Gy delivered in 5 fractions vs. 20 Gy in 10 fractions. The present comparative analysis is intended to provide clearer insight into the efficacy and safety of these protocols, potentially guiding future clinical practice and standardizing treatment approaches.
Patients and methods
Study design and setting
The present study was conducted at the Department of Radiation Oncology, National Institute of Cancer Research and Hospital, Dhaka, Bangladesh, from September 30, 2021 to June 30, 2022. The study aimed to evaluate the efficacy and safety of RT for OA in patients with metastatic BCa. The present study was conducted according to the guidelines of the Declaration of Helsinki and was approved by Ethics Committee of the National Institute of Cancer Research and Hospital, Dhaka, Bangladesh (NICRH/Ethics/2021/280; dated September 30, 2021). Written informed consent was obtained from all subjects involved in the study.
Patient selection
A total of 68 patients were enrolled in the study, with 34 patients allocated to each study arm by purposive sampling. The inclusion criteria were the following: Premenopausal female patients with a confirmed diagnosis of hormone-receptor-positive, Her-2 negative metastatic BCa, for whom OA was deemed clinically necessary. The exclusion criteria included patients who were in visceral crisis, or who had previous history of ovarian surgery or pelvic RT, or had received chemotherapy within the past 1 year of the study, or those with pre-existing conditions affecting ovarian function.
Operational definitions
Patients were considered hormone receptor-positive in the present study if, in available immunohistochemical reports performed at another laboratory, they had ≥10% estrogen receptor (ER)- or progesterone receptor (PR)-positive cells. Female patients were deemed to be premenopausal and included in the present study if they had: i) A normal menstrual period within 2 months clinically; or ii) a normal menstrual period within the past 12 months, with serum follicle-stimulating hormone (FSH) and estradiol levels within the premenopausal range. Patients were considered to have developed amenorrhea if they had experienced an absence of menstruation for 3 consecutive months without any subsequent resumption. Serum FSH levels >22 mIU/ml and estradiol levels <30 pg/ml were used as criteria for postmenopausal hormone levels to observe the response. The Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 was used to evaluate radiation-induced toxicities (4). Postmenopausal symptoms were assessed using the standardized Menopause Rating Scale (MRS), which measures health-related quality of life regarding 11 symptoms related to the menopause transition. The presence of a visceral crisis, considered as an exclusion criterion for the study, was defined as extensive visceral metastasis with profound symptomatic involvement, such as lymphangitis carcinomatosis, bone marrow replacement, lung metastases with severe symptoms, carcinomatous meningitis, significant liver metastasis, or a rise in liver function markers to three times above the upper limit.
RT technique
The RT technique employed was two-dimensional (2D) radiation therapy. For treatment, patients were positioned in a supine position on the treatment table, and radiopaque markers were utilized to outline the pelvic region. Anteroposterior and posteroanterior pelvic fields were designed to fully encompass the ovaries. The delineation of field borders included the following: The inferior border was set at the lower border of the obturator foramen; superiorly, it extended to the inferior sacroiliac joint; and laterally, it was placed 1.5 cm beyond the true pelvic brim. To ensure precise ablation, the localization of the ovaries was verified using ultrasonography. Of note, two different dosing regimens were prescribed for the present study: Arm A received a total dose of 15 Gy, delivered in 5 fractions over the course of 1 week, while arm B was administered 20 Gy in 10 fractions spread over a period of 2 weeks, with treatments administered on consecutive days.
Assessment of efficacy
The primary endpoint was the efficacy of RT in inducing OA, assessed by the development and persistence of amenorrhea and the attainment of postmenopausal levels of FSH and estradiol. These hormonal levels were measured prior to the commencement of RT and then at 4, 12, and 24 weeks post-RT.
Statistical analysis
Data were analyzed using appropriate statistical methods to compare the efficacy and safety profiles of the two RT regimens. The primary comparative analysis focused on the rate of OA, while secondary analyses included the assessment of radiation-induced toxicities and menopausal symptoms. The statistical method used was the inferential statistical analysis (Hypothesis testing). Analyses were performed using a two-way mixed ANOVA test followed by the Bonferroni post hoc test and independent t-test for continuous variables and the Chi-squared test and Fisher's exact test for categorical variables. For associations, the Chi-squared test of independence was used. All reported P-values were two-sided and P-values <0.05 were considered to indicate statistically significant differences. As statistical software, IBM SPSS software version 25.0 for windows (IBM SPSS Statistics for Windows, version 25.0; IBM Corp.) was used.
Results
Efficacy of RT in OA
The patient characteristics are detailed in Table I. In evaluating the efficacy of RT for OA, the present study found no significant differences between arm A (15 Gy in 5 fractions) and arm B (20 Gy in 10 fractions). The rate of development and persistence of amenorrhea was comparable between the two arms, with 85.7% in arm A and 89.5% in arm B (P-value, not significant), excluding 28 (41.17%) patients who had pre-RT amenorrhea with premenopausal hormonal levels. Similarly, the achievement of postmenopausal estradiol levels exhibited no significant differences between the groups, being 91.2% in arm A and 94.1% in arm B (P-value, not significant). The rate of attainment of postmenopausal FSH levels was also similar, with 79.4% in arm A and 88.2% in arm B (P-value, not significant) (Table II). A significant reduction (P-value <0.001) in the mean estradiol level in all the patients included in both groups across all four time points was observed (Fig. 1), alongside a notable consistent significant increase in the mean FSH level at all four points (P-value <0.001) (Fig. 2). However, these changes were not significantly different between the two treatment groups when compared at baseline, 6 weeks, 12 weeks and at 24 weeks indicating that both groups followed a similar pattern of estradiol and FSH levels (Figs. 1 and 2). Additionally, there was no strong evidence of a difference in the mean estradiol (P=0.856) and mean FSH (P=0.056) levels between the two groups.
Factors influencing efficacy of OA
The analysis revealed that a younger age (<36 years), a higher body mass index (BMI), elevated baseline estradiol levels, and the absence of prior chemotherapy were significantly associated with a failure to achieve OA (P<0.05). These findings suggest that patient-specific characteristics play a crucial role in the response to RT for OA (Table III, Table IV, Table V and Table VI).
Toxicity and postmenopausal symptoms
As regards safety, the treatment was well tolerated in both arms. No grade ≥3 radiation induced toxicities were observed. The most common postmenopausal symptoms reported by the patients in both study arms were hot flushes and irritability, with no significant difference in their incidence or severity between the two treatment groups (Tables VII and VIII).
Discussion
The present study aimed to assess the efficacy and safety of RT for OA in patients with metastatic BCa. It primarily investigated the role of RT in inducing OA, assessed through the development and persistence of amenorrhea, and the attainment of postmenopausal levels of FSH and estradiol within 24 weeks of treatment. Using a 2D RT technique, 68 patients were treated with one of two different dose regimens: 15 Gy delivered in 5 fractions (arm A) or 20 Gy delivered in 10 fractions (arm B). The tolerability of these protocols treatments was measured through the CTCAE version 5.0 for radiation-induced toxicities, and the MRS for evaluating post-menopausal symptoms.
The results indicated no significant differences between the two arms in terms of the rate of amenorrhea development, and the achievement of postmenopausal estradiol and FSH levels. In fact, both groups demonstrated a significant decrease in mean estradiol levels and an increase in mean FSH levels compared to baseline, without significant differences between the groups. Furthermore, a younger age, a higher BMI, a high estradiol level, and the absence of prior chemotherapy were significantly associated with the failure to achieve OA. Notably, the study observed no grade ≥3 toxicity, and the most common postmenopausal symptoms were hot flushes and irritability, with no significant differences between the study arms.
The results of the present study can be compared with those of previous studies. In the meta-analysis by Asiri et al (5), the efficacy of RT-induced OA was assessed in terms of amenorrhea rates, progression-free survival and overall survival. Their study concluded that RT-OA was effective, with doses of 15 Gy in 5 fractions, 15 Gy in 4 fractions, 16 Gy in 4 fractions, and 20 Gy in 10 fractions demonstrating high amenorrhea rates (5). Comparatively, the present study used doses of 15 Gy in 5 fractions and 20 Gy in 10 fractions, aligning closely with two regimens evaluated in the aforementioned meta-analysis. Both studies found no significant differences in the efficacy of OA between different dose regimens, suggesting that a lower dose may be sufficient for effective OA.
In their retrospective evaluation, Bese et al (6) reported a high rate of amenorrhea (96%) with various doses ranging from 5 Gy in a single fraction to 36 Gy in 18 fractions. Their study did not report any severe acute or late complications attributable to RT (6). This aligns with the findings of the present study, where no significant difference in amenorrhea rates was observed between the two study arms, and no severe toxicity was noted. The broad range of doses used in the study by Bese et al (6) suggests a potential for flexibility in dosing without compromising the efficacy of OA.
Hughes et al (7) reported 75% successful OA using a dose of 20 Gy in 10 fractions, with no reported grade 3 or 4 toxicities. This is consistent with the findings of the present study. In fact, both analyses highlight the relatively low toxicity profile of RT-OA, supporting its safety and tolerability. One of the most notable aspects of the present study is its setting in a LMIC, distinct from the majority of prior studies conducted predominantly in high-income countries (8-12).
In fact, the effectiveness and tolerability of medical therapies, including OA, can be greatly influenced by the treatment setting. This is particularly true in LMICs, where unique challenges, such as the prevalence of specific comorbidities, issues related to malnutrition and the utilization of less advanced medical technologies, including obsolete RT techniques, could potentially affect the outcomes of such treatments. These factors may influence not only the efficacy of the treatment, but also its tolerability, patient compliance and overall outcomes.
Despite these potential limitations, the present study achieved results consistent with those obtained in high-income settings (8-12). This finding is crucial, as it suggests that OA, even when conducted under the constraints typical of a LMIC setting, can be effective and well-tolerated. This is significant, particularly in the context of resource-limited healthcare environments, where access to the latest medical technologies and treatments is often challenging. Moreover, in Bangladesh, radiotherapy-induced ovarian ablation (RT-induced OA) can be performed at a cost as low as 1,200 required for 2 years of ovarian suppression using hormonal agents, or the $600 needed for surgical oophorectomy.
Furthermore, as demonstrated herein, the equivalence in the efficacy of OA administered in 5 sessions, as opposed to 10, holds particular importance in low resource settings. In fact, the scarcity of RT equipment in a number of LMICs often leads to extended waiting lists. Therefore, a shorter treatment regimen not only reduces the burden on healthcare resources, but also improves patient access to timely treatment and compliance to the prescribed treatment. This can be a critical factor in the management of metastatic BCa, where timely intervention can significantly impact patient outcomes and quality of Life.
In conclusion, the findings of the present study not only align with international research (5-7) but also extend its applicability to LMIC contexts. They underscore the potential for adapting and optimizing cancer treatment protocols in resource-limited settings, thereby enhancing the global equity in cancer care.
The present study, while providing key insight into the efficacy of OA using RT, had certain limitations that need to be mentioned. The small sample size and the specific demographic characteristics of the participants may affect the generalizability of the findings to a broader population. Another constraint was the short follow-up period, which limited the authors' ability to assess long-term efficacy in terms of persistence of clinical and hormonal response as well as survival and also late-onset toxicities. Furthermore, being a quasi-experimental study, there may be inherent biases in data collection and analysis methods, potentially affecting the reliability of the results.
On the other hand, the present study also had several strengths. It highlighted the feasibility of a shorter treatment regimen, potentially useful in reducing treatment wait times and improving patient access to care. Moreover, the assessment approach, using both clinical and biochemical markers, provided a comprehensive understanding of the treatment impact. Notably, the safety profile of the treatment regimens using conventional 2D technique was a key finding, with no severe toxicities reported in either treatment arm. This aspect is particularly significant in the settings of metastatic BCa, where patient tolerance and quality of life are paramount.
In summary, while the present study has some limitations typical of quasi-experimental designs, its strengths lie in its practical applicability, comprehensive outcome assessment, and demonstrated safety profile.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arnold M Morgan E Rumgay H Mafra A Singh D Laversanne M Vignat J Gralow JR Cardoso F Siesling S Soerjomataram I Current and future burden of breast cancer: Global statistics for 2020 and 2040 Breast 661523202210.1016/j.breast.2022.08.01036084384 PMC 9465273 · doi ↗ · pubmed ↗
- 2Ferlay J Ervik M Lam F Laversanne M Colombet M Mery L Piñeros M Znaor A Soerjomataram I Bray F Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer, Lyon, 2024. Available from: https://gco.iarc.who.int/today. Accessed March 2, 2024.
- 3Celio L Bajetta E Toffolatti L Catena L Beretta E Buzzoni R Ovarian ablation for premenopausal early-stage breast cancer: An update Tumori 86191194200010.1177/03008916000860030210939596 · doi ↗ · pubmed ↗
- 4Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0. Published November 27, 2017. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v 5_Quick_Reference_5x 7.pdf.
- 5Asiri MA Tunio MA Abdulmoniem R Is radiation-induced ovarian ablation in breast cancer an obsolete procedure? Results of a meta-analysis Breast Cancer (Dove Med Press)8109116201610.2147/BCTT.S 9461727307764 PMC 4887042 · doi ↗ · pubmed ↗
- 6Bese NS Iribas A Dirican A Oksuz D Atkovar G Ober A Ovarian ablation by radiation therapy: Is it still an option for the ablation of ovarian function in endocrine responsive premenopausal breast cancer patients?Breast 18304308200910.1016/j.breast.2009.09.00519800233 · doi ↗ · pubmed ↗
- 7Hughes LL Gray RJ Solin LJ Robert NJ Martino S Tripathy D Ingle JN Wood WC Eastern Cooperative Oncology Group; Southwest Oncology Group et al Efficacy of radiotherapy for ovarian ablation: Results of a breast intergroup study Cancer 101969972200410.1002/cncr.2048115329905 · doi ↗ · pubmed ↗
- 8Boccardo F Rubagotti A Perrotta A Amoroso D Balestrero M De Matteis A Zola P Sismondi P Francini G Petrioli R Ovarian ablation versus goserelin with or without tamoxifen in pre-perimenopausal patients with advanced breast cancer: Results of a multicentric Italian study Ann Oncol 5337342199410.1093/oxfordjournals.annonc.a 0588378075030 · doi ↗ · pubmed ↗