Kawasaki Disease or Cat Scratch Disease? A Diagnostic Dilemma: A Paediatric Case Report and Literature Review
Daiva Gorczyca, Daniel Lewandowski, Jacek Postępski

TL;DR
A child's case highlights the difficulty in distinguishing Kawasaki disease from atypical cat-scratch disease, emphasizing the need for careful diagnosis.
Contribution
The case expands the known spectrum of Bartonella henselae infection and suggests abdominal ultrasonography as a key diagnostic tool.
Findings
A 6-year-old girl's symptoms initially resembling Kawasaki disease were later attributed to atypical cat-scratch disease.
Abdominal ultrasonography revealed a hypoechoic splenic lesion, aiding in the diagnosis of Bartonella henselae infection.
Literature review identified cases where CSD mimicked autoimmune diseases or malignancies.
Abstract
Kawasaki disease (KD) and atypical cat-scratch disease (CSD) can manifest with fever and similar non-specific symptoms. We report the case of an immunocompetent child who presented with signs and symptoms consistent with KD, which overlapped with those of atypical CSD (hepatosplenic form). Subsequently, we conducted a literature review to identify paediatric cases of KD and CSD. We present the case of a 6-year-old girl with fever, abdominal pain, non-purulent bilateral conjunctivitis, maculopapular rash on the trunk, bilateral cervical lymphadenopathy, and oral mucosa erythema, meeting KD diagnostic criteria. Echocardiography revealed coronary artery dilatations. Despite initial intravenous immunoglobulin (IVIG) treatment eighteen hours later the general condition worsened, with the recurrence of fever, diffuse myalgia, severe abdominal pain, and vomiting. A detailed history revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
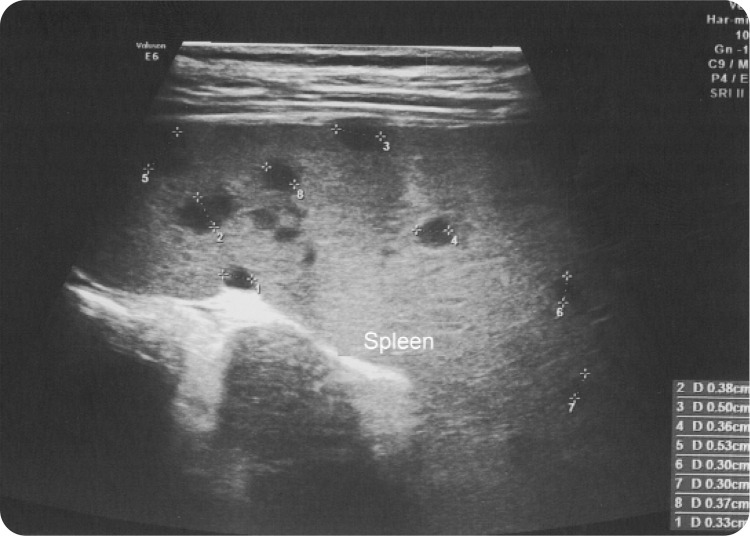 Figure 1
Figure 1|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|
|
| 6/F | 5/F | 5/F | 7/F | 4/M | 8/M |
|
| yes | yes | yes | no, with a hamster | yes | - |
|
| yes | yes | yes | no | yes | - |
|
| 3 weeks | 10 days | several months | - | - | - |
|
| 8 days | 5 days | 11 days | 3 days | 7 days | yes |
|
| yes | yes | - | yes | yes | yes |
|
| erythema of oral mucosa | sore throat, erythema of the lips | - | yes | no | - |
|
| maculopapular rash on the trunk | pale erythema on the anterior surface of the trunk | - | yes | generalised maculopapular rash | yes |
|
| bilateral cervical, left axilla | no | left axilla | cervical | unilateral cervical | - |
|
| - | erythema and oedema of the palms and soles | - | desquamation on the 21st day | - | yes |
|
| left and right CAL | no | left CAL, repeated echo normal | - | no | - |
|
| crampy abdominal pain | - | crampy abdominal pain, nausea | - | - | |
|
| - | - | - | - | bilateral anterior uveitis | - |
|
| diffuse myalgia | myalgia, chest pain | arthralgia | |||
|
| yes | - | - | - | - | - |
|
| 8.2 | 15.9 | 10.9 | - | - | - |
|
| 71 | 75 | 74 | - | 124 | - |
|
| 54 | - | - | - | 120 | - |
|
| 1:160/1:1024 | 1:40 / 1:512 | - | - | IgG 1:100 | IgG 1:100 |
|
| - | - | PCR positive | - | - | - |
|
| multiple granulomatous lesions in the spleen, hepatomegaly | multiple lesions suggesting micro-abscesses in the spleen | first abdominal USG as normal; 2 weeks later numerous small, round, hypoechoic lesions in the liver | - | mild splenomegaly | - |
|
| co-morbidity: complete KD and atypical CSD | atypical CSD mimicking complete KD | atypical CSD mimicking incomplete KD | CSD mimicking complete KD | incomplete KD, CSD mistakenly diagnosed due to false-positive serology following IVIG therapy | incomplete KD, CSD mistakenly diagnosed due to false-positive serology following IVIG therapy |
|
| IVIG 2 g/kg and aspirin | IVIG 2 g/kg and aspirin, but the fever persisted | IVIG two times, because the fever persisted, and aspirin | IVIG two times, aspirin | IVIG 2 g/kg to reduce the risk of KD consequence | IVIG |
|
| amoxicillin, erythromycin 3 months | ceftriaxone-azithromycin 10 mg/kg, as second-line trimethoprimsulfamethoxazole | no data | azithromycin - ampicillin/sulbactam - meropenem - mitomycin | doxycycline 7 days | no data |
|
| Abdominal USG displayed a normal liver two weeks later and a regression of spleen lesions. A 6-month follow-up showed no local or systemic relapse of Bartonella infection, and no coronary artery abnormalities were observed. | The fever resolved on the 8th day of hospitalisation. 10 days after the complete resolution of the granulomatous lesion in the spleen | no data | no data | recovery | recovery |
|
|
|
|
|
|
| |
|---|---|---|---|---|---|---|
|
| 11/F | 11/F | 7/F | 4/F | 9/M | 5/M |
|
| yes | yes | yes | yes | - | yes |
|
| - | yes | no | yes | - | unknown |
|
| - | - | unknown | 1 month | - | 2 months |
|
| - | - | 3 weeks | 3 weeks | Eleven days before fever (39°C) for three days, with a successive spontaneous regression | 4 weeks |
|
| - | yes | yes | - | - | - |
|
| - | - | yes | - | - | - |
|
| - | - | yes | - | - | - |
|
| - | yes | - | - | - | |
|
| - | - | hilar lymph nodes | - | cervical | in the upper right leg |
|
| - | - | - | - | - | yes |
|
| neuroretinitis | - | unilateral conjunctivitis 3 days, unilateral anterior granulomatous uveitis | - | - | - |
|
| - | 8 cm large soft tissue mass on the left temporal bone | arthralgias | myalgia of the legs | - | low back pain without neuro damage |
|
| - | - | erythematous popular rash | no | purpura on limbs and trunk | - |
|
| - | - | 18 | 6.9 | 8.9 | 14.6 |
|
| - | 68 | 80 | 30–90 | normal range | 49 |
|
| - | 95 | 86 | 100–150 | normal range | - |
|
| ||||||
|
| - | - | negative | negative | - | negative |
|
| - | -- | negative | negative | negative | negative |
|
| 1:32 / 1:256 | negative/1:256 | ||||
|
| - | 1:200 / 1:6400 | negative/1:4096 | IgG 1:2048 | ||
|
| - | - | PCR negative | PCR negative | - | blood PCR negative, lymph node PCR positive |
|
| - | several hypodense lesions in the liver and spleen | small hypoechoic lesions in the liver and spleen; subsequent MRI revealed multiple focal lesions in the organs above in keeping with granulomata; echocardiogram normal | low echoic lesions in the liver and spleen on day 38th | - | hepatic and splenic hypoechogenic lesions without hepatosplenomegaly; nine months later no lesions |
|
| Systemic lupus erythematosus positive ANA, hematuria | Langerhans cell histiocytosis a circumscribed lytic skull lesion, histopathology revealed necrosing inflammation without evidence for LCH | Sarcoidosis serum Ca 11.8 mg/dl, ACE 120 mg/dl | Systemic Juvenile Idiopathic Arthritis hypergammaglobulinemia, high complement titres, and an elevated titre of antinuclear antibody 1:80 | Autoimmune thrombocytopenia platelet count 7 × 109/L, coagulation parameters in the reference range | Spondylitis of the D6 vertebra in MRI |
|
| - | Mimicker | Mimicker | B. henselae as trigger of autoimmune disease | As a complication of CSD | Mimicker |
|
| - | Azithromycin 12 weeks | intravenous gentamicin for 7 days, followed by oral ciprofloxacin for 21 days. A combination of topical steroids and tobramycin for a total period of 6 weeks was used to control uveitis | - | Azithromycin 14 days | intravenous rifampicin for 6 weeks and azithromycin for 4 weeks |
|
| Methylprednisolone | none | none | Aspirin 41 days | IVIG 1/kg/die for two days | none |
|
| - | Fever episodes, malaise, and headaches completely resolved within 3 months, first signs of regression of hepatic lesion after 6 months, 12 months later complete | Fever and constitutional symptoms improved within 72 hours of commencing therapy | 11 months later no changes in sonography | end of antibiotic therapy a total regression of cervical lymphadenopathy. After 14 days from hospitalisation, the platelet count was 211x109/L and the patient was asymptomatic | The fever decreased two days after the correct antibiotic treatment, and a love grade fever continued for three weeks. Nine months later no changes in USG. Fatigue for two months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBartonella species infections research · Streptococcal Infections and Treatments · Vector-borne infectious diseases
INTRODUCTION
Kawasaki disease (KD) is a vasculitis of medium-sized vessels, primarily affecting coronary arteries, potentially leading to their dilatation. It typically occurs in children under 5 years old, manifesting acute febrile disease with polymorphic rash, conjunctival injection, oropharyngeal and lip mucositis, tongue papillitis, erythema and edema of the hands and feet, as well as unilateral cervical lymphadenopathy.^1^ In the absence of an available and affordable diagnostic test, a detailed clinical history and physical examination remain crucial for diagnosing KD. It is important to recognise that delayed diagnosis or misdiagnosis of KD can result in an increased risk of cardiac complications, e.g., coronary artery aneurysms, which develop in approximately 25% of untreated cases of KD.^1^
The bacterium Bartonella henselae, an aerobic, intra-cellular, gram-negative bacillus, causes cat-scratch disease (CSD) that commonly affects children and teenagers. In typical CSD, the incubation period ranges from 3 to 10 days, and a papule appears at the site of inoculation approximately 4 to 6 days after the animal scratch.^2^ The regional lymphadenopathy usually develops 1 - 3 weeks after the initial skin findings. This is often associated with constitutional symptoms such as fever, malaise, and night sweats. The disease usually resolves spontaneously within a few weeks.
An extra-nodal manifestation is collectively known as atypical or systemic CSD. It commonly presents with fever of unknown origin, hepatosplenic disease, neurological, cardiac, Parinaud’s syndrome, or musculoskeletal symptoms.^3^ It remains unclear why some patients suffer from atypical manifestations involving visceral organs.
We report a case of an immunocompetent child who presented signs and symptoms consistent with KD, which overlapped with those of atypical CSD (hepatosplenic form). Subsequently, we searched for pediatric cases of KD and CSD published in the literature.
In our case, signed informed consent was obtained from the parents of the patient. The local ethics committee approved the report protocol.
CASE DESCRIPTION
A 6-year-old Caucasian girl was admitted to the hospital due to a fever (39.2^o^C) lasting 2 days, associated with abdominal pain, non-purulent bilateral conjunctivitis, maculopapular rash on the trunk, bilateral cervical lymphadenopathy, and erythema of the oral mucosa. Initial laboratory tests were within normal ranges, except for elevated C-reactive protein levels (71.4 mg/L; normal range <6 mg/L) and erythrocyte sedimentation rate (54 mm/h; normal range 0–20 mm/h). Serologic testing was negative for Epstein-Barr virus, cytomegalovirus*, Mycoplasma pneumoniae*, and Chlamydia pneumoniae. Cultures of blood samples and urine were negative. Testing for anti-nuclear antibodies (ANA), anti-(double stranded)-DNA antibodies (anti-ds-DNA), extractable nuclear antigen antibodies (ENA), anti-proteinase 3 (anti-PR3), and anti-myeloperoxidase (anti-MPO) antibodies were negative. Despite antibiotic therapy with intravenous amoxicillin, the fever persisted. Due to this reason, an expanded differential diagnosis was performed, including infectious and non-infectious conditions. Echocardiography revealed dilated left and right coronary arteries, of 3 mm and 6 mm, respectively. On the eighth day of fever, KD was diagnosed. On the same day blood test showed an anemia for age (haemoglobin 8.6 g/dl; normal range: 11.9–15.0), moderately raised ALT level (68 IU/ml; normal range 0–48), leukocyturia (21–30 WBC/hpf). The patient received intravenous immunoglobulins (IVIG) at a dose of 2 g/kg together with aspirin at a dose of 80 mg/kg/day divided into four doses. A short-term improvement in the general condition and a transient normalisation of the body temperature were observed. Eighteen hours after IVIG infusion, the general condition of the patient worsened, with the reoccurrence of fever, diffuse myalgia, severe abdominal pain, and vomiting. Abdomen ultrasonography revealed an enlarged liver, hypoechoic areas in the spleen (Figure 1), and enlarged left axial lymph nodes, with the largest node measuring 2.5x1.5 cm. An extended history showed that the patient had been scratched on the left thumb by a cat three weeks before admission. Upon examination, an erythematous nodule (2 mm) on the thumb was noted. Serological analyses by the indirect fluorescent antibody (IFA) method detected the positive presence of both IgM 1:160 (normal range <1:20) and IgG 1:1024 (normal range <1:64) antibodies to B. henselae. Treatment with erythromycin (40 mg/kg/day administered orally in four divided doses) for 3 months was introduced. Two weeks later, abdominal ultrasonography displayed a normal liver and a regression of spleen lesions. A 6-month follow-up showed no evidence of local or systemic relapse of B. henselae infection, and no coronary artery abnormalities were observed.
Spleen ultrasound with multiple hypoechoic areas at diagnosis of CSD.
Discussion of similar published cases
We performed a search using PubMed and Google Scholar. Initially, we focused on identifying cases resembling KD and B. henselae infections using keywords such as “Kawasaki disease”, “Cat Scratch Disease”, “Bartonella henselae”, “spleen”, “liver”, “disseminate”, “systemic”, and “mimicker” with detailed control of references. There were no language restrictions. Additionally, we expanded our literature search to determine whether an atypical (sometimes referred to as extra-nodular, systemic, or disseminated) B. henselae infection could present as a mimic of other autoimmune diseases in pediatric patients. Keywords for this extended search included “Cat Scratch Disease”, “Bartonella henselae”, “spleen”, “liver”, “disseminate”, “systemic”, “child”, and “mimicker”. Demographic data (sex, age), epidemiological data, clinical presentations, laboratory findings, radiologic images, clinical course, and treatments were reported and discussed.
It is important to note that Tsuchida et al. published an abstract in Japanese from a conference (319th Kanagawa Regional Meeting of the Japanese Pediatric Society) rather than a full paper.^4^ Despite the limited accessibility of the abstract in English and full text, we included the available data from this abstract. However, we excluded publications referenced by Ma M et al. in the 11^th^ and 12th positions due to the unavailability of the abstracts and/or full texts.^5^
Our case of typical KD, which overlapped with the hepatosplenic form CSD, and the cases from the literature review, highlight the diagnostic complexities in both KD and CSD because these diseases often present with nonspecific symptoms. Through our literature search, we identified five cases describing the co-occurrence of KD and CSD (Table 1).
In our case, the initial clinical presentation, characterised by the presence of four of the five main clinical symptoms, combined with the detection of the dilatation of coronary arteries, supported the diagnosis of complete KD. The diagnosis of atypical (systemic) CSD was based on the history of a cat scratch three weeks before fever onset, along with the identification of an erythematous nodule on the thumb, prolonged fever, axillary lymphadenopathy, a typical splenic lesion in abdominal ultrasonography, and positive B. henselae IgM, IgG serology. We have identified two similar cases of 5-year-old previously healthy girls initially diagnosed with KD and treated with IVIG along with aspirin.^5,6^ Due to persistent fever after the second dose of IVIG, a repeat abdominal ultrasonogram examination was performed and demonstrated numerous small, round, hypoechoic lesions in the spleen^5^ and in the liver.6 Although we lacked the abdominal ultrasonogram before the KD diagnosis and treatment with IVIG, in these cases, the initial abdominal ultrasonogram was normal. Fusani et al., in a retrospective study from a Children’s Hospital in Italy, showed that the systemic CSD form manifested with the classic red-brown non-tender papule (33.3%), more than 14 days of fever (median 17 days), abdominal pain (22.2%), rash (44.4%), asthenia (66.7%), and weight loss (44.4%).^7^ Notably, in this cohort, in all patients with systemic CSD, an abdominal ultrasound revealed alterations compatible with CSD. In our identified case series (Table 1), fever was the most frequent clinical manifestation, observed in all patients, with or without rash in 5 out of 6 cases, lymphadenopathy in 4 out of 6 cases, and crampy abdominal pain and myalgia were each reported in 2 out of 6 cases. However, patients with fever, rash, and lymphadenopathy can be misdiagnosed as having KD instead of infectious (Mycoplasma-induced rash and mucositis, Staphylococcal scalded skin syndrome, BCGosis) or non-infectious (systemic onset juvenile idiopathic arthritis, multisystemic inflammatory syndrome in children (MIS-C) associated with SARS-CoV2) diseases.^8^ In 3 out of 6 cases, abdominal ultrasonography was very useful in diagnosing the hepatosplenic form of CSD, as it can identify typical hypoechoic lesions in the spleen and/or liver.^3,9^ Deregibus et al., in a study conducted at a tertiary care hospital in Argentina, found pathological abdominal ultrasonography in 85.7% of CSD cases.^10^
Our patient, as well as patients from our literature review, have an elevated C-reactive protein level (CRP) (≥ 30 mg/L) and erythrocyte sedimentation rate (ESR) (≥ 40 mm/hour). A Scientific Statement for Health Professionals from the American Heart Association included CRP ≥ 30 mg/L and ESR ≥ 40 mm/hour among supportive laboratory tests for diagnosing incomplete KD.^1^ Fusani et al. reported increased CRP (median 23.4 mg/L, IQR=7.3–44.7) and ESR (median 31 mm/hour, IR=26.25–66.5 mm/hour) levels in the systemic CSD group.^7^
Atypical (systemic) CSD can be easily mistaken for other diseases given its dissemination through the bloodstream and diverse manifestations of symptoms. We identified six cases reported in the literature where CSD in children mimicked autoimmune diseases or oncological processes (Table 2). Atypical CSD has been interpreted as a mimicker of systemic lupus erythematosus,^11^ Langerhans cell histiocytosis,^9^ sarcoidosis,^12^ or spondylitis.^13^ In another case, B. henselae has been implicated as a trigger for systemic juvenile idiopathic arthritis,^14^ or autoimmune thrombocytopenia, which was noted as a complication of CSD.^15^
We believe that both our diagnoses, KD and CSD, were correct and we were dealing with a coincidence in timing when the child developed KD and, shortly thereafter, symptoms of atypical (systemic) CSD. To the best of our knowledge, the time for the development of granulomatous lesions in the liver and spleen in the case of hepatosplenic forms of CSD in immunocompetent patients has not been described in the literature. Johnson et al. reported that the IgM titre against B. henselae became positive by day eleven of the illness defined by the onset of fever and negative by day 40.^16^
IVIG in conjunction with aspirin, is the treatment of choice for Kawasaki disease.^1^ The main mechanisms of the beneficial effects of high dose (> 1 g/kg body weight) IVIG in autoimmune disorders include neutralisation of the functional activity of various autoantibodies and/or inhibition of binding of the autoantibodies to their respective autoantigens, inference with activation of complement and the cytokine network, regulation of T and B cell growth, differentiation, as well as effector functions that provide immunodepression.^17^ IVIG therapy could therefore be associated with increased susceptibility to infections and latent infection reactivation, but currently, a lack of literature data fails to confirm this hypothesis. Yakubowski et al. reported two cases of atypical KD with only positive IgG titres for CSD and suggested that the administration of IVIG provides for the misdiagnosis of CSD.^18^ However, the authors have not provided enough epidemiological data and the timing of serology tests was unspecified in both cases. There was also no information regarding fever recurrence after the initial doses of IVIG**.** In our case and others from our literature review,^5,6^ B. henselae serology was performed after the first IVIG infusion in children who did not respond to IVIG administration and were positive for specific IgM and IgG antibodies titres. The systemic literature review by Lopez et al. has reported cases of Bartonella henselae infection in pediatric solid organ recipients treated with mycophenolate mofetil, tacrolimus, and prednisolone.^19^ Clinically, patients have more often presented with typical CSD, and in the case of atypical CSD hepatosplenic granulomatous lesions, they occur in immunocompetent patients. The hepatic peliosis seen in immunosuppressed patients, especially in HIV patients, was not reported. Incidences of CSD with regional lymphadenopathy and extra-nodular CSD in adults with rheumatologic diseases during therapy with biologic disease-modifying antirheumatic drugs (bDMARDs) were reported previously.^20–24^ To the best of our knowledge, there are no reports in the pediatric population.
The therapeutic approach for B. henselae infection is not standardised and for atypical (systemic) Bartonella infections in children includes macrolides (e.g., erythromycin, azithromycin), rifampicin, or doxycycline for children older than 8 years of age.^25,26^ The optimum duration of antibiotic therapy has not been determined. Our patient tolerated 3 months of therapy with erythromycin well, and a complete recovery was made.
In conclusion, the presented case of a child with KD overlapping with the hepatosplenic form of CSD illustrated the expanding spectrum of B. henselae infection and emphasised the importance of considering this disease in the differential diagnosis of KD and prolonged fever syndromes. We propose the incorporation of abdominal ultrasonography into the initial diagnostic workup considering it to be essential before empiric therapy initiation.
DECLARATION OF INTERESTS
The authors declared no funding and conflicts of interest.
AUTHOR CONTRIBUTIONS STATEMENT
DG conceived of and designed the study. DL prepared the case report. JP was involved in planning and supervising the manuscript. All authors contributed to the interpretation of results, participated in writing the manuscript, critically reviewed the manuscript, and approved the final version for submission.
DISCLAIMER
I, the Corresponding Author, declare that his manuscript is original and has not been copied, submitted, or published elsewhere.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Crindle BW Rowley AH Newburger JW Burns JC Bolger AF Gewitz M American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young Council on Cardiovascular and Stroke Nursing Council on Cardiovascular Surgery and Anesthesia Council on Epidemiology and Prevention. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017;135: · doi ↗ · pubmed ↗
- 2Florin TA Zaoutis TE Zaoutis LB. Beyond cat scratch disease: widening spectrum of Bartonella henselae infection. Pediatrics 2008;121:e 1413–25.18443019 10.1542/peds.2007-1897 · doi ↗ · pubmed ↗
- 3Tirotta D Mazzeo V Nizzoli M. Hepatosplenic Cat Scratch Disease: Description of Two Cases Undergoing Contrast-Enhanced Ultrasound for Diagnosis and Follow-Up and Systematic Literature Review. SN Compr Clin Med 2021;3:2154–2166.34151189 10.1007/s 42399-021-00940-1PMC 8203397 · doi ↗ · pubmed ↗
- 4Tsuchida T Uchimura T Honi H [A case of Bartonella henselae infection with six diagnostic criteria for Kawasaki disease]. J Kanagawa Med Ass 2013;40:144.
- 5Ma M Aoki Y Kitazawa K. Atypical Cat Scratch Disease With Splenic Lesion Mimicking Kawasaki Disease in a Healthy 5-Year-old Girl. Pediatr Infect Dis J 2024;43:e 16–e 19.37922474 10.1097/INF.0000000000004148 · doi ↗ · pubmed ↗
- 6Dangman BC Albanese BA Kacica MA Lepow ML Wallach MT. Cat scratch disease in two children presenting with fever of unknown origin: imaging features and association with a new causative agent, Rochalimaea henselae. Pediatrics 1995;95:767–71.7536916 · pubmed ↗
- 7Fusani L Venturini E Chiappini E Galli L. Cat scratch disease in childhood: a 10-year experience of an Italian tertiary care children’s hospital. World J Pediatr 2023;19:189–93.36100799 10.1007/s 12519-022-00616-3 · doi ↗ · pubmed ↗
- 8Saez-de-Ocariz MGámez-González LB Rivas-Larrauri F Castaño-Jaramillo LM Toledo-Salinas C Garrido-García LM Kawasaki disease mimickers. Pediatr Int 2021;63:880–8.33249696 10.1111/ped.14561 · doi ↗ · pubmed ↗