Carelizumab and rivoceranib for advanced extramammary Paget’s disease: an investigator-initiated multicenter, single-arm, phase II trial
Sheng Zhang, Mengyang Ju, Qin Wang, Dongyuan Zhu, Zengjun Liu, Xiongjun Ye, Wenfeng Li

TL;DR
This trial tested a combination of two drugs for a rare cancer called extramammary Paget’s disease but found no significant improvement in patient outcomes.
Contribution
The first clinical trial to evaluate a PD-1 inhibitor combined with a VEGFR inhibitor for advanced extramammary Paget’s disease.
Findings
No patients achieved complete or partial response to the treatment combination.
Median progression-free survival was 2.4 months.
Half of the patients experienced grade 3 adverse events.
Abstract
Extramammary Paget’s disease (EMPD) is a rare cancer without standard therapy. We evaluated the safety and efficacy of a combination of the humanized monoclonal antiprogrammed death-1 (PD-1) antibody, carelizumab, with rivoceranib, a vascular endothelial growth factor receptor (VEGFR) inhibitor, in patients with advanced EMPD. This multicenter, single-arm, phase II trial included 12 patients with EMPD. The primary endpoint is the objective response rate (ORR), defined as the proportion of patients achieving complete response (CR) or partial response (PR) according to RECIST v1.1 criteria. It is hypothesized that the ORR will be less than 10% if the treatment is ineffective and will reach 35% if effective. Secondary endpoints include progression-free survival (PFS) and safety assessments. Eligible patients are aged ≥18 years, with histologically confirmed advanced EMPD. Treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
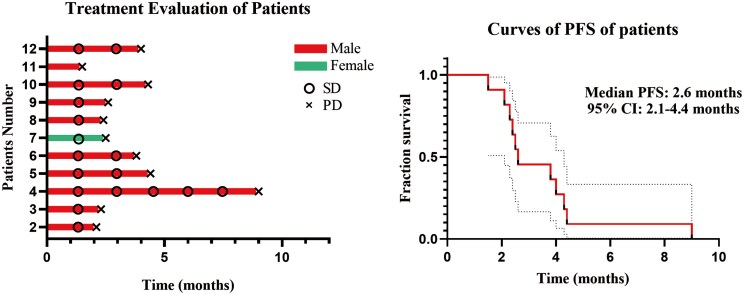 Figure 1
Figure 1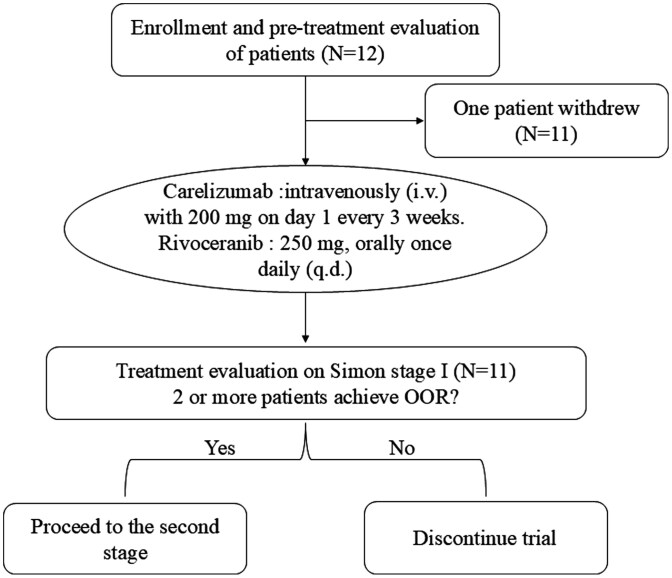 Figure 2
Figure 2|
| Advanced Extramammary Paget’s disease |
|
| IV |
|
| No limitation. |
|
| Phase II |
|
| objective response rate (ORR), defined as the proportion of patients achieving complete response (CR) or partial response (PR)according to RECIST v1.1 criteria. |
|
| progression-free survival (PFS) and safety assessments. |
|
| |
|
| Carelizumab and Rivoceranib |
|
| Hengrui Pharmaceuticals, China |
|
| Carelizumab is an anti-PD-1 monotherapy. Rivoceranib is a VEGFR inhibitor. |
|
| Carelizumab is an ICI. Rivoceranib is a targeted therapy |
|
| Carelizumab 200 mg + Rivoceranib 250 mg |
|
| Carelizumab is intravenous (IV). Rivoceranib is oral. |
|
| 69.5 (60-86) |
|
| 11/1 |
|
| IV (100%) |
|
| |
| Scrotum | 8(67%) |
| Vulva | 3(8%) |
| Penis | 1(25%) |
|
| |
| Yes | 9(75%) |
| No | 3(25%) |
|
| |
| Yes | 6(50%) |
| No | 6(50%) |
|
| |
| 0-2 | 9(75%) |
| >2 | 3(25%) |
|
| |
| Inguinal lymph nodes | 12(100%) |
| Nonlnguinal lymph nodes | 8(67%) |
| Lung | 4(34%) |
| Liver | 6(50%) |
| Bone | 7(58) |
| Yes | 9(75%) |
| No | 3(25%) |
|
| |
| Yes | 6(50%) |
| No | 6(50%) |
|
| |
| 0 | 3(25%) |
| 1 | 9(75%) |
|
| 1(9%) |
|
| 0 |
|
| It is hypothesized that the ORR will be less than 10% if the treatment is ineffective and will reach 35% if effective. Simon’s MinMax 2-stage design was employed, with a power of 80% and a significance level (α) of 0.05. In the first stage, 11 patients were enrolled. If 2 or more patients achieve ORR, the study will proceed to the second stage, where an additional 7 patients will be enrolled, bringing the total to 18 patients. If a combined total of 5 patients achieves ORR across both stages, the study will be considered successful. |
|
| 18 |
|
| 12 |
|
| 11 |
|
| 11 |
|
| The response of patients with measurable target lesions on CT imaging was evaluated according to RECIST version 1.1. The efficacy of those with skin lesions but deemed as not measurable was evaluated according to WHO criteria. Disease progression was defined as the deterioration of the subject’s condition caused by the indication of the study. The progression of imaging and clinical symptoms and signs was included. Disease progression was considered to be the presence of a new metastasis relative to the primary tumor or the progression of an existing metastasis. |
|
| 0/0 |
|
| 0/11 |
|
| |
| Adverse event | Grade 1 | Grade 2 | Grade 3 | % |
|---|---|---|---|---|
| Fatigue | 3 | 5 | 1 | 82 |
| Nausea | 1 | 1 | 0 | 18 |
| Vomiting | 2 | 1 | 0 | 27 |
| Abdominal pain | 1 | 1 | 0 | 18 |
| Diarrhea | 1 | 2 | 0 | 27 |
| Skin and subcutaneous tissue disorders | 2 | 4 | 1 | 64 |
| Constipation | 0 | 2 | 0 | 18 |
| Cough | 0 | 1 | 0 | 9 |
| Dry skin | 2 | 1 | 1 | 36 |
| Dyspnea | 0 | 0 | 0 | 0 |
| Edema limbs | 0 | 0 | 0 | 0 |
| Flank pain | 1 | 1 | 0 | 18 |
| Flu-like symptoms | 0 | 0 | 0 | 0 |
| Musculoskeletal and connective tissue disorder | 1 | 2 | 0 | 27 |
| Noncardiac chest pain | 0 | 1 | 0 | 9 |
| Anemia | 0 | 0 | 0 | 0 |
| Hypertension | 4 | 2 | 2 | 73 |
| Sciatic pain | 0 | 0 | 0 | 0 |
| Tachycardia | 3 | 1 | 1 | 45 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Polyomavirus and related diseases · Advanced Antenna and Metasurface Technologies
Trial information
**: **
Drug information
**: **
Patient characteristics
**: **
Primary assessment method
**: **
(A) The timeline of the treatment evaluation among 11 patients who completed at least 2 cycles. (B) PFS of the 11 patients who completed at least 2 cycles. Abbreviations: PD, progression disease; SD, stable disease.
General toxicity profile
Common and grade 3 or higher adverse events observed with the combination therapy
**: **
Discussion
Extramammary Paget’s disease (EMPD) is a rare epithelial malignancy, primarily occurring in the skin with rich apocrine glands, including vulva, scrotum, penis, and axilla.^1^ EMPD tends to be indolent and is often identified as carcinoma in situ at the time of diagnosis.^2^ However, when distant metastases occur, 5-year survival rates are <10%.^3^ For now, there have not been established treatments for metastatic EMPD, and treatment experience is based on case reports or small case series. Chemotherapy regimens, such as docetaxel, fluoropyrimidines, S-1, platins, and their combination therapy, are attempted and achieve limited progress.^4^ In general, the treatment efficacy is limited with the risk of adverse effects. Therefore, it is essential to find more effective and tolerable treatment options for advanced EMPD.
The programmed death-1 (PD-1)/PD-L1 pathway is crucial for the normal physiological regulation and suppression of immune responses in healthy tissues. Numerous tumors manage to evade immune detection and attack by increasing their PD-L1 expression. Humanized monoclonal antibodies targeting PD-1 and PD-L1 have demonstrated both safety and efficacy in treating a variety of cancers.^5^ We noticed several researchers have published case reports about the role of immune-checkpoint-inhibitors monotherapy in patients with EMPD.^6-8^ But the conclusions are conflicting and there is still a lack of clinical trials to provide higher-quality evidence. Furthermore, the treatment landscape for the combination of ICI and vascular endothelial growth factor receptor (VEGFR) inhibitor for EMPD remains underexplored, particularly there has been substantial evidence that the combination has a significant synergistic anticancer effect in various kinds of solid tumors.^9^ Research indicates that combining carelizumab, with rivoceranib, significantly decreases peripheral blood regulatory T cell (Treg) levels and increases the effector T cell (Teff) to Treg ratio. Additionally, the combination appears to enhance objective tumor response rates while maintaining the durability of immunotherapy. Consequently, numerous clinical trials have been conducted on this combination therapy, targeting advanced cancers such as hepatocellular carcinoma, lung cancer, intrahepatic cholangiocarcinoma, gastric adenocarcinoma, triple-negative breast cancer, and other solid tumors. These studies have investigated the safety, tolerability, and preliminary efficacy of camrelizumab in combination with rivoceranib across various malignancies.^10-12^
Thus, we hypothesized the combination of the PD-1 antibody, carelizumab, with the VEGFR inhibitor, rivoceranib, would be a potential strategy for patients with advanced EMPD. To our knowledge, this is the first clinical trial to investigate the objective response rate (ORR) and safety profile of this combination therapy in patients with advanced EMPD. Figure 2 shows the study schema.
Study schema.
The primary endpoint is the ORR, defined as the proportion of patients achieving complete response or partial response according to RECIST v1.1 criteria. Secondary endpoints include progression-free survival (PFS) and safety assessments. Patients receive carelizumab intravenously (i.v.) with 200 mg on day 1 every 3 weeks. The administration regimen for rivoceranib is as follows: 250 mg, orally once daily (q.d.), to be taken within half an hour after a meal, with continuous dosing. The treatment cycle is for 3 weeks. If tolerated, the dose can be escalated to a maximum of 500 mg q.d. Treatment was continued until documented disease progression, development of unacceptable level of toxic effects, withdrawal of consent, or decision by investigator to discontinue treatment.
From June 2024 to March 2025, 12 patients were enrolled (see Patient characteristics table). Median age was 69.5 years (range 60-86 years). 11 patients (92%) are male, and 1 patient (8%) is female. All patients had EMPD histology and were diagnosed as advanced EMPD. Primary tumor locations included vulva in 1 patient, scrotum in 8 patients, and penis in 3 patients. Metastatic sites included inguinal lymph nodes in all 12 patients, and noninguinal lymph nodes in 8 patients. Also, there are pulmonary metastases in 4 patients, liver metastases in 6 patients, and bone metastases in 7 patients. The median number of previous chemotherapy lines of treatment was 2 (range 1-6). Nine patients (75%) received prior surgery, and radiotherapy as a previous line of therapy for 6 patients (50%).
We found that camrelizumab in combination with rivoceranib was tolerated in this study with no immune-related adverse events reported. Unfortunately, this clinical trial did not show clinical activity for the combination in patients with advanced EMPD. All patients discontinued the combination therapy because of disease progression. One patient achieved stable disease for 9 months. The median PFS is 2.4 months, 95% CI, 2.1-4.4 months (Figure 1). Per study protocol, at least 2 objective responses were required to continue enrolling on the second stage of the study; therefore, the trial was closed at the completion of the first stage.
The main reason for the negative result may be the lack of PD-1/PDL1 expressions. Only one patient was identified as PD-L1 positive. In fact, there is still limited understanding of the relationship between EMPD and PD-1/PDL1 expression. A study evaluated PD-L1 expressions in 18 EMPD surgical pathology cases. PD-L1 was found in 3 cases (17%), including 2 of 4 invasive cases (50%) and 1 of 14 noninvasive cases (7%). Invasive cases with lymph node metastasis also showed PD-L1 expression. TAI cells had higher PD-L1 positivity (83%) compared to tumor cells (17%).^13^ Goto et al. investigated the relationship between EMPD and PD-L1/PD-1 expression in 39 Japanese EMPD patients using immunohistochemical staining. Results showed that Paget’s cells did not express PD-L1, but some tumor-infiltrating mononuclear cells (TIMCs) expressed PD-L1 and PD-1. However, no correlation was found between PD-L1/PD-1 expression in TIMCs and patient characteristics. The study concluded that further clinical research is needed to explore other immune escape pathways in EMPD.^14^ A study investigates the Warburg effect in EMPD, finding that elevated glycolytic enzymes like LDHA are associated with increased immunosuppressive cells and cytokines.^15^ These studies suggest that the tumor microenvironment of EMPD leads to immunotherapy resistance, suggesting that EMPD patients have a poor response to immunotherapy, which is consistent with our observation.
In conclusion, this is the first reported clinical trial evaluating carelizumab in combination with rivoceranib in advanced EMPD. This combination did not demonstrate clinical benefit in this cohort of patients with advanced EMPD. Further investigation requires evaluation of the mechanism of resistance and a possible new combination strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kibbi N , Owen JL, Worley B, et al Evidence-based clinical practice guidelines for extramammary Paget disease. JAMA Oncol. 2022;8:618-628. https://doi.org/10.1001/jamaoncol.2021.714835050310 · doi ↗ · pubmed ↗
- 2Fukuda K , Funakoshi T. Metastatic extramammary Paget’s disease: pathogenesis and novel therapeutic approach. Front Oncol.2018;8:38. https://doi.org/10.3389/fonc.2018.0003829503810 PMC 5820294 · doi ↗ · pubmed ↗
- 3Joshi TP , Dokic Y, Shimizu I. Epidemiology of extramammary Paget’s disease among Asian-American subgroups: a surveillance, epidemiology, and end results (SEER) program-based analysis. J Am Acad Dermatol.2024;91:567-569. https://doi.org/10.1016/j.jaad.2024.05.02538763292 · doi ↗ · pubmed ↗
- 4Hatta N , Ogata D, Asai J, et al Recent treatment and prognosis in 643 patients with extramammary Paget’s disease. Exp Dermatol.2024;33:e 15030. https://doi.org/10.1111/exd.1503038375900 · doi ↗ · pubmed ↗
- 5Chamoto K , Yaguchi T, Tajima M, Honjo T. Insights from a 30-year journey: function, regulation and therapeutic modulation of PD 1. Nat Rev Immunol.2023;23:682-695. https://doi.org/10.1038/s 41577-023-00867-937185300 · doi ↗ · pubmed ↗
- 6Guercio BJ , Iyer G, Kidwai WZ, et al Treatment of metastatic extramammary paget disease with combination ipilimumab and nivolumab: a case report. Case Rep Oncol.2021;14:430-438. https://doi.org/10.1159/00051434533790764 PMC 7983595 · doi ↗ · pubmed ↗
- 7Narasaki M , Kato J, Sato S, et al Extramammary Paget’s disease treated with of anti-programmed cell death protein 1 therapy after docetaxel therapy failure. J Dermatol.2025;52:359-362. https://doi.org/10.1111/1346-8138.1750039460493 · doi ↗ · pubmed ↗
- 8Bellahsen-Harrar Y , Boisson M, Louveau B, et al Molecular profiling of anal Paget’s disease and underlying anal adenocarcinoma highlights their common origin. EJC Skin Cancer 2023;1:100002. https://doi.org/10.1016/j.ejcskn.2023.100002 · doi ↗