Comparative features and outcomes of cardiogenic shock in patients with and without prior resuscitated shockable cardiac arrest: Insight from the FRENSHOCK multicenter prospective registry
Hamid Merdji, Vincent Bataille, Anais Curtiaud, Laurent Bonello, François Roubille, Bruno Levy, Pascal Lim, Jean-Claude Dib, Julien Maizel, Nicolas Brechot, Marion Beuzelin, Emmanuelle Fillippi, Miloud Cherbi, Julien Demiselle, Grégoire Rangé, Jérémie Joffre, Marwan Yassine

TL;DR
This study compares outcomes of cardiogenic shock patients with and without prior resuscitated cardiac arrest, finding no worse prognosis in those with prior shockable rhythms.
Contribution
The study provides new insights into the prognosis of cardiogenic shock following resuscitated shockable cardiac arrest.
Findings
Approximately 10% of cardiogenic shock patients had prior resuscitated shockable cardiac arrest.
Shockable CA patients required more respiratory and mechanical support and had more coronary angiography.
Survival rates at 30 days and one year were similar between groups, with better long-term survival in shockable CA survivors.
Abstract
Differences between cardiogenic shock (CS) with and without prior resuscitated cardiac arrest (CA) remain largely unexplored. We hypothesized that patients who experience shockable CA followed by CS are likely to have worse outcomes compared to CS without prior CA. FRENSHOCK is a prospective multicenter observational registry conducted in French critical care units in 2016, which included CS from various etiologies. Patients admitted after resuscitation of a CA were included if they fulfilled previously defined CS criteria. Non-shockable rhythms at the time of medical intervention were considered exclusion criteria and were not recorded in the registry. Among the 771 enrolled patients (mean age 65.7 ± 14.9 years; 71.5 % male), 79 (10.2 %) had a resuscitated shockable cardiac arrest just before inclusion. Shockable CA patients had more respiratory support (78.5 % vs. 33.2 %, p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1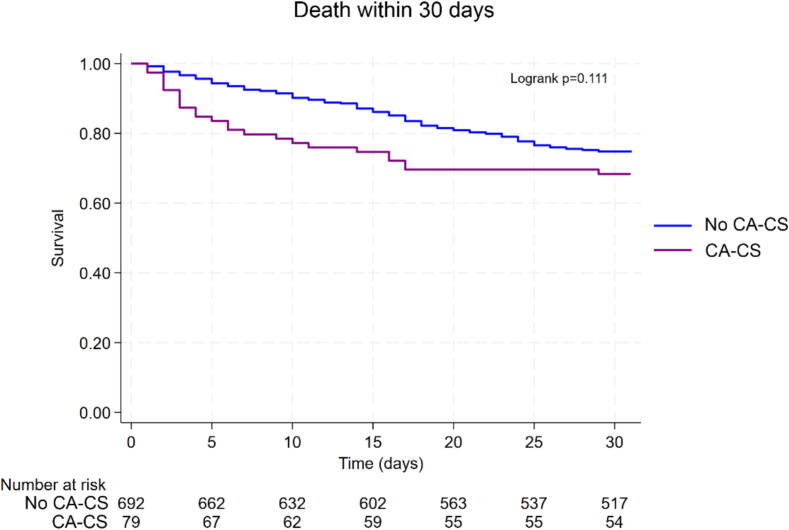 Figure 2
Figure 2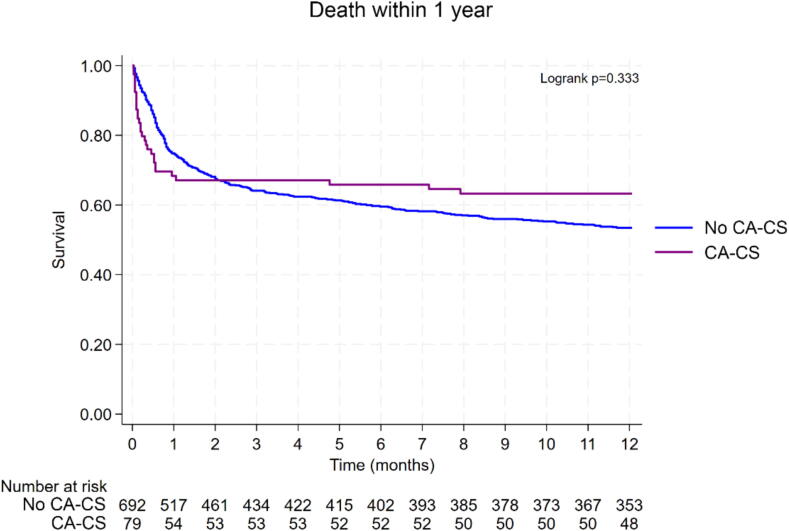 Figure 3
Figure 3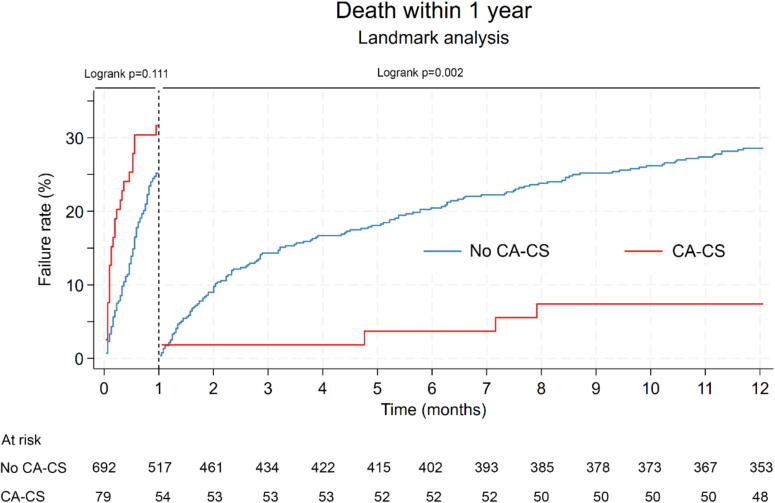 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Mechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair
Introduction
Cardiogenic shock (CS) is one of the most lethal complications of acute cardiovascular disease, with in-hospital mortality rates exceeding 30 % to 40 %.1 Similarly, cardiac arrest (CA) has a very high fatality rate, with nearly 90 % of out-of-hospital cardiac arrest (OHCA) patients in the U.S. not surviving, despite receiving assistance.2 Among those admitted to the hospital after OHCA, mortality remains high, at approximately 40 % to 50 %.3 Thus, both CS and CA are a significant burden on healthcare systems despite advances in supportive care.4
CS can result from a variety of etiologies, with resuscitated CA frequently occurring as one of its precipitating events, regardless of whether the CA is directly triggered by an initial myocardial issue. Consequently, many studies and clinical trials on CS encompass patients who develop CS following resuscitated CA, such as the IMPRESS in Severe Shock trial (which included 92 % patients with prior CA),5 the CULPRIT-SHOCK trial (>50 % of patients with prior CA),6 the HYPO-ECMO trial (almost 50 % patients with prior CA),7 the ECLS-SHOCK trial (>77 % patients with prior CA),8 and the DanGer Shock trial (almost 20 % of patients with prior CA).9 However, while CS in patients with and without preceding CA may share underlying myocardial substrates, their pathophysiological mechanisms and clinical outcomes often differ significantly. Indeed, patients with CS following resuscitated CA (CA-CS) frequently develop a complex post-resuscitation shock syndrome characterized by overlapping cardiogenic and distributive shock components, primarily attributed to ischemia–reperfusion injury and systemic inflammatory response syndrome (SIRS).10 This post-resuscitation shock introduces a complex clinical picture that differs markedly from that of non-CA-CS patients, who primarily experience shock due to pump failure. Additionally, CA-CS patients are more prone to develop anoxic brain injury, a severe neurological complication, which further distinguishes them from those with non-CA-CS.11
Exploring these differences is crucial for tailoring therapeutic strategies to the specific needs of each patient subgroup for redefining critical illness12. As such, distinguishing between CA-CS and non-CA-CS is essential for the design of future studies and for optimizing clinical management in this high-risk population.13, 14, 15 We hypothesized that patients who experience shockable CA followed by CS are likely to have worse outcomes than CS without prior CA. Therefore, our study aimed to assess the features and outcomes of CS in patients based on whether CA precedes the onset of CS. Using data from a dedicated CS registry, we aimed to compare the clinical characteristics, pathophysiological mechanisms, and outcomes between patients with CS following CA with a shockable rhythm (shockable CA-CS group) and those who develop CS without prior CA (non-CA-CS group). By clarifying these differences, we aim to provide essential insights that will enhance the understanding of these characteristics and contribute valuable data to more accurately assess the relevance of including CA-CS patients in future CS studies. The initial primary objective of the FRENSHOCK registry was to evaluate the characteristics, management, and outcomes of CS patients, with a new modified definition of CS as seen in routine clinical practice, on a nationwide scale.
Methods
Patient population
FRENSHOCK is a prospective multicenter observational registry conducted in metropolitan France during six months between April and October 2016 in intensive care unit (ICU) and cardiac intensive care unit (CICU) (NCT02703038). The methods used for this registry have been previously described.16 All adult patients (≥18 years old) with CS were prospectively included in this registry if they met at least one criterion of each of the following three components: (i) hemodynamic criteria, defined as low systolic blood pressure (SBP) < 90 mmHg and/or the need for maintenance with vasopressors/inotropes and/or a low cardiac index < 2.2 L/min/m^2^; (ii) left and/or right heart overload, defined by clinical signs, radiology, blood tests, echocardiography, or invasive hemodynamics’ signs; and (iii) signs of organ malperfusion (clinical and/or biological criteria). Patients could be included regardless of CS etiology, and whether CS was primary or secondary. Exclusion criteria were refusal or the inability to consent, and when a diagnosis of CS was refuted in favor of main alternative diagnoses, such as septic shock and post-cardiotomy CS.
Patients admitted after resuscitation of a CA were included only if they had a shockable rhythm and fulfilled previously defined CS criteria. Non-shockable rhythms at the time of medical intervention and refractory CA under extracorporeal cardiopulmonary resuscitation were considered as exclusion criteria and, therefore, were not included in the registry.
All institutions were invited to participate in the study, including university teaching hospitals, general and regional hospitals, and public and private hospitals that manage CS patients (CICUs, surgical ICUs, medical ICUs, and general ICUs). This inclusive approach was designed to capture a strong representation of adult cardiogenic shock admissions across France during the study period.
Ethics
The study was conducted in accordance with the guidelines for good clinical practice and French law. Written consent was obtained for all the patients. The data recorded and their handling and storage were reviewed and approved by the CCTIRS (French Health Research Data Processing Advisory Committee) (no. 15.897) and the CNIL (French Data Protection Agency) (no. DR-2016-109).
Data collection
The protocol for data collection has been published previously.16, 17 Briefly, the data collected included the patient’s medical history, past treatments, and management of CS during hospitalization, including fluid administration and the use of antibiotics, inotropes/vasopressors, mechanical ventilation, renal replacement therapy, and temporary mechanical circulatory support (tMCS). Additionally, various clinical, biological, and echocardiographic variables were recorded at admission and after 24 h. This protocol has been written according to the “Strengthening The Reporting of OBservational Studies in Epidemiology” (STROBE) guidelines.
Follow-up and censoring
All patients included in the registry were followed for survival status up to one year after inclusion. In cases where vital status was not available at one year, patients were censored at the date of last known follow-up. Loss to follow-up was handled using appropriate time-to-event methods (Kaplan-Meier survival analyses and Cox proportional hazards models).
Statistical analysis
Continuous variables were reported as means (SD) or medians and interquartile ranges when appropriate. Discrete variables were described in numbers and percentages. Groups (shockable CA-CS vs non-CA-CS) were compared using student’s t-tests (or non-parametric Mann & Whitney tests when skewed) for continuous variables; and χ^2^ or Fisher’s exact tests for qualitative variables. Survival in the two groups was computed using the Kaplan-Meier method, and the crude (unadjusted) difference in survival between the two groups was tested using the Logrank test. However, since the survival curves of patients with and without prior CA crossed between one and two months of follow-up, a landmark analysis was performed with a landmark set at 30 days. This approach allows for the comparison of long-term mortality (up to one year) among patients who survived beyond the initial 30 days. Additionally, a stratified analysis based on the variable shockable CA-CS vs. non-CA-CS was conducted to identify factors potentially associated with 30-day mortality in each group. This analysis was performed using a Cox proportional hazards regression model with a stepwise backward selection procedure. The initial model included all factors previously identified as associated with 30-day mortality in univariable analysis (with p < 0.15), adjusted for age. Only variables with p < 0.05 were retained in the final model. Although not strictly “crude” estimates, age-adjusted hazard ratios were derived from univariable Cox regression models adjusted solely for age, given its clinical relevance as a potential confounder. Only variables with p < 0.05 were retained in the final model. The assumption of the Cox model was assessed using Schoenfeld residuals and log(−log) survival plots, and first-order interaction terms were tested. For the CA-CS group, the initial model included the following variables: age, ongoing smoking, furosemide treatment, “other” trigger, sinus rhythm, estimated glomerular filtration rate (eGFR), left ventricular ejection fraction (LVEF), severe aortic stenosis, bilirubin, and BNP/Nt-proBNP. And for the non-CA-CS group, the initial variables were: age, diabetes, chronic kidney disease, ongoing treatment with either vitamin K antagonists or direct oral anticoagulants, infectious trigger, “other” trigger, admission unit, heart rate, systolic blood pressure, mottling, lactate levels, aspartate aminotransferase (AST), BNP/Nt-proBNP, C-reactive protein (CRP), and LVEF.
Statistical analyses were performed using Stata (StataCorp, 2023. Stata 18. Statistical software. StataCorp LLC. Two-sided P values <0.05 were considered significant for all tests.
Results
Study population
A total of 771 patients with CS were included across 49 centers, of whom 79 (10.2 %) had a CA just before admission. Clinical characteristics of patients with and without prior resuscitated CA before the onset of CS are summarized in Table 1. The mean age of the shockable CA-CS group was 60.8 ± 16.8 years, with a predominance of men (84.8 %). These characteristics differed significantly from the non-CA-CS group, where patients were older (66.3 ± 14.6) and less frequently represented by men (69.9 %). Shockable CA-CS patients were more frequently current smokers (48.6 % vs. 25.6 %, p < 0.001) and had a lower prevalence of pre-existing cardiac disease (38 % vs. 58.2 %, p = 0.004), likely contributing to fewer implanted defibrillators (2.5 % vs. 18.1 %, p = 0.003) and less use of cardiotropic medications, including aspirin, furosemide, aldosterone antagonists and vitamin K antagonists. This difference remained statistically significant after adjusting for age.Table 1. Baseline characteristics of cardiogenic shock patients included.Overall (n = 771)Non-CA-CS (n = 692)CA-CS (n = 79)Age-adj. pMale gender55171.548469.96784.80.010Age (years), mean ± SD65.7±14.966.3±14.660.8±16.8−BMI (kg/m^2^), mean ± SD25.8±5.525.8±5.726.6±4.40.283n744668**76Risk factors, n (%)Current smoker20627.917125.63548.60.001Diabetes mellitus21728.220129.11620.30.264Arterial hypertension36447.232747.33746.80.156Dyslipidaemia27735.925336.62430.40.697Medical history, n (%)History of cardiac disease43356.240358.23038.00.004Ischaemic23029.821130.51924.10.664Hypertrophic111.4111.600.0−Idiopathic7810.17310.656.30.210Toxic344.4344.900.0−Multisite pacing638.2618.822.50.112Defibrillator12716.512518.122.50.003CABG628.1578.356.30.841PCI16621.615021.71620.30.695Peripheral artery disease9111.88512.367.60.364Ischemic stroke617.9547.878.90.553Chronic renal failure16421.315522.4911.40.098Dialysis111.4101.511.30.842COPD506.5487.022.50.219Cancer516.6487.033.80.364Previous medications before admission, n (%)Aspirin28837.425036.13848.70.006P2Y12 inhibitor12616.411316.31316.70.733Statins28637.126037.62633.30.966Betablockers31641.029142.12532.10.184Vitamin K antagonist16521.415923.067.70.008Direct oral anticoagulant567.3558.011.30.067ACE inhibitors or ARB29237.926838.72430.80.366Sacubitril/valsartan182.5182.800.0−Furosemide37648.835851.71823.1<0.001Aldosterone antagonist10814.010715.511.30.007Amiodarone13217.612418.4810.40.100Proton pump inhibitor27636.425938.01722.10.019TriggersIschaemic29037.624535.44557.0<0.001Mechanical233.0223.211.30.424Ventricular arrhythmia9812.76910.02936.7<0.001Atrial arrhythmia10814.010014.5810.10.285Conductive disorders182.3142.045.10.074Infectious9612.59413.622.50.013Non compliance303.9294.211.30.229Iatrogenic607.8598.511.30.043Other10213.29513.778.90.090None/undefined11114.410615.356.30.054ACE: Angiotensin-Converting Enzyme. ARB: Angiotensin-Receptor Blocker. BMI: Body Mass Index. CABG: Coronary Artery Bypass Graft. COPD: Chronic Obstructive Pulmonary Disease. PCI: Percutaneous Coronary Intervention. SD: Standard Deviation.
Regarding the triggers of CS (not mutually exclusive), ischemia (57 % vs. 35.4 %, p < 0.001) and ventricular arrhythmia (36.7 % vs. 10 %, p < 0.001) were significantly more common as etiologies in shockable CA-CS patients. Conversely, infection or iatrogenic factors were less frequent triggers of CS among CA-CS patients.
Shockable CA-CS patients exhibited significantly higher levels of hepatic cytolysis, with a median ASAT of 189 IU/L [IQR: 87–541] versus 83 IU/L [37–276] in non-CA patients (p = 0.003), and a median ALAT of 117 IU/L [53–296] versus 56 IU/L [25–170], respectively (p = 0.007) (Table 2). Additionally, hyperlactatemia was more pronounced (median lactate level 4.0 vs. 3.0 mmol/L for shockable CA-CS and non-CA-CS respectively, p < 0.001). C-reactive protein levels at admission were significantly lower in shockable CA-CS patients (median: 6 mg/L [IQR: 2–43]) compared to non-CA patients (29 mg/L [10–70]; p = 0.003).Table 2. Clinical, echographic, and biological characteristics of cardiogenic shock patients included.Overall (n = 771)non-CA-CS (n = 692)CA-CS (n = 79)Age-adj. pFirst medical contact, n (%)Emergency department25733.425236.556.3(ref)Mobile emergency unit22929.816824.36177.2<0.001Hospital (already hospitalized)14719.113719.91012.70.019General practitioner688.8679.711.30.846Cardiologist688.8669.622.50.472Admission unit, n (%)<0.001CICU41470.238774.02740.3Reanimation17629.813626.04059.7Clinical presentation at admissionHeart rate (bpm), mean ± SD95.6±29.696.1±29.091.4±34.20.071n769691**78SBP (mmHg), mean ± SD101±25101±25103±300.728n770691**79DBP (mmHg), mean ± SD63±1763±1761±190.143n769691**78Sinus rhythm, n (%)39952.036152.43848.10.238Mottling, n (%)25638.822137.73548.00.077Blood tests at admissionSodium (mmol/l), mean ± SD135±6134±6138±5<0.001n760683**77eGFR (mL/min/1.73 m^2^), mean ± SD49.6±26.648.8±26.555.9±27.40.295n751674**77Bilirubin (mg/L), median (IQR)16 (9–29)17 (10–31)12 (8–18)<0.001^^*n54448658Haemoglobin (g/dL), mean ± SD12.5±2.312.5±2.312.6±2.40.861n75467876*Arterial blood lactates (mmol/l), median (IQR)3.0 (2.0–4.7)3.0 (2.0–4.0)4.0 (2.0–7.0)<0.001^^n684608**76ASAT (IU/L), median (IQR)90 (39–301)83 (37–276)189 (87–541)0.003^^*n54749354ALAT (IU/L), median (IQR)59 (27–183)56 (25–170)117 (53–296)0.007^^*n55950455Nt proBNP (pg/mL), median (IQR)9277 (4052–23256)9604 (4411–22149)1309 (724–31347)0.025^^*n22421113BNP (pg/mL), median (IQR)1150 (477–2768)1352 (602–2844)210 (75–422)<0.001n26423925CRP (mg/L), median (IQR)28 (9–69)29 (10–70)6 (2–43)0.003^^*n40638125Baseline echographyLVEF (%), mean ± SD26.3±13.426.1±13.127.6±15.20.141n76368578TAPSE (mm), mean ± SD13.4±5.013.2±4.816.0±6.20.015n25923920PSVtdi (cm/s), median (IQR)8 (6–11)8 (6–10)11 (9–17)0.001^^*n20619016Severe mitral regurgitation, n (%)10714.610415.834.00.010Severe aortic stenosis, n (%)364.7345.022.60.630Severe aortic regurgitation, n (%)101.381.222.60.357ALAT: ALanine AminoTransferase. ASAT: ASpartate AminoTransferase. CICU: Cardiologic Intensive Care Unit. CRP: C-Reactive Protein. DBP: Diastolic Blood Pressure. IQR: InterQuartile Range. LVEF: Left Ventricular Ejection Fraction. PSVtdi: Peak Systolic Velocity Tissue Doppler Imaging. SBP: Systolic Blood Pressure. SD: Standard Deviation. TAPSE: Tricuspid Annular Plane Systolic Excursion.
Baseline echocardiographic characteristics
No difference at admission was noticed regarding left ventricular ejection fraction (LVEF) between the two groups. Shockable CA-CS patients also showed a tendency toward less valvular dysfunction, with severe mitral regurgitation present in 4.0 % versus 15.8 % in non-CA patients (p = 0.010) (Table 2). The assessment of right ventricular dysfunction through tricuspid annular plane systolic excursion (TAPSE) and tricuspid peak systolic velocity using tissue Doppler imaging was hindered by the substantial amount of missing data in the shockable CA-CS group.
CS management
Shockable CA-CS patients were more frequently hospitalized from a mobile emergency unit than non-CA-CS patients (77.2 % vs. 24.3 %, p < 0.001), consequently, they were also less frequently hospitalized first in the emergency department (6.3 % vs. 36.5 %, p < 0.001) or elsewhere in the hospital (12.7 % vs. 19.9 %, p < 0.019). As expected, shockable CA-CS patients were more frequently admitted in ICU than in CICU (59.7 % vs. 40.3 %, p < 0.001).
In-hospital management
In hospital management is reported in Table 3. Medical management was different between the two groups, regarding volume expansion, administration of norepinephrine and epinephrine, which was significantly higher in shockable CA-CS patients versus non-CA-CS groups (respectively, 67.5 vs. 39 %; p < 0.001, 69.2 % vs. 51.6 %; p = 0.003, 37.2 % vs. 9.6 %; p < 0.001). Conversely, diuretics were more frequently used in non-CA-CS patients (85.5 vs. 55.1 %, p < 0.001), whereas no difference regarding renal replacement therapy was found between the two groups. The administration of dobutamine did not differ significantly between the non-CA-CS group (83 %) and the shockable CA-CS group (75.6 %, p = 0.10).Table 3. In-hospital management/discharge.Overall(n = 771)non-CA-CS(n = 692)CA-CS(n = 79)Age-adj. pMedications used, n (%)Diuretics63382.459085.54355.1<0.001Volume expander32141.926939.05267.5<0.001Dobutamine63282.357383.05975.60.083 If yes, Maximum dose (μg/kg/min): 5–1040563.837264.73355.00.348 10–1513621.412121.01525.0(ref) >15477.4427.358.30.905 Unknown477.4407.0711.70.478Norepinephrine41053.435651.65469.20.006 If yes, Maximum dose (mg/h) <18621.07420.81222.20.737 1–521552.418953.12648.1(ref) >57518.36117.11425.90.151 Unknown348.3329.023.70.305Epinephrine9512.4669.62937.2<0.001 If yes, Maximum dose (mg/h) <13435.82334.81137.9(ref) 1–54042.12537.91551.70.690 >51414.71116.7310.30.427 Unknown77.4710.600.0–Norepinephrine + dobutamine combination35245.830944.84355.10.125Levosimendan577.4547.833.90.156Dopamine20.320.300.0–Isoprenaline324.2263.867.70.102Antiarrhythmic29838.827139.32734.60.455Transfusion12816.711116.11722.10.280Fibrinolysis131.7131.900.0–Organ replacement therapies, n (%)Respiratory support Invasive29137.922933.262^2^x<0.001 Non invasive19925.917725.72228.20.555Mechanical circulatory support14218.511416.52835.40.002 If yes: IABP4834.54035.7829.60.785 Impella2618.72421.427.40.101 ECLS8460.46356.32177.80.061Renal replacement therapy12115.710615.31519.00.564Invasive cardiology, n (%)CAG39851.633848.86076.0<0.001 If yes: CAG result Normal7418.66719.8711.9(ref) 1 – Mono8020.25716.92339.0<0.001 2 – Bi9022.78224.3813.60.246 3 – Tri8721.98124.0610.20.734 Unknown6616.65115.11525.40.003 Culprit lesion25680.521179.34586.50.331Any PCI21728.217525.34253.2<0.001Any PCI (even in a second time)22629.318426.64253.2<0.001Right heart catheterisation12115.811416.579.00.032Pace-maker implantation354.8314.745.20.657Defibrillator implantation375.1304.679.10.247Radiofrequency ablation172.3162.411.30.575DischargeLVEF (%), mean ± SD35.0±14.534.1±14.442.5±12.60.002n439396**43LVEF variation*, mean ± SD+8.5±14.2+7.9±13.9+13.3±16.00.130n436393**43Length of stay in CICU (days), median (IQR)11(7-21)12(7-21)10(5-16)0.044n44039545Length of stay in hospital (days), median (IQR)17(11-28)17(11-28)17(11-27)0.417n43639343Discharge mode Home17126.415326.41826.1(ref) Rehabilitation446.8366.2811.60.096 Transferred (other center/other department)21433.019633.91826.10.519 Death21633.319133.02536.20.473 Other30.530.500.0–Registration on transplant waiting list406.4376.734.50.187*At discharge compared with admission.**Using log-transformed variable.
Another major difference was the use of respiratory support, which was much more frequent in shockable CA-CS patients (78.5 % vs. 33.2 %, p < 0.001). Mechanical circulatory support was also much more frequent in shockable CA-CS patients (35.4 % vs. 16.5 %, p < 0.001). There was more coronary angiography performed in shockable CA-CS patients (76 % vs. 48.8 %, p < 0.001), highlighting more mono-troncular lesions (39 % vs. 16.9 %, p < 0.001) and leading to more percutaneous coronary intervention than in non-CA-CS patients (53.2 % vs. 25.3 %, p < 0.001).
There was no difference between groups regarding the median length of stay in ICU and/or CICU or discharge mode after hospitalization. At discharge, left ventricular ejection fraction was higher in shockable CA-CS patients compared to non-CA-CS patients (42.5 % vs. 34.1 %, p < 0.001).
Thirty-day and one-year outcomes and correlates
The mortality rate at 30 days was similar in shockable CA-CS patients compared to non-CA-CS patients (31.7 % vs. 25.4 %, Logrank p = 0.11) (Fig. 1). The mortality rate at one year was not statistically different, with 36.7 % mortality in the shockable CA-CS population and 46.1 % in the non-CA-CS population (Logrank p = 0.33) (Fig. 2). However, among 30-day survivors, shockable CA-CS exhibited significantly better long-term survival than the non-CA-CS population (Logrank p = 0.002) (Fig. 3).Fig. 1. Early (30-day) mortality in patients with and without prior resuscitated shockable CA before the onset of CS. Kaplan-Meier Landmark analysis of failure rate (all-cause death) of 30-day survivors. CA-CS: CS following resuscitated shockable CA. No CA-CS: CS without prior resuscitated CA.Fig. 2. Long-term (1-year) mortality in patients with and without prior resuscitated shockable CA before the onset of CS CA-CS: CS following resuscitated shockable CA. No CA-CS: CS without prior resuscitated CA.Fig. 3. Kaplan-Meier Landmark analysis of failure rate (all-cause death) of 30-day survivors in patients with and without prior resuscitated shockable CA before the onset of CS. Kaplan-Meier Landmark analysis of failure rate (all-cause death) among 30-day survivors. CA-CS: CS following resuscitated shockable CA. No CA-CS: CS without prior resuscitated CA.
Patients in the shockable CA-CS group had significantly higher LVEF at discharge (42.5 % ± 12.6 %) compared to the non-CA-CS group (34.1 % ± 14.4 %, p < 0.001). This followed a significant increase in LVEF of 13.3 % (SD = 16) in the shockable CA-CS population, whereas the non-CA-CS population only experienced a 7.9 % (SD = 13.9) improvement (P = 0.018).
Age-adjusted univariate analysis was performed to identify baseline characteristics associated with 30-day and 1-year mortality in both populations (Table S1). Severe aortic stenosis and a clinical profile of congestion (marked by elevated natriuretic peptide levels and routine furosemide treatment) were identified as significant key factors associated with increased 30-day and 1-year mortality in shockable CA-CS patients.
In shockable CA-CS population, the multivariable analysis identified 4 independent factors at admission associated with higher mortality at 30 days: age (aHR = 1.03 [1.01–1.06]), previous treatment by furosemide (aHR = 4.04 [1.66–9.83]); CS trigger classified as “other” (aHR = 4.1 [1.31–12.79]) and severe aortic stenosis (aHR = 10.28 [2.09–50.48]) (Table 4).Table 4. Stratified multivariate analysis of baseline characteristics associated with 30-day mortality in shockable CA-CS and non-CA-CS populations.Death within 30 days – Multivariate Cox RegressionCA-CS (n = 79)non-CA-CS (n = 692)HR95 % CIpHR95 % CIpAge (years)1.031.01–1.060.0211.031.02–1.04<0.001Chronic renal failure1.501.07–2.100.018Previous treatment: Furosemide4.041.66–9.830.002Trigger: infectious1.991.38–2.86<0.001Trigger: other4.101.31–12.790.015SBP (for 10 mmHg increase)0.910.85–0.970.005Arterial blood lactates (mmol/l)Tertile 11.00(ref)Tertile 21.400.96–2.040.085Tertile 31.811.21–2.700.004Unknown value0.920.52–1.65**0.791LVEF (for 10 % increase)0.850.75–0.960.009Severe aortic stenosis10.282.09–50.480.004
In non-CA-CS population, the multivariable analysis identified 3 independent factors at admission associated with higher mortality at 30 days: age (aHR = 1.03 [1.02–1.04]), chronic renal failure (aHR = 1.5 [1.07–2.1]); CS trigger classified as “infectious” (aHR = 1.99 [1.38–1-2.86]), tertile 2 and 3 of the arterial blood lactate (aHR = 1.4 [0.96–2.4] and 1.81 [1.21–2.70]). Conversely, among the non-CA-CS population, a higher SBP and LVEF at admission were independent factors associated with lower mortality at 30 days (Table 4).
Discussion
The present study, conducted within the FRENSHOCK registry, aimed to elucidate the clinical outcomes of patients who developed CS following a resuscitated CA with a shockable rhythm compared to those with CS arising from other etiologies (non-CA-CS).
While the annual incidence of cardiogenic shock (CS) in the U.S. adult population is approximately 15 per 100,00018, the incidence of out-of-hospital cardiac arrest (OHCA) treated by emergency medical services is significantly higher—ranging from 66 to 82 per 100,000 adults per year19. Notably, fewer than 20 % of these OHCA patients present with an initial shockable rhythm.20 Indeed, our results about a scarcely, but of utmost importance, issue in CS show that shockable CA-CS patients have similar 30-day and one-year outcomes compared to patients with CS secondary to other causes (non-CA-CS). Even though they usually present at admission with different ages, medical history, and triggers of CS, but also clinical, biological, and echocardiographic differences.
Our results are in line with those of other studies, which found no significant differences between CS patients with and without prior resuscitated CA. Indeed, in a retrospective study by Ostenfeld et al., the authors examined the effects of OHCA on outcomes in patients with acute myocardial infarction (AMI) complicated by CS.21 The study revealed that among 248 consecutive patients admitted alive to a tertiary center with the diagnosis of AMI-CS, 48 % presented with OHCA and 52 % without. Although these patients had higher lactate levels upon admission, out-of-hospital CA was not found to be an independent predictor of mortality. Moreover, a large Danish cohort study (n = 1,716) including patients with AMICS admitted to two tertiary heart centers (2010–2017) was conducted, capturing approximately two-thirds of the Danish AMICS population.22 Interestingly, patients with and without prior OHCA initially presented with similar metabolic and hemodynamic profiles. However, during the first days in ICU, marked differences emerged between the groups. Despite unadjusted analysis suggesting no significant difference in 30-day mortality between OHCA and non-OHCA patients, the cause of in-hospital death differed substantially. Hypoxic brain injury, leading to withdrawal of life support, was the primary cause of death in the OHCA group (56 %), compared to only 4 % in the non-OHCA group. Conversely, CS was the leading cause of death in the non-OHCA group (60 %) compared to 27 % in the OHCA group.22 Similarly, in a post hoc study of the HYPO-ECMO trial,7 there was no significant difference between CS patients with or without prior resuscitated CA supported by venoarterial extracorporeal membrane oxygenation.23 In this study, however, it is important to note that patients with cardiopulmonary resuscitation exceeding 45 min and out-of-hospital refractory CA were excluded.
Our observation is notable given the substantial physiological and metabolic derangements associated with CA, which can often lead to prolonged periods of ischemia and reperfusion injury, leading to multiple organ failure and ischemic encephalopathy.24 It is possible that the rigorous management strategies employed in contemporary critical care, including advanced mechanical circulatory support and targeted therapies, have contributed to mitigating the adverse effects of prior CA on outcomes in patients with CS.25
Our study focused exclusively on patients who developed CS following a CA and did not consider the reverse scenario, where a CA occurred secondary to pre-existing ongoing CS during hospitalization. This distinction is crucial, as the underlying pathophysiology and prognostic implications of these two scenarios differ, as it was recently evaluated in a retrospective, single-center study by Ahmed et al., who investigated the incidence, clinical characteristics, and outcomes of in-hospital CA in patients admitted to the CICU for CS. Among 1,498 patients with CS, 34 % experienced CA during their hospitalization in CICU, with ventricular fibrillation as the most common trigger (50.6 %). In this study, patients with in-hospital CA during CS management experienced significantly higher rates of both in-hospital (51 % vs. 24.2 %, p < 0.001) and 1-year mortality (adjusted hazard ratio 1.53, p < 0.001).26
Interestingly, one of the findings of our study was that among survivors beyond 30 days, patients with shockable CA-CS exhibited better long-term survival compared to those with non-CA-CS. This may be explained by differences in baseline characteristics (shockable CA-CS patients were younger with less history of cardiac disease) and by the greater improvement in LVEF observed at discharge in the shockable CA-CS group. These results underscore the importance of avoiding therapeutic nihilism in carefully selected CA-CS patients, as a more aggressive management approach could potentially yield favorable outcomes. To better identify patients at risk of unfavorable outcomes in CA-CS, a recent study by Besch et al. highlighted several key predictors of poorer prognosis, including prolonged cardiopulmonary resuscitation (CPR), unwitnessed CA, and OHCA, all of which are strongly associated with an increased risk of anoxic brain injury.27
However, it is essential to acknowledge the limitations of our study. As in any observational study, there are limitations to our analysis. First, patients were enrolled from ICU and CICU (directly or after transfer from another center), and we cannot exclude the possibility that severe comorbid, older, or most severe cases with multiple organ failure could have not been transferred for futility. Moreover, data for patients who died early (before informed consent was obtained) were not collected and recorded in the database because of administrative regulations. Thus, a potential 'healthy survivor bias' may have contributed to an underestimation of mortality, particularly in the shockable CA-CS group.28 Patients with shockable CA-CS who did not survive long enough for ICU admission or those who died early before informed consent could be obtained were excluded, likely leading to a selection of healthier individuals within this group. This selection bias may help explain the absence of excess mortality, despite the more severe clinical presentation in shockable CA-CS patients. Nonetheless, the younger age of shockable CA-CS patients likely played a significant role in their improved survival between 30 days and 1 year. Additionally, regarding patients with CA who were included, the incompleteness of Utstein criteria29 data limits the generalizability of our findings. Indeed, information on prognostic modifiers main factors, such as the initial location of CA and no-flow or low-flow durations, proportion of witnessed and bystander CPR, and the cause-of-death data, was not available. One limitation of our analysis is the use of backward selection, which may omit true confounders or introduce bias through over-adjustment or collider effects. Another limitation to mention is that SCAI SHOCK Stage Classification was not used for the CS severity classification, given that this score was not yet available at the time of the study, since it was first published in 2019.30 To our knowledge, this is the first study to comprehensively address features and outcomes of CS resulting from diverse etiologies (including ischemic and non-ischemic) in patients with and without prior resuscitated CA.
In accordance with expert recommendations, CA should be more precisely defined within the context of CS studies and trials, to include only cases that do not inherently predispose to more severe outcomes than the general CS population.4
Conclusion
In a cohort of patients with cardiogenic shock from various etiologies, approximately 10 % had experienced prior resuscitation following a cardiac arrest with shockable rhythms. Our findings suggest that while a resuscitated cardiac arrest with a shockable rhythm is a recognized risk factor for the development of cardiogenic shock, selected cardiac arrest with a shockable rhythm leading to cardiogenic shock does not inherently confer a worse prognosis compared to other causes of cardiogenic shock. However, further research is needed to fully elucidate the long-term outcomes in this population and to determine the appropriateness of including patients with cardiogenic shock secondary to cardiac arrest in future clinical trials.
Consent for publication
All authors hereby consent to the publication.
Availability of data and material
All summarized data are available upon request.
CRediT authorship contribution statement
Hamid Merdji: Writing – review & editing, Writing – original draft, Formal analysis, Conceptualization. Vincent Bataille: Writing – review & editing, Data curation. Anais Curtiaud: Writing – review & editing. Laurent Bonello: Writing – review & editing. François Roubille: Writing – review & editing. Bruno Levy: Writing – review & editing. Pascal Lim: Writing – review & editing. Jean-Claude Dib: Writing – review & editing. Julien Maizel: Writing – review & editing. Nicolas Brechot: Writing – review & editing. Marion Beuzelin: Writing – review & editing. Emmanuelle Fillippi: Writing – review & editing. Miloud Cherbi: Writing – review & editing. Julien Demiselle: Writing – review & editing. Grégoire Rangé: Writing – review & editing. Jérémie Joffre: Writing – review & editing. Marwan Yassine: Writing – review & editing. Caroline Biendel: Writing – review & editing. Fanny Bounes: Writing – review & editing. Guillaume Leurent: Writing – review & editing. Edouard Gerbaud: Writing – review & editing. Eric Bonnefoy: Writing – review & editing. Etienne Puymirat: Writing – review & editing. Clément Delmas: Writing – review & editing. Nadia Aissaoui: . François Bagate: . Florence Boissier: . Éric Bonnefoy-Cudraz: . Marie Boughenou: . Stéphane Boule: . Jérémie Bourenne: . Cédric Bruel: . Alain Cariou: . Philippe Castellant: . Sébastien Champion: . Karim Chaoui: . Marion Chatot: . Nicolas Combaret: . Nicolas Debry: . Xavier Delabranche: . Raphael Favory: . Emmanuelle Filippi: . Romain Gallet: . Frédérique Ganster: . Philippe Gaudard: . Brahim Harbaoui: . Patrick Henry: . Benoit Herce: . Fabrice Ivanes: . Philippe Karoubi: . Hadi Khachab: . Khalifé Khalife: . Kada Klouche: . Vincent Labbe: . Marc Laine: . Nicolas Lamblin: . Benoit Lattuca: . Yann Lefetz: . Gilles Lemesle: . Philippe Letocart: . Leurent: . Guillaume Louis: . Jacques Mansourati: . Stéphane Manzo-Silberman: . Séverine Marchand: . Benjamin Marchandot: . Stéphanie Marliere: . Joy Mootien: . Frédéric Mouquet: . Louis Niquet: . Alexis Paternot: . Vincent Probst: . Charlotte Quentin: . Grégoire Range: . Nassim Redjimi: . Jean Christophe Richard: . Christophe Saint Etienne: . Francis Schneider: . Guillaume Schurtz: . Marie-France Seronde: . Julien Ternacle: . Gérald Vanzetto: . Elie Zogheib: .
Ethics approval and consent to participate
The data recorded, their handling, and storage were reviewed and approved by the CCTIRS (French Health Research Data Processing Advisory Committee) (no. 15.897) and the CNIL (French Data Protection Agency) (no. DR-2016-109).
Funding
The study was sponsored by the Fédération Française de Cardiologie and was funded by unrestricted grants from Daiichi-Sankyo and Maquet SAS.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jung C.Bruno R.R.Jumean M.Management of cardiogenic shock: state-of-the-art Intensive Care Med 202410.1007/s 00134-024-07618-x PMC 1154137239254735 · doi ↗ · pubmed ↗
- 2Virani S.S.Alonso A.Benjamin E.J.Heart disease and stroke statistics-2020 update: a report from the American Heart Association Circulation 1412020 e 139e 5963199206110.1161/CIR.0000000000000757 · doi ↗ · pubmed ↗
- 3Yan S.Gan Y.Jiang N.The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis Crit Care 242020613208774110.1186/s 13054-020-2773-2PMC 7036236 · doi ↗ · pubmed ↗
- 4Jentzer J.C.van Diepen S.Henry T.D.Understanding how cardiac arrest complicates the analysis of clinical trials of cardiogenic shock Circ Cardiovasc Qual Outcomes 132020 e 00669210.1161/CIRCOUTCOMES.120.00669232862695 · doi ↗ · pubmed ↗
- 5Ouweneel D.M.Eriksen E.Sjauw K.D.Percutaneous mechanical circulatory support versus intra-aortic balloon pump in cardiogenic shock after acute myocardial infarction J Am Coll Cardiol 6920172782872781034710.1016/j.jacc.2016.10.022 · doi ↗ · pubmed ↗
- 6Thiele H.Akin I.Sandri M.PCI strategies in patients with acute myocardial infarction and cardiogenic shock N Engl J Med 3772017241924322908395310.1056/NEJ Moa 1710261 · doi ↗ · pubmed ↗
- 7Levy B.Girerd N.Amour J.Effect of moderate hypothermia vs normothermia on 30-day mortality in patients with cardiogenic shock receiving venoarterial extracorporeal membrane oxygenation: a randomized clinical trial JAMA 32720224424533510376610.1001/jama.2021.24776 PMC 8808325 · doi ↗ · pubmed ↗
- 8Thiele H.Zeymer U.Akin I.Extracorporeal life support in infarct-related cardiogenic shock N Engl J Med 3892023128612973763414510.1056/NEJ Moa 2307227 · doi ↗ · pubmed ↗