Individual Cortisol Production in Active Rheumatoid Arthritis Associates with Treatment Responses: A Pilot, Two-Year Study
Maria G. Filippa, Maria P. Yavropoulou, Nikolaos I. Vlachogiannis, George E. Fragoulis, Aimilia Mantzou, Aggeliki Papapanagiotou, Maria G. Tektonidou, George P. Chrousos, Petros P. Sfikakis

TL;DR
This study found that lower cortisol production in active rheumatoid arthritis patients may predict poor treatment responses over two years.
Contribution
The study introduces a potential biomarker for predicting long-term treatment outcomes in rheumatoid arthritis.
Findings
Lower baseline diurnal cortisol production predicted inadequate treatment responses in RA patients.
A cortisol production threshold of 81.3 predicted remission with 86% specificity and 65% sensitivity.
Cortisol/ACTH ratio and diurnal cortisol levels were significantly lower in non-responders compared to remitters.
Abstract
Inadequate production of cortisol in relation to increased demands of chronic inflammation, a phenomenon coined as the “disproportion-principle”, occurs in some patients with active rheumatoid arthritis (RA). Moreover, relatively lower diurnal cortisol production prior to antirheumatic treatment initiation/escalation for active RA has been associated with inadequate corresponding treatment responses after 6-months. To evaluate whether individual levels of endogenous cortisol in active RA patients followed in an Academic Rheumatology Unit may predict the type of response to subsequent antirheumatic treatment regimens after two years. We measured morning circulating ACTH, cortisol and DHEAS blood levels, as well as saliva diurnal-cortisol levels (collected samples at 08:00, 12:00, 18:00, 22:00), prior to treatment initiation/escalation in RA patients with active disease. In a pilot…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
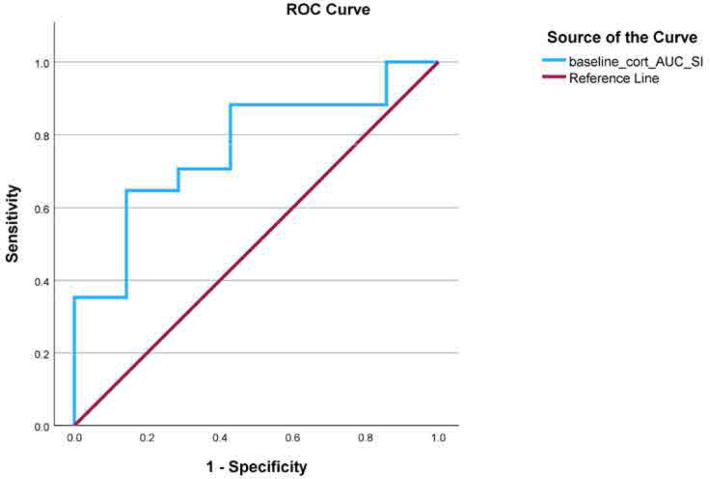 Figure 1
Figure 1|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 4.2 | 6.0 | no |
| 5115 |
|
| ● ● | No |
| Case 2 | 4.2 | 3. 8 | no |
| 540 |
| Yes | ||
| Case 3 | 5.7 | 3.2 | moderate |
| 563 |
| Yes | ||
| Case 4 | 5.7 | 4.4 | moderate |
| 1072 |
| No | ||
| Case 5 | 5.5 | 3.8 | moderate | - | 0 |
| ● ● ● |
| NA |
| Case 6 | 5.0 | 3.8 | moderate |
| 1288 | ● ● | ● ● | Yes | |
| Case7 | 4.2 | 3.2 | moderate | - | 0 | ● ● ● | NA | ||
| Case 8 | 4.1 | 1.4 | good |
| 2250 | ● ● | No | ||
| Case 9 | 6.0 | 2.5 | good |
| 2294 | No | |||
| Case 10 | 5.2 | 1.9 | good |
| 3196 |
| ● ● | No | |
| Case 11 | 4.8 | 2.5 | good |
| 3674.5 | ● ● | No | ||
| Case 12 | 6.6 | 2.3 | good | - | 0 |
|
| NA | |
| Case 13 | 4.2 | 1.9 | good |
| 516 |
| Yes | ||
| Case 14 | 6.4 | 2.0 | good |
| 573 |
|
| Yes | |
| Case 15 | 7.1 | 2.4 | good |
| 520 |
|
| Yes | |
| Case 16 | 4.0 | 2.5 | good |
| 417 |
| Yes | ||
| Case 17 | 6.0 | 1.8 | good |
| 747 | ● ● | Yes | ||
| Case 18 | 6.6 | 1.8 | good |
| 731 |
|
| Yes | |
| Case 19 | 4.4 | 1.7 | good |
| 620 |
| Yes | ||
| Case 20 | 5.2 | 1.8 | good |
| 250 | ● ● | ● ● |
| Yes |
| Case 21 | 6.2 | 1.8 | good |
| 255 |
| Yes | ||
| Case 22 | 7.2 | 1.5 | good |
| 148 |
|
| Yes | |
| Case 23 | 6.2 | 2.5 | good | 0 | ● ● | NA | |||
| Case 24 | 5.9 | 2.0 | good |
| 1187 |
| Yes |
|
|
|
|
|
|---|---|---|---|
|
| 13/17 | 7/7 | 0.283 |
|
| 56.7 ± 11.7 | 55 ± 11 | 0.747 |
|
| 83± 120 | 52.9±52.1 | 0.494 |
|
| 8/17 | 3/7 | 1.000 |
|
| 37.7± 42 (0.5–153) | 8.10 ± 7.7 (1.75–25) | 0.087 |
|
|
|
|
|
|
| 3.9± 3.1 | 3.2± 1.4 | 0.964 |
|
|
|
|
|
|
| 105.1 ± 49.1 | 69.7 ± 20.4 | 0.047 |
|
| 3.7 ± 3.0 | 3.8 ± 3.0 | 0.977 |
|
| 16.4 ± 8.3 | 14.2 ± 7.1 | 0.418 |
|
| 6.3± 3 | 4.3 ± 1.7 | 0.166 |
|
| 5 ± 4.1 | 2.6 ± 1.9 | 0.065 |
|
| 4.5± 3.4 | 2.4 ± 4.5 | 0.114 |
|
| 99± 42 | 68 ± 19 |
|
|
| 10/17 (58.8%) | 3/7 (42.9%) | 0.659 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal Hormones and Disorders · Stress Responses and Cortisol
INTRODUCTION
The efficacy of glucocorticoids (GC) in the management of rheumatoid arthritis (RA) and their beneficial effect on tissue damage was established through high-quality trials since late 50s.^1–4^ More recent longer-term follow-up studies have also shown that decreased progression of joint damage is maintained even after the glucocorticoid treatment has been discontinued.^5,6^ The most recent recommendations for the management of RA by the European Union Against Rheumatism (EULAR) acknowledge the fact that long-term administration of even low-dose glucocorticoids is frequently necessary to maintain clinical remission, even with the introduction of highly effective agents, such as the conventional disease-modifying anti-rheumatic drugs (cDMARDs), and biologics (b) or targeted-synthetic (ts) DMARDs.^7^
A compromised adrenocortical response to stress and inflammation, termed as “relative” or “functional” adrenal insufficiency has been previously described in some patients with RA, even in the absence of prior clinical and/or biochemical evidence of overt adrenal insufficiency,^8–13^ coined as the ‘disproportion principle’. As a result, endogenous adrenal cortisol production may be insufficient considering the increased clinical needs associated with the systemic inflammatory response, in at least a subset of patients with RA.^11,14,15^ Notably, both basal cortisol levels and time-integrated cortisol response to tetracosactide stimulation (Synacthen test) are significantly lower, compared to healthy controls, in patients with chronic inflammatory rheumatic diseases, who, while being in long-term remission with DMARDs combined with very low-dose GC, relapse upon discontinuation of GC, in the absence of adrenal insufficiency.^16^
In the current lack of relevant biomarkers with a predictive role for response to antirheumatic treatment in patients with RA we have previously shown that low basal morning saliva cortisol (<13.9 nmol/L) can predict inadequate clinical response after 6 months of treatment with 75% sensitivity and 92% specificity in a real-world clinical setting.^17^ However, the long-term potential predictive value of low cortisol levels concerning the clinical trajectory of rheumatoid arthritis has yet to be elucidated. Along these lines, herein we report the results of a pilot study to further investigate the relationship between baseline cortisol levels and clinical outcomes in rheumatoid arthritis over an extended period of 2 years.
PATIENTS AND METHODS
The present study is a follow-up of our single-centre, prospective cohort study, conducted at the Rheumatology Unit of the first Department of Propaedeutic and Internal Medicine, of the Medical School, National and Kapodistrian University of Athens.^17^ The protocol was approved by the scientific committee of “Laiko” General Hospital (E. Σ 38/21-01-2021) and was registered in ClinicalTrials.gov (NCT05671627). Our 6 months results have been previously published. ^17^
Patients with RA fulfilling the 2010 American College of Rheumatology (ACR)/EULAR classification criteria^18^ with moderate/high disease activity (28-joint Disease Activity Score (DAS28)-ESR/CRP >3.2)^19,20^ had been initially enrolled. Patients who continued their follow-up in our academic centre up to 24 months from baseline are included in the present analysis. All patients were treated as per clinician’s judgement with any combination of cDMARDs, b/ts DMARDS, and glucocorticoids (≤15mg/day of prednisolone or equivalent) following the EULAR recommendations for RA management (2019 update).^21^
All of the core set variables were evaluated for each patient [i.e., swollen joint count (SJC), tender joint count (TJC), patient’s global assessment (PtGA), C reactive protein (CRP) and erythrocyte sedimentation rate (ESR)] and a DAS28–score was calculated. Response to treatment was based on the EULAR response criteria that classify patients as good, moderate, or non-responders, using the individual amount of change in DAS-28 and the level (low, moderate, or high) of DAS-28 reached.^22–24^
Remission was defined based on the Boolean 2.0 criteria (i.e., each of the 3 core set variables TJC, SJC, CRP (in mg/dl) must have a value of ≤1, and a PtGA cut-off of 2 cm).^25^ Complete medical history, current medication, and history of GC withdrawal were obtained from the Patient’s database in compliance with the General Data Protection Regulation policy of the hospital.
Sampling procedures and measurements
At baseline, blood was obtained from RA patients at morning hours (8.00am) after an overnight fast, for the measurement of plasma adrenocorticotropic hormone (ACTH), serum C-reactive protein (CRP) and serum cortisol, as previously described.^17^Serum dehydroepiandrosterone sulphate (DHEAs) (μmol/L) was also retrospectively measured from stored serum samples, using an electrochemiluminescence ECLIA on cobas® e immunoassay analyser (reference values are given stratified by age).Saliva samples were obtained from patients with RA the next day at prescheduled time points, namely at 08:00, 12:00, 18:00 and 22:00, also as previously described.^17^
Statistical analysis
Shapiro–Wilk’s test was used to assess for normality of distributions and continuous variables are presented as mean ± standard deviation (SD). Differences in continuous variables between groups were assessed by independent samples t-test or the non-parametric Mann Whitney U test, when appropriate; categorical variables were assessed by two-tailed Fisher’s exact test. Serial measurements of saliva cortisol during the day were used to calculate the area under the curve (AUC) by integrating the values of the saliva cortisol over the prespecified time points (8.00-12noon–6pm-10pm). Time-integrated daily cortisol production was then calculated employing the integrated area under the curve using the trapezoidal method.^26^ Since AUC was calculated by integrating the values of the saliva cortisol over the prespecified time-range, saliva cortisol units were cancelled out and therefore AUC is expressed as a numerical value without any associated units.
We employed receiver operator characteristic (ROC) curve analysis to evaluate the predictive ability of baseline time integrated daily saliva cortisol production (AUC)to distinguish RA patients who attained treatment -induced remission at 24 months from those who did not. Logistic regression was used to examine the association between time-integrated cortisol production (below the ROC-defined cut-off value) at baseline and remission at 24 months while controlling for potential confounding effects of age, sex, and CRP levels at baseline. “Disturbed” cortisol rhythm, was defined as the lack of anticipated decline in saliva cortisol in at least one of the 3 following timepoints; i) from 8am to 12-noon, ii) from 12-noon to 6pm, and iii) from 6pm to 10pm.^16^
Statistical analysis was conducted with Stata v.13, SPSS v.27 and GraphPad Prism v. 7.05.
RESULTS
There were 24 patients with RA (83.3% females, mean age: 55 ± 11.3 years), of whom 12/24 had been newly diagnosed at baseline and initiated treatment with DMARDs, while the rest were presented with worsening of disease activity and required escalation of treatment. Current medication consisted of cDMARDs (9/24, 37.5%), b/tsDMARDs monotherapy (3/24, 12.5%), or a combination of DMARDS (12/24, 50%), while 6/24 (25%) were also receiving GC (mean daily dose: 5mg of prednisolone). Table 1 presents a comprehensive overview of the treatment modalities administered to enrolled patients throughout the 2-year follow up period, encompassing all therapeutic agents that were utilised on an individual basis during this time frame.
At 2 years of follow-up, remission, was achieved by 70.8% (17/24) of our study cohort, of whom 58.8% (10/17) were on remission already from 6 months of treatment and remained stable up to 2 years. Notably, of the 17 patients on remission, 13 (54.2%) were on steroid-free remission (defined as successful withdrawal of GC for >1 month prior to visit without disease flair reported or clinically documented by the treating physician). No differences in clinical or laboratory parameters recorded at baseline, including age, disease duration, seropositivity, CRP levels and DAS28 score were observed between those on remission (n=17) and those with moderate or no response to treatment (n=7) (Table 2).
We next investigated the potential predictive value of the baseline evaluation of i) diurnal production of saliva cortisol, ii) plasma ACTH and serum cortisol levels and iii) serum DHEAS levels in the long-term response of our RA patients. Time integrated daily saliva cortisol production at baseline was significantly higher in those patients on remission at 2 years compared to the rest of the patients (99± 42 vs. 68 ± 19, respectively, p=0.04). Individual saliva cortisol measurements at all time points during the day were higher in patients on remission at 2 years, albeit not reaching statistical significance. Circulating levels of ACTH, cortisol, and DHEAS did not differ between the two groups.
To further investigate the integrity of HPA axis in our patients we i) calculated the cortisol/ACTH ratio in a subset of patients (n=18), in whom both serum and plasma samples were available at baseline and ii) we evaluated the proportion of patients with disturbed saliva cortisol rhythm in the 2 groups. Patients on remission at 2 years demonstrated a significantly higher cortisol/ACTH ratio (14/18) compared to the patients with moderate or no response to treatment (4/18) (105.1 ± 49.1 vs. 69.7 ± 20.4 respectively, p=0.04), but the numbers were small. No significant difference was observed in the number of patients with disturbed cortisol rhythm at baseline between the 2 groups.
Among all the parameters evaluated we found that time integrated daily saliva cortisol production (AUC) at baseline was significantly associated with attaining remission at 2years, independently of age, or baseline CRP levels (adjusted beta coefficient=3.83, SE=1.715, p=0.02). We next performed a ROC curve analysis to examine the ability of cortisol AUC at baseline to predict response to treatment after 2 years. A cut off AUC value ≥ 81.3 could identify RA patients attaining remission after 2 years of treatment according to EULAR recommendations, with 86% specificity and 65% sensitivity (Youden’s Index= 0.504, p=0.047) (Figure 1).
Receiver operating characteristic curve for baseline predicting disease-remission at 2 years of follow-up in patients with RA. Remission was based on the Boolean 2.0 criteria.25AUC: area under the curve; DAS: Disease Activity Score; RA: rheumatoid arthritis.
Steroid-free remission was reported in 13 out of 17 patients at 24 months (Suppl. Table 1). Among the parameters evaluated at baseline, patients on steroid-free remission at 2 years had higher, albeit not-significantly, time integrated daily production of cortisol in the saliva and serum cortisol/ACTH ratio, but the numbers were small to draw any definite conclusions.
DISCUSSION
In this study, we confirm the presence of a compromised adrenocortical functional reserve, as indicated by the lower baseline diurnal saliva cortisol production, in RA patients with moderate or no response to treatment at 2-years of follow-up despite being on highly effective DMARDs regimens. In the need of easily accessible biomarkers that could identify long term remission in RA, we suggest that a value ≥ 81.3 of time integrated daily saliva cortisol production (AUC) at baseline, can predict remission with 86% specificity and 65% sensitivity after 2 years of treatment initiation/escalation in RA patients. This is in accordance with our previous results where we showed that low morning saliva cortisol levels <13.9nmol/L, could be used to predict inability to achieve minimal disease activity after 6 months of treatment.^17^Moreover, we identified a significantly lower serum cortisol/ACTH ratio at baseline in RA patients with moderate or no response to treatment at 2 years compared to those on remission, mostly due to the lower serum cortisol levels, regardless of the provided treatment according to the international guidelines.^21^ Cortisol, as a stress hormone, is of pivotal value in inflammation restriction and its inadequate secretion when needed may have a negative impact in RA development, clinical outcome or long-term antirheumatic treatment response, as suggested in our pilot study. Clinical effectiveness of low-dose glucocorticoids in the management of RA has been reported from early years^1^ and their contribution in early and efficient control of Joint destruction has been well established.^4,27,28^ More recent multicentre randomised clinical trials have confirmed the beneficial effects of low-dose exogenous glucocorticoids over placebo or tapering in disease activity control in RA patients,^29,30^ despite the introduction into clinical practice of more targeted therapeutic agents. Therefore, glucocorticoids may be considered as a substitutional therapy for an impaired adrenal glands reserve in, at least some, patients with RA.^16,31^
On the other hand, although, significant progress has been made in our understanding of the cellular and molecular aspects of rheumatoid arthritis and regardless the utilisation of advanced machine learning, the lack of validated biomarkers that could predict treatment response remains an unmet need. In this context, several studies have attempted to identify circulating biomarkers in peripheral blood that could lead to a more precise treatment and a favourable clinical outcome, without adding, though, significant contribution in clinical practice.^32–34^ In the quest to identify circulating biomarkers of predictive value in RA, researchers are currently focusing on the molecular heterogeneity of the synovium tissue to target distinct molecular subtypes of the disease and to pave the way for precise medicine. As endogenous cortisol reduces inflammation by primarily acting through the glucocorticoid receptor (GR),^35^ the functional integrity of GR in the synovium tissue is currently under intense investigation.^36^ It has been shown that decreased cortisol production at the tissue level has been associated with higher GR expression in circulating leukocytes.^37^ In line with this evidence, using RNA-sequencing data from early and established RA, we demonstrated an increased expression of the GR in the synovial tissue of RA patients compared to healthy and osteoarthritic tissue.^38^ Higher GR expression could potentially serve as a compensatory mechanism that makes synovial tissue more sensitive to GC action in patients with disproportionally decreased cortisol in systematic circulation and explain the dramatically positive impact of exogenously-administered GC in RA management.^29–31^
Our pilot study has several limitations: i) the small sample size, since some patients were lost to follow-up, ii) patients with both early-stage and established RA were included in the analysis, increasing the heterogeneity of the study population and disease characteristics, iii) no patients with inactive disease at baseline were included as a control group, and iv) due to the non-interventional study design, as in our original cohort, no unified treatment protocol was used throughout the duration of the study, reflecting however, patients in the clinical setting of an Academic Rheumatology Unit. Taken together, our findings suggest that in a subset of RA patients there is a deficit in endogenous cortisol production that could affect disease pathophysiology and progression. Further studies are needed to confirm that low saliva cortisol levels at baseline in RA patients, could serve as potential valuable and easy-to-use bio-marker to predict treatment response and disease remission over long-term in routine clinical practice.
AUTHOR CONTRIBUTION
Conceptualisation: M.P.Y and P.P.S. Data curation: all authors. Data analysis: M.G.F, N.I.V, M.P.Y, P.P.S. Funding acquisition: P.P.S. Investigation: All authors. Methodology: N.I.V, M.P.Y, M.G.F. Writing original draft: M.G.F and M.P.Y. Writing review and editing: all authors.
FUNDING
No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article. Resources were used from ELKE grant 0974 (P.P.S.)
CONFLICT OF INTEREST
All authors declare no conflict of interest relevant to this manuscript.
NOTE
All authors take full responsibility for the integrity and accuracy of all aspects of the work. All authors confirm that the results of this follow up study have not been previously published as an abstract or in its full version anywhere else.
ETHICS APPROVAL
The study was approved by the scientific committee of “Laiko” General Hospital (E. Σ 38/21-01-2021) and was registered in ClinicalTrials.gov (NCT05671627).
PATIENT CONSENT
Obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Copeman WSC Savage O Bishop PMF Dodds EC Gottlieb B Glyn JH A study of cortisone and other steroids in rheumatoid arthritis. Br Med J 1950;2:849–55.14772498 10.1136/bmj.2.4684.849PMC 2038922 · doi ↗ · pubmed ↗
- 2A comparison of prednisolone with aspirin or other analgesics in the treatment of rheumatoid arthritis. A second report by the joint committee of the Medical Research Council and Nuffield Foundation on clinical trials of cortisone, ACTH, and other therapeutic measures in chronic rheumatic diseases. Ann Rheum Dis 1960;19:331–7.14447267 10.1136/ard.19.4.331PMC 1007163 · doi ↗ · pubmed ↗
- 3Kirwan JR. The effect of glucocorticoids on joint destruction in rheumatoid arthritis. The Arthritis and Rheumatism Council Low-Dose Glucocorticoid Study Group. N Engl J Med 1995;333:142–6.7791815 10.1056/NEJM 199507203330302 · doi ↗ · pubmed ↗
- 4Kirwan JR Bijlsma JWJ Boers M Shea BJ. Effects of glucocorticoids on radiological progression in rheumatoid arthritis. Cochrane Database Syst Rev 2007;2007:CD 006356.17253590 10.1002/14651858.CD 006356 PMC 6465045 · doi ↗ · pubmed ↗
- 5LandewéRBM Boers M Verhoeven AC Westhovens Rvan de Laar MA Markusse HM COBRA combination therapy in patients with early rheumatoid arthritis: long-term structural benefits of a brief intervention. Arthritis Rheum 2002;46:347–56.11840436 10.1002/art.10083 · doi ↗ · pubmed ↗
- 6Jacobs JW Gvan Everdingen AA Verstappen SMM Bijlsma JW. Followup radiographic data on patients with rheumatoid arthritis who participated in a two-year trial of prednisone therapy or placebo. Arthritis Rheum 2006;54:1422–8.16645970 10.1002/art.21809 · doi ↗ · pubmed ↗
- 7Smolen JS LandewéRBM Bergstra SA Kerschbaumer A Sepriano A Aletaha D EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis 2023; 82: 3–18.36357155 10.1136/ard-2022-223356 · doi ↗ · pubmed ↗
- 8Cutolo M Foppiani L Minuto F. Hypothalamic-pituitary-adrenal axis impairment in the pathogenesis of rheumatoid arthritis and polymyalgia rheumatica. J Endocrinol Invest 2002; 25: 19–23.12508908 · pubmed ↗