Clinical significance of altered expression of mitochondrial genome-derived LncRNA LIPCAR in colorectal cancer
Seyed Taha Nourbakhsh, Fatemeh Mohamadhashem, Mohammad Mehdi Naghizadeh, Amirnader Emami Razavi, Abdolreza Daraei, Faezeh Mohamadhashem

TL;DR
This study finds that LIPCAR, a mitochondrial lncRNA, is significantly downregulated in colorectal cancer tissues, suggesting it could act as a tumor suppressor and potential diagnostic biomarker.
Contribution
This is the first study to investigate the expression profile of LIPCAR in colorectal cancer and its potential as a diagnostic biomarker.
Findings
LIPCAR expression is significantly downregulated in CRC tumor tissues compared to non-tumor tissues.
LIPCAR shows diagnostic potential with an AUC of 0.75 in distinguishing CRC tissues.
No significant correlation was found between LIPCAR downregulation and clinical parameters.
Abstract
The prevalence and mortality of colorectal cancer (CRC) are rising; therefore, understanding its molecular pathophysiology is necessary for identifying reliable diagnostic and therapeutic markers. Several studies corroborate the fact that the initiation and progression of various diseases, including cancers, are significantly influenced by the dysregulation of mitochondrial transcripts, such as lncRNAs encoded by the mitochondrial genome. This study is the first to examine the expression profile of LIPCAR in CRC and its correlation with clinicopathological parameters. In this work, 40 pairs of CRC tissues were obtained, including 40 tumor samples and 40 adjacent non-tumor samples. The SYBR green technique was applied in real-time PCR to analyze the expression profile of LIPCAR in CRC patients. The findings indicated a significant downregulation of LIPCAR in tumor tissue samples…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
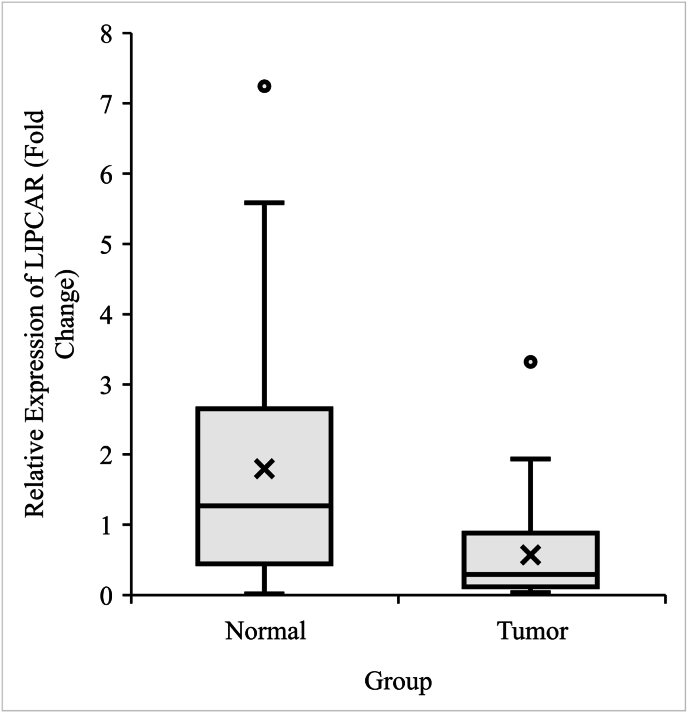 Figure 1
Figure 1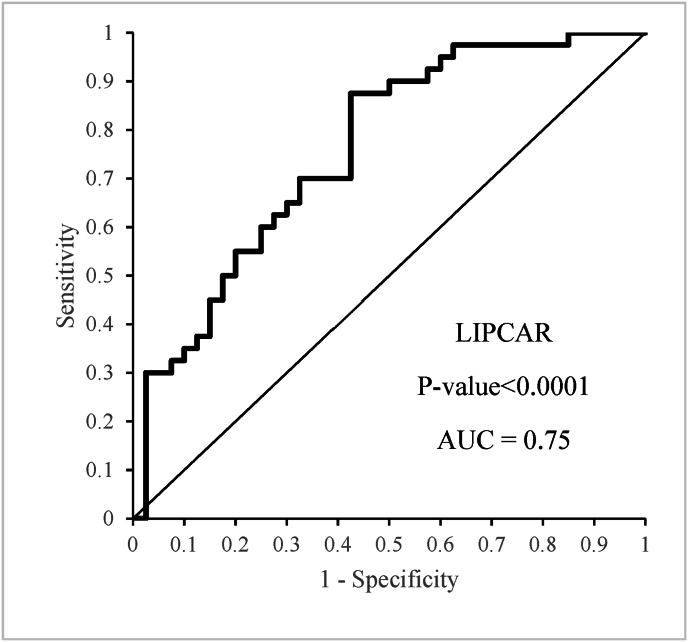 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer-related molecular mechanisms research · RNA modifications and cancer · RNA Research and Splicing
Introduction
1
Colorectal cancer (CRC) ranks as the second-leading cause of cancer-related mortality and the third-most prevalent malignancy worldwide [1]. By 2030, global projections estimate over 2.2 million new CRC cases and 1.1 million deaths [2]. Similar to other solid tumors, CRC is a heterogeneous disease characterized by various subtypes, each defined by unique molecular and/or clinical features. These subtypes fall into three major categories: chromosomal instability (CIN), microsatellite instability (MSI), and CpG island methylation phenotype (CIMP), based on distinct carcinogenetic pathways [3]. Furthermore, CRC can be classified into two primary types: the more common sporadic form, which accounts for approximately 65 % of cases and arises from genetic and epigenetic alterations, and the rarer hereditary forms [4,5]. Despite advances in therapeutic approaches, CRC remains associated with poor prognosis. Consequently, a deeper understanding of the mechanisms driving CRC carcinogenesis and metastasis is essential to identify novel therapeutic targets and biomarkers that enable efficient early detection, personalized treatments, and effective monitoring to improve patient outcomes.
Metabolic reprogramming, a hallmark of cancer, plays a pivotal role in the initiation and progression of various malignancies, including CRC. Cancer cells often rewire their metabolic pathways to sustain rapid proliferation, meeting their substantial energy and biosynthetic demands [6]. One prominent feature of metabolic reprogramming is the Warburg effect, wherein cancer cells preferentially utilize glycolysis over mitochondrial oxidative phosphorylation for energy production, even under oxygen-rich conditions. This metabolic shift is closely tied to mitochondrial dynamics [[7], [8], [9], [10]]. As the metabolic hub of tumor cells, mitochondria fulfill the energy, metabolic, and signaling demands necessary for tumor growth, survival, and metastasis. Thus, mitochondria are integral players in metabolic reprogramming and cancer development [11]. Numerous studies have demonstrated that mitochondrial DNA (mtDNA) mutations and alterations significantly contribute to CRC pathophysiology [[12], [13], [14]].
Recent research has further highlighted the role of mitochondrial transcriptomics in cancer. Beyond mutations in mtDNA, alterations in mitochondrial-encoded non-coding RNAs (mt-ncRNAs) have emerged as significant contributors to the pathogenesis of various diseases, including cancer [[15], [16], [17], [18], [19]]. Notably, a significant subtype of these non-coding RNAs is mitochondrial-encoded long non-coding RNAs (mt-lncRNAs), which, similar to long non-coding RNAs encoded by the nuclear genome, exceed 200 nucleotides in length [20,21].
Long intergenic noncoding RNA predicting cardiac remodeling (LIPCAR), a 781-nucleotide chimeric mt-lncRNA, is one of the most important lncRNAs encoded by the mitochondrial genome. Its 5′ segment corresponds to the antisense strand of the mitochondrial CYTB gene, while its 3′ segment aligns with the antisense strand of the mitochondrial COX2 gene [22]. LIPCAR has been shown to serve as a prognostic biomarker in heart failure and cardiac remodeling [22,23]. Interestingly, elevated LIPCAR expression levels have been reported in hepatocellular carcinoma (HCC), where it promotes tumor growth, migration, and metastasis, suggesting that its biological functions are closely linked to mitochondrial dynamics [24].
To our knowledge, no research has explored LIPCAR expression and its function in CRC. In this study, we aimed to evaluate the clinical relevance of LIPCAR by analyzing its expression profile in CRC tumor tissues versus adjacent non-tumoral tissues and assessing its association with clinicopathological features.
Materials and methods
2
Subjects
2.1
Forty paired tissue samples (tumoral and adjacent non-tumoral tissues) from patients diagnosed with CRC were obtained from Iran National Tumor Bank (Imam Khomeini Hospital, Tehran, Iran). All patients provided written informed consent before participating and the study was approved by the Ethics Committee of Shahrekord University of Medical Sciences (IR.SKUMS.MED.REC.1402.075). Before surgery, none of the patients had received any preoperative therapies, such as chemotherapy or radiation.
RNA extraction and quantification
2.2
Total RNA was extracted from the CRC and adjacent non-tumoral tissues using the RNSol H reagent (ROJE Technologies, Tehran, Iran), according to the manufacturer's protocol. The quality and quantity of the RNA were assessed using both spectrophotometric analysis (NanoDrop 2000c, Thermo Fisher Scientific) and electrophoresis on a 1 % agarose gel. cDNA synthesis was carried out using Easy cDNA Synthesis Kit (Parstous, Mashhad, Iran), following the provided guidelines.
Quantitative real-time PCR
2.3
Gene expression levels were quantified using quantitative real-time PCR (qRT-PCR) with specific primers for LIPCAR and ACTB as the housekeeping gene. The primers were selected based on previously published studies [25,26]. Reactions were carried out in duplicate using Rotor-Gene 6000 (Qiagen, Hilden, Germany) and ExcelTaq 2X Q-PCR Master Mix (SMOBIO). The amplification program included an initial denaturation at 95 °C for 10 min, followed by 40 cycles of 95 °C for 15 s, 59 °C for 30 s (annealing temperature), and 72 °C for 30 s. The relative expression of LIPCAR was calculated using the 2^−ΔΔCt^ method.
Statistical analysis
2.4
IBM SPSS Statistics 27 was used for statistical analysis, and p-values <.05 were considered statistically significant. The relative expression of LIPCAR in tumors and nearby non-tumoral tissues was compared using the Wilcoxon test and the paired sample t-test. The relationship between the LIPCAR fold change and clinicopathological data was investigated using the Mann-Whitney and Kruskal-Wallis tests. Based on the median, the LIPCAR fold change was then divided into two groups: low and high expression. The difference between these groups was examined using the chi-square test. The Receiver Operating Characteristic (ROC) curve and the area under the curve (AUC) were used to assess the diagnostic value, while the Kaplan–Meier method was employed to evaluate overall survival (OS). Graphs were created using Excel software.
Results
3
Clinical characteristics
3.1
This study included 40 CRC patients. The clinical and demographic characteristics of the study population are summarized in Table 1. The study comprised 70 % males and 30 % females, with a mean age of 59.33 years (range: 26–93 years). Most patients presented with tumors classified as T3-T4 (87.5 %), N1–N2 (80 %) with no evidence of metastasis (M0:95 %). Histopathological evaluation revealed that 80 % of cases were categorized as stages III-IV, and lymph node involvement was observed in 65 %. Additionally, lifestyle factors such as smoking were reported in 20 % of patients. No significant differences were observed between the groups in any of these variables.Table 1. Demographic and clinicopathological parameters of CRC participants.Table 1. CountColumn N %Age<602152.5 %>601947.5 %SexF1230.0 %M2870.0 %Site of primaryColon2665.0 %Rectum1435.0 %GradeGrade I1025.0 %Grade II2050.0 %Grade III1025.0 %Lymphatic invasionYes2665.0 %No1435.0 %Vascular invasionYes2870.0 %No1230.0 %Pathological TT1-T2512.5 %T3-T43587.5 %Pathological NN0820.0 %N1–N23280.0 %Clinical MetastasisM03895.0 %M125.0 %StageI-II820.0 %III-IV3280.0 %Smoking StatusNon-smoker3280.0 %Smoker820.0 %Table 2. Association between the clinicopathological and demographic features of CRC patients and LIPCAR expression.Table 2LIPCARP-valueNumberMeanSDMedianAge<6021.48.50.28.49>6019.66.81.32SexF12.60.50.58.55M28.56.73.28Site of primaryColon26.41.41.23.06Rectum14.87.92.57Histology gradeGrade I10.49.42.45.79Grade II20.54.75.25Grade III10.71.72.41Lymphatic invasionYes26.52.70.26.44No14.67.60.65Vascular invasionYes28.51.68.26.4No12.70.62.65Pathological TT1-T25.94.51.95.05T3-T435.52.67.28Pathological NN08.72.62.50.23N1–N232.53.68.26Clinical MetastasisM038.56.68.28.19M12.79.34.79StageI-II8.72.62.50.23III-IV32.53.68.26Smoking StatusNon-smoker32.49.47.26.41Smoker8.901.14.48Table 3Association between the clinicopathological and demographic features of CRC patients and LIPCAR expression, according to dividing fold changes into two groups of high and low expressions.Table 3LIPCARP-valueLowHighCountColumn N %CountColumn N %Age<601260.0 %945.0 %.34>60840.0 %1155.0 %SexF525.0 %735.0 %.49M1575.0 %1365.0 %Site of primaryColon1575.0 %1155.0 %.18Rectum525.0 %945.0 %Histology gradeGrade I420.0 %630.0 %.44Grade II1260.0 %840.0 %Grade III420.0 %630.0 %Lymphatic invasionYes1470.0 %1260.0 %.5No630.0 %840.0 %Vascular invasionYes1575.0 %1365.0 %.49No525.0 %735.0 %Pathological TT1-T215.0 %420.0 %.15T3-T41995.0 %1680.0 %Pathological NN0210.0 %630.0 %.11N1–N21890.0 %1470.0 %Clinical MetastasisM020100.0 %1890.0 %.14M10.0 %210.0 %StageI-II210.0 %630.0 %.11III-IV1890.0 %1470.0 %Smoking StatusNon-smoker1785.0 %1575.0 %.42Smoker315.0 %525.0 %
The expression levels of LIPCAR in tumoral and non-tumoral adjacent tissues
3.2
The statistical analysis of the qRT-PCR data revealed a significant downregulation of LIPCAR in tumor tissues (median = .29) compared to the adjacent non-tumoral tissues (median = 1.26; p-value = .0001; Fig. 1).Fig. 1. Relative expression level of LIPCAR in CRC samples (n = 40) compared to adjacent non-tumoral samples (n = 40). The paired sample t-test was used to compare the level of LIPCAR expression. SCAR/mc-COX2 expression was significantly decreased (p-value = 0001) in tumor tissues compared to adjacent non-tumoral tissues.Fig. 1
Clinical significance and diagnostic value of LIPCAR
3.3
The potential of LIPCAR as a clinical biomarker was assessed through ROC curve analysis. The findings demonstrated that LIPCAR could be utilized for CRC diagnosis and prognosis, showing an AUC of .75 (p-value <.0001; Fig. 2), with a sensitivity of 87.5 % and a specificity of 57.5 % at a cutoff value of .094. The analysis of the relationship between LIPCAR expression levels and clinicopathological parameters revealed no statistically significant associations (Table 2). Furthermore, categorizing patients into low and high expression groups based on LIPCAR fold change did not demonstrate any significant correlations with clinical characteristics (Table 3).Fig. 2ROC curve analysis on the relative expression level of LIPCAR to ascertain its biomarker value to distinguish tumors from non-tumoral samples.Fig. 2
Discussion
4
Metabolic pathways are critical for maintaining cellular stability and homeostasis under normal physiological conditions. However, during the onset and progression of cancer, these pathways undergo significant alterations that become crucial for the survival and proliferation of cancer cells, as well as for the process of carcinogenesis [27]. Consequently, metabolic reprogramming has emerged as a hallmark of many malignancies, including CRC [6,28]. Mitochondria, as one of the most vital intracellular organelles, play diverse roles in cellular processes, including energy production, metabolite synthesis, regulation of cell signaling and apoptosis, and maintenance of metabolic homeostasis [[29], [30], [31]]. Extensive research has identified mitochondrial dysfunction as a fundamental factor in CRC development. Mitochondrial alterations drive carcinogenesis by reshaping metabolic pathways, facilitating tumor initiation and growth, promoting resistance to therapeutic agents, and enhancing metastatic potential [10,32]. Advances in molecular techniques and bioinformatics tools have further underscored the role of mitochondrial transcriptomics in cancer. Beyond the well-documented contributions of mtDNA defects and mutations, disruptions in mitochondrial transcriptomics—including non-coding RNAs, such as mt-lncRNAs—have been increasingly recognized as pivotal players in cancer pathogenesis [17,[33], [34], [35], [36], [37]].
In this study, we investigated the expression level of the important mt-lncRNA LIPCAR in CRC tumor tissues to adjacent non-tumoral tissues. Additionally, we explored its potential relationship with clinicopathological factors. Our results revealed a significant downregulation of LIPCAR expression in tumor tissues. However, no significant correlation was observed between LIPCAR expression and clinicopathological parameters. Furthermore, Receiver Operating Characteristic (ROC) curve analysis demonstrated that LIPCAR exhibited promising biomarker potential, with an Area Under the Curve (AUC) value of .75. Notably, the addition of other clinicopathological characteristics to the expression variable, followed by ROC curve analysis, improves the accuracy of biomarker discovery; however, the sample size in this study precluded this.
Given its reduced expression in CRC, LIPCAR may play a significant role in the development and progression of this malignancy, potentially functioning as a tumor suppressor. Interestingly, in a study by Bongolo et al., LIPCAR was shown to be significantly upregulated in hepatocellular carcinoma (HCC) cell lines and plasma samples [24]. Their findings revealed a significant upregulation of LIPCAR expression in both HCC cell lines and plasma samples. Moreover, this elevated expression was associated with various clinicopathological factors, including gender, glucose levels, alanine aminotransferase (ALT), and aspartate aminotransferase (AST). The heightened expression levels demonstrated considerable diagnostic potential for HCC. Notably, the overexpression of LIPCAR significantly promoted cell proliferation, migration, invasion, and epithelial-mesenchymal transition (EMT) while suppressing apoptosis in vitro. Furthermore, it enhanced tumor proliferation and metastatic potential in vivo [24]. Beyond cancer, LIPCAR has been implicated in other pathological conditions. For instance, Zhang et al. reported that elevated plasma levels of LIPCAR were associated with an increased risk of coronary artery disease (CAD), suggesting its potential as a biomarker for this condition [38]. Additionally, LIPCAR levels were shown to rise during advanced stages of left ventricular remodeling and in patients with chronic heart failure, making it a valuable prognostic marker for cardiac remodeling and a predictor of mortality in heart failure patients [22,23]. According to a recent research report, the expression level of LIPCAR in atrial fibrillation was strongly linked to the phosphorylation of TGF-β1 and Smad2/3, indicating that it controls atrial fibrosis through the TGF-β/Smad pathway [39]. Furthermore, Wang et al. demonstrated that vascular smooth muscle cell migration and proliferation were enhanced by LIPCAR overexpression [40]. Notably, one of the main limitations of the present study is the relatively small sample size and the uneven distribution of samples across key clinical parameters, such as tumor stage and grade. Moreover, this study focused solely on comparing LIPCAR expression levels between tumor tissues and their adjacent normal counterparts. To address these limitations, future research should incorporate larger and more clinically diverse patient cohorts, accompanied by detailed clinicopathological data. Such studies would enable a more comprehensive assessment of potential associations between LIPCAR expression and clinical features, thereby providing deeper insights into the biomarker's role in tumor progression and its prognostic significance.
Conclusion
5
In conclusion, this study is the first to evaluate the expression levels and clinical significance of LIPCAR in CRC. Our findings indicate that the expression of this mt-lncRNA is significantly downregulated in tumor tissues compared to adjacent non-tumoral tissues. Although no significant associations were observed between LIPCAR expression and clinicopathological characteristics, our results suggest that LIPCAR may hold potential as a biomarker for CRC. However, given the limitations of this study, further functional research is necessary to elucidate the biological role and clinical utility of LIPCAR in CRC.
Ethics approval and consent to participate
The experimental procedures were approved by the Ethics Committee of Shahrekord University of Medical Sciences (IR.SKUMS.MED.REC.1402.075). Informed consent was obtained from all patients by the Iran National Tumor Bank.
Consent for publication
Not Applicable.
Availability of data and materials
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author contributions
Faezeh Mohamadhashem Supervision, Project administration, Funding acquisition, Writing - Review & Editing A Daraei Conceptualization, Writing - Review & Editing ST Nourbakhsh Investigation, Writing - Original Draft Fatemeh Mohamadhashem Writing - Review & Editing M Naghizadeh Formal analysis AN Emami Razavi Resources.
Fundings
The authors would like to acknowledge the 10.13039/501100005756Shahrekord University of Medical Sciences (SKUMS-6982) for their financial support. The funders had no role in the study design, data collection, analysis, publication decision, or manuscript writing process. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H.Ferlay J.Siegel R.L.Laversanne M.Soerjomataram I.Jemal A.Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.71320212092493353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Arnold M.Sierra M.S.Laversanne M.Soerjomataram I.Jemal A.Bray F.Global patterns and trends in colorectal cancer incidence and mortality Gut 66420176836912681861910.1136/gutjnl-2015-310912 · doi ↗ · pubmed ↗
- 3Ogino S.Goel A.Molecular classification and correlates in colorectal cancer J. Mol. Diagn.101200813271816527710.2353/jmoldx.2008.070082 PMC 2175539 · doi ↗ · pubmed ↗
- 4Jasperson K.W.Tuohy T.M.Neklason D.W.Burt R.W.Hereditary and familial Colon cancer Gastroenterology 13862010204420582042094510.1053/j.gastro.2010.01.054PMC 3057468 · doi ↗ · pubmed ↗
- 5Keum N.Giovannucci E.Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies Nat. Rev. Gastroenterol. Hepatol.161220197137323145588810.1038/s 41575-019-0189-8 · doi ↗ · pubmed ↗
- 6Hanahan D.Weinberg R.A.Hallmarks of cancer: the next generation Cell 144520116466742137623010.1016/j.cell.2011.02.013 · doi ↗ · pubmed ↗
- 7Sessions D.T.Kashatus D.F.Mitochondrial dynamics in cancer stem cells Cell. Mol. Life Sci.7882021380338163358083410.1007/s 00018-021-03773-2PMC 11071759 · doi ↗ · pubmed ↗
- 8Bonnay F.Veloso A.Steinmann V.Kocher T.Abdusselamoglu M.D.Bajaj S.Oxidative metabolism drives immortalization of neural stem cells during tumorigenesis Cell 1826202014901507 e 193291613110.1016/j.cell.2020.07.039 · doi ↗ · pubmed ↗