Extracorporeal photopheresis for pembrolizumab-induced dermatitis: a case report
Veronika Zenderowski, James A Hutchinson, Andreas Brosig, Sebastian Haferkamp, Katharina Kronenberg

TL;DR
Extracorporeal photopheresis (ECP) successfully treated a patient's severe skin reaction caused by cancer immunotherapy, without worsening their cancer outcome.
Contribution
This is the first reported case of ECP used to treat immune-related dermatitis from anti-PD-1 therapy.
Findings
ECP significantly improved dermatitis symptoms and reduced skin lesions in a melanoma patient.
The patient remained cancer-free for 14 months after ECP treatment.
Immune markers stabilized during ECP treatment.
Abstract
Immune-related adverse events (irAE) are common in checkpoint blockade–treated patients and limit its clinical application. Corticosteroids are the first-line therapy for treatment of irAE, but animal models clearly demonstrate that steroids diminish anti-programmed cell death protein 1 (PD-1)-induced tumour immunity. Better strategies to manage irAE while preserving anti-tumour immunity are needed. Extracorporeal photopheresis (ECP) was recently introduced as second-line treatment for steroid-refractory immune checkpoint inhibitor (ICI)-related colitis and hepatitis. Here, we extend the application of ECP to immune-related maculopapular rash after adjuvant anti-PD-1 therapy in a single melanoma patient. The patient’s dermatitis markedly improved after off-label ECP, with a substantial reduction in skin lesions and pruritus scores, and stabilization of immune markers. The patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
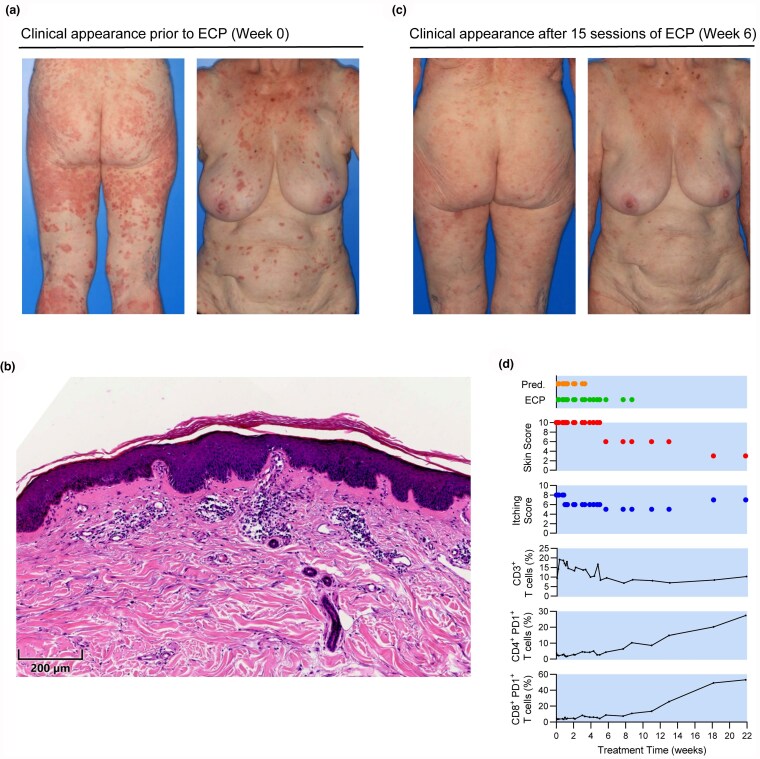 Figure 1
Figure 1- —European Union through the exTra doctoral network
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Immunotherapy and Immune Responses · CAR-T cell therapy research
Although serious immune-related adverse events (irAE) after immune checkpoint inhibitor (ICI) therapy for melanoma are infrequent, they invariably disrupt treatment and may require immunosuppression – conventionally, corticosteroids as first-line, escalating to mycophenolate mofetil, azathioprine, infliximab [α-tumour necrosis factor (TNF)] or vedolizumab (α-integrin α_4_β_7_). Whether steroids limit clinical efficacy of ICI is controversial and possibly depends upon timing;^1,2^ however, mouse models clearly demonstrate that prednisolone, α-TNF and α-α_4_β_7_ are detrimental in α-programmed cell death receptor 1 (PD-1)-induced tumour immunity.^3^ Concerns about irAE risk influence the decision to prescribe adjuvant ICI in stage II melanoma patients, despite KEYNOTE-716 and Checkmate 76 registering improved recurrence-free survival and distant metastasis-free survival.^4,5^ Consequently, there is an urgent need for better strategies to manage irAE caused by α-PD-1 in adjuvant settings, which can control adverse reactions while preserving anti-tumour immunity.^6^
Extracorporeal photopheresis (ECP) is a safe therapy with long-established applications in various T-cell mediated diseases.^7^ The ECP procedure involves collecting autologous peripheral blood leucocytes, which are driven into apoptosis before being reinfused intravenously. ECP acts primarily through in situ exposure of mononuclear phagocytes to apoptotic cells, which then suppress inflammation, promote specific regulatory T-cell responses and retard fibrosis.^8,9^ Because different populations of macrophages and dendritic cells (DC) play diverse, often contradictory roles in immune pathologies, the actions of ECP are context specific. In experimental ICI-induced colitis, the critical action of ECP appears to be reprogramming of tissue macrophages after efferocytosis of apoptotic cells from photopheresates, which then locally suppress inflammation. Accumulating clinical evidence from case reports and a small phase 1b/2 trial supports ECP as a second-line therapy for irAE, especially colitis or hepatitis.^3,10^
Case report
An 83-year-old woman presenting with cutaneous melanoma on the right temple (depth 6 mm, stage IIB) underwent wide local excision and sentinel lymph node biopsy. Histopathological examination and full-body computed tomography (CT) imaging – from the skull to the pelvis – showed no signs of metastatic disease. Adjuvant immunotherapy with 400 mg pembrolizumab at 6-week intervals was initially well-tolerated. After the sixth dose, pruritic skin lesions developed over her entire body that were refractory to topical and systemic corticosteroids; accordingly, pembrolizumab was stopped after eight doses. At this time, the patient exhibited multiple, disseminated erythematous macules and papules across the trunk and upper extremities. Lesions on the upper back had a verrucous appearance, whereas those on the lower legs and thighs were erythematous plaques (Figure 1a). A sharply demarcated erythema extended across the nose and cheeks. Notably, there was no mucosal involvement. The patient reported severe pruritus, rated 8 out of 10 on the Numerical Rating Scale. Excluding other causes, a clinical and histopathological diagnosis of immune-related maculopapular rash [Common Terminology Criteria for Adverse Events (CTCAE) grade 3] was made. Histopathological examination showed moderate lymphocytic inflammatory infiltrates, an increased number of plasma cells and subepidermal edema (Figure 1b). Initial treatment included topical corticosteroids, oral antihistamines and polidocanol-containing topical preparations.
Extracorporeal photopheresis (ECP) treatment of steroid-refractory, Common Terminology Criteria for Adverse Events (CTCAE) grade III dermatitis caused by adjuvant pembrolizumab therapy in an 83-year-old patient with stage IIB melanoma. (a) Clinical appearance prior to ECP. (b) Haematoxylin and eosin (H&E) staining of lesional skin biopsy pre-ECP showing an unremarkable epidermis. The upper dermis reveals moderately pronounced lymphocytic infiltrates, increased plasma cells and subepidermal edema, consistent with non-specific dermatitis. (c) Clinical appearance after 6 weeks of ECP. (d) Improvement in skin lesions and symptoms allowed weaning of prednisolone (Pred.) within 4 weeks of starting ECP. Peripheral T cell subset distributions were monitored with established methods.20 Notably, clinical improvement coincided with a stabilization of peripheral T cell frequencies and preceded pembrolizumab clearance.
Owing to her dermatitis, the patient was hospitalized twice for high-dose prednisolone therapy. Initially, she received 50 mg daily (body weight: 60 kg), tapered by 10 mg every 3 days. During the second admission, treatment was intensified to 70 mg daily with tapering every 3–5 days. However, this regimen failed to improve her symptoms. A decision was made to commence off-label ECP treatment, beginning with an intensive phase of six sessions over 2 weeks and twice-weekly sessions thereafter. ECP was initially performed using a Sheldon catheter. After 2 weeks, treatment was continued in an outpatient setting using peripheral venous access. Following marked improvement, oral prednisolone was stopped by 4 weeks and ECP was reduced to once-weekly sessions. ECP was terminated at 9 weeks with a substantial reduction in skin lesion and pruritus scores (Figure 1c, d). Immune monitoring revealed a rapid stabilization of peripheral blood T cell frequency after 4–5 weeks of ECP that coincided with clinical improvement. Notably, skin lesions and itching began to improve before pembrolizumab was cleared, as shown by the increasing frequency of PD-1^+^ T cells after 8 weeks. This suggests that the drug was still bound to PD-1 receptors and that clinical improvement occurred despite its continued presence in the system.
CT imaging during ECP showed no detectable metastases. A follow-up PET-CT scan at 14 months after starting ECP revealed no signs of recurrent or metastatic disease, or other abnormalities. S100 was monitored at 3-month intervals and remained with its normal range. An intriguing feature of ECP as an immunosuppressive therapy is its ability to control pathological T cell responses without compromising protective immunity.^11^ This apparently paradoxical effect is exploited in solid organ transplantation when minimizing conventional immunosuppression to treat opportunistic infections or post-transplant lymphoproliferative disorder.^12–14^ Moreover, when used in cutaneous T cell lymphoma, ECP enhances cytotoxic T cell (CTL) responses against tumour antigens, which is vital for its therapeutic effect.^15^ Priming of CD8^+^ T cells against viral and other tumour antigens is now a well-documented phenomenon after ECP, but its mechanism is not properly understood.^16,17^ It appears that monocytes present in ECP products become DC-like and acquire a capacity for cross-presentation of phagocytosed antigens to CD8^+^ T cells;^18^ however, it is not certain that such monocytes engraft in patients after reinfusion or whether they interact with T cells. As in other contexts, we speculate that ECP-treated monocytes deliver antigens and apoptotic signals to marginal zone DC and splenic red pulp macrophages, enhancing their cross-presenting ability.^19^ It is interesting to think that ECP might both suppress α-PD-1-induced inflammation and promote specific CTL responses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Luo J, Beattie JA, Fuentes P et al Beyond steroids: immunosuppressants in steroid-refractory or resistant immune-related adverse events. J Thorac Oncol 2021; 16:1759–64.34265432 10.1016/j.jtho.2021.06.024PMC 8464489 · doi ↗ · pubmed ↗
- 2Horvat TZ, Adel NG, Dang TO et al Immune-related adverse events, need for systemic immunosuppression, and effects on survival and time to treatment failure in patients with melanoma treated with ipilimumab at Memorial Sloan Kettering Cancer Center. J Clin Oncol 2015; 33:3193–8.26282644 10.1200/JCO.2015.60.8448 PMC 5087335 · doi ↗ · pubmed ↗
- 3Braun LM, Giesler S, Andrieux G et al Adiponectin reduces immune checkpoint inhibitor-induced inflammation without blocking anti-tumor immunity. Cancer Cell 2025; 43:269–91.e 19.39933899 10.1016/j.ccell.2025.01.004 · doi ↗ · pubmed ↗
- 4Kirkwood JM, Del Vecchio M, Weber J et al Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 Check Mate 76K trial. Nat Med 2023; 29:2835–43.37845511 10.1038/s 41591-023-02583-2PMC 10667090 · doi ↗ · pubmed ↗
- 5Luke JJ, Ascierto PA, Khattak MA et al Pembrolizumab versus placebo as adjuvant therapy in resected stage IIB or IIC melanoma: final analysis of distant metastasis-free survival in the phase III KEYNOTE-716 study. J Clin Oncol 2024; 42:1619–24.38452313 10.1200/JCO.23.02355 PMC 11095869 · doi ↗ · pubmed ↗
- 6Hutchinson JA, Kronenberg K, Riquelme P et al Virus-specific memory T cell responses unmasked by immune checkpoint blockade cause hepatitis. Nat Commun 2021; 12:1439.33664251 10.1038/s 41467-021-21572-y PMC 7933278 · doi ↗ · pubmed ↗
- 7Cho A, Paulitschke V, Knobler R. Mode of action, indications and recommendations on extracorporeal photopheresis (ECP). J Dtsch Dermatol Ges 2023; 21:1369–80.10.1111/ddg.1516737723908 · doi ↗ · pubmed ↗
- 8Maeda A, Schwarz A, Kernebeck K et al Intravenous infusion of syngeneic apoptotic cells by photopheresis induces antigen-specific regulatory T cells. J Immunol 2005; 174:5968–76.15879089 10.4049/jimmunol.174.10.5968 · doi ↗ · pubmed ↗