Comparative survival outcomes of minimally invasive versus open radical nephroureterectomy for upper tract urothelial carcinoma in Taiwan
I-Hsuan Alan Chen, Wei-Ming Li, Hung-Lung Ke, Yi-Huei Chang, Chao-Hsiang Chang, Yao-Chou Tsai, Chih-Chin Yu, Wun-Rong Lin, Marcelo Chen, Yi-Hsin Lu, Chia-Cheng Yu

TL;DR
Minimally invasive surgery for upper tract urothelial carcinoma in Taiwan shows better survival outcomes than open surgery.
Contribution
Demonstrates that minimally invasive radical nephroureterectomy improves survival outcomes compared to open surgery in UTUC patients.
Findings
Minimally invasive surgery showed significantly improved overall survival compared to open surgery.
Disease-free and cancer-specific survival were also better in the minimally invasive group.
MIS outcomes were maintained despite higher prevalence of high-grade tumors in MIS patients.
Abstract
Upper tract urothelial carcinoma (UTUC) is rare globally but accounts for 30–40% of urothelial cancers in Taiwan. Radical nephroureterectomy (RNU) with bladder cuff excision (BCE) remains the standard of care for localized or locally advanced disease. Despite the increasing adoption of minimally invasive surgical (MIS) approaches, concerns about their oncological outcomes persist. This study evaluates the comparative survival outcomes of MIS versus open RNU for UTUC using propensity-score-matched (PSM) analysis. Data from 2430 patients with UTUC, treated between 1988 and 2022 within the Taiwan UTUC Collaboration Group, were retrospectively analyzed. PSM was employed to minimize baseline differences. The primary endpoints were overall survival (OS), cancer-specific survival (CSS), and disease-free survival (DFS). Kaplan-Meier estimates, stratified log-rank tests, and Cox proportional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
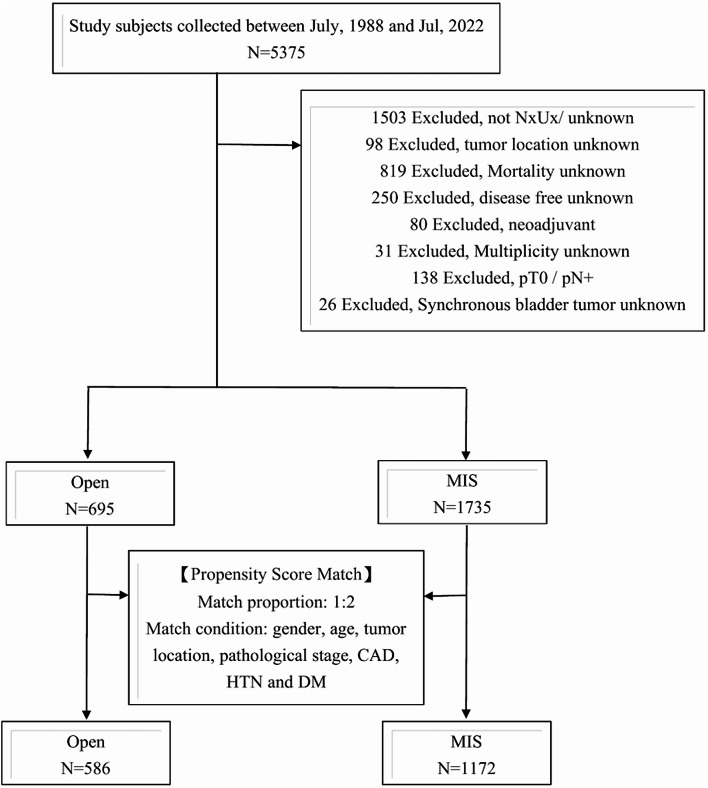 Figure 1
Figure 1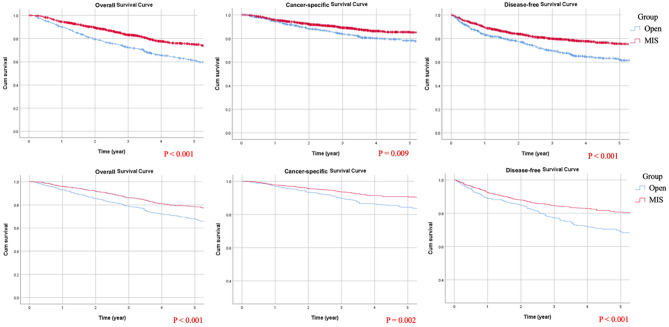 Figure 2
Figure 2- —National Yang Ming Chiao Tung University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Esophageal Cancer Research and Treatment
Introduction
Upper tract urothelial carcinoma (UTUC) is relatively rare worldwide; however, it represents a significant proportion of urothelial cancers in Taiwan, accounting for approximately 30–40% of cases [1]. Radical nephroureterectomy (RNU) with bladder cuff excision (BCE) remains the established gold standard for managing localized or locally advanced UTUC. Since the introduction of laparoscopic RNU in 1991 [2] and robotic RNU in 2007 [3], minimally invasive surgical (MIS) approaches have been widely adopted, revolutionizing the management of UTUC over the past two decades.
The benefits of minimally invasive surgery, including reduced intraoperative blood loss, shorter hospital stays, decreased perioperative morbidity, and faster postoperative recovery, are well-documented. However, debate persists regarding the oncological outcomes of MIS compared to traditional open surgery. A systematic review by the European Association of Urology suggests that conventional open RNU [4] offers superior oncological control compared to laparoscopic RNU, particularly in high-risk cases of locally advanced UTUC where laparoscopic bladder cuff excision is performed [5]. Conversely, a meta-analysis found no significant difference in oncological outcomes between open and laparoscopic RNU, even in cases of locally advanced disease [6]. Further support for MIS comes from a propensity-matched analysis of the National Cancer Database (NCDB), which reported improved overall survival (OS) in octogenarians undergoing MIS (both laparoscopic and robotic RNU) after a median follow-up of 39.4 months [4].
Within the Taiwanese UTUC Collaboration Group, 72% of patients treated between August 1988 and April 2021 underwent minimally invasive RNU, with a marked increase in MIS adoption observed after 2000 [7]. Multivariate analyses identified MIS approaches—specifically laparoscopic, hand-assisted laparoscopic, and robotic RNU—as favorable predictors of OS. Notably, laparoscopic RNU alone was found to be an independent predictor of reduced cancer-related mortality. To further investigate the potential survival advantages of MIS compared to conventional open procedures, we performed a propensity-score-matched (PSM) multivariable survival analysis, comparing OS and cancer-specific survival between MIS and open RNU.
This study aims to provide robust evidence comparing the survival outcomes of MIS and open RNU for UTUC, with the goal of informing surgical decision-making and enhancing the understanding of MIS’s role in oncological control for UTUC.
Materials and methods
Patient population
This study, conducted by the Taiwan UTUC Collaboration Group, was reviewed and approved by the Kaohsiung Veterans General Hospital Institutional Review Board (IRB No.: VGHKS14-CT3-06). A total of 5375 patients with upper tract urothelial carcinoma (UTUC), enrolled between July 1988 and July 2022, were considered for inclusion. Of these, 2430 patients who underwent open or MIS RNU with bladder cuff excision were ultimately included in the analysis. The procedures were performed between August 9, 1988, and February 17, 2022. To ensure data completeness and analytical robustness, stringent exclusion criteria were applied (Fig. 1). Patients with incomplete data were excluded, and no imputation was performed, resulting in fully complete datasets for all extracted variables.
Fig. 1. Study flowchart
Patient demographics, postoperative complications, and their grading (based on the Clavien-Dindo classification) were recorded. Tumor location and size were determined from post-RNU specimen evaluations, with multifocality defined as the presence of two or more pathologically confirmed lesions at distinct anatomical sites (renal pelvis or ureter). Tumor size was measured as the sum of the longest diameters of all detected tumors. Preoperative hydronephrosis was assessed using computed tomography (CT) or magnetic resonance imaging (MRI). Pathological features—including tumor cell type, carcinoma in situ (CIS), lymphovascular invasion (LVI), tumor necrosis, and surgical margins—were reviewed by urological pathologists. Histological grading adhered to the 1973 and 2004 World Health Organization classification, while pathological staging was performed according to the 2017 AJCC TNM staging system. Additionally, the presence and timing of bladder UC were documented.
Survival assessment
The primary endpoint of this study was to compare oncological outcomes between the open and MIS groups, specifically evaluating OS, cancer-specific survival (CSS), and disease-free survival (DFS). For the CSS analysis, patients who died within 30 days of RNU or during the same hospital stay were censored at the time of death. DFS was defined as the time from RNU to the first documented occurrence of local recurrence at the tumor bed, lymph node involvement, or distant metastasis, with recurrence and metastasis confirmed through radiological or pathological evaluation. Intravesical recurrence (IVR) was defined as any histologically confirmed bladder UC occurring at least 3 months post-RNU. All survival outcomes were analyzed using multivariate Cox proportional hazards models.
Statistical method
Group differences were assessed using the Pearson Chi-square test for categorical variables, while normality of continuous variables was evaluated using the Student’s t-test. To address potential imbalances in confounding factors between the open and MIS RNU groups, propensity score matching was employed. Propensity scores were estimated using a logistic regression model, with surgical status as the dependent variable and baseline covariates—including gender, age, tumor location, pathological stage, coronary artery disease (CAD), hypertension, and diabetes mellitus (DM)—as predictors. Matched pairs were created between the groups using nearest-neighbor propensity-score matching, with tolerance levels set at 0.001 and 0.002.
Our study utilized one-to-two propensity score matching to form pairs of control and treated subjects with similar propensity scores. Prognostic outcome rates were estimated using the Kaplan-Meier method, and survival curves were compared with the stratified log-rank test. The effect of surgical approaches on prognostic outcomes was assessed using a Cox proportional hazards model, both unadjusted and adjusted for potential confounders. All statistical tests were two-tailed, with a significance threshold set at p < 0.05. Statistical analyses were conducted using IBM SPSS Statistics, version 26.
Results
A total of 2430 patients were included in the study (Table 1). Of these, 1735 (71.4%) underwent MIS RNU, while 695 (28.6%) underwent open RNU. The age distribution was comparable between the two groups. Comorbidity analysis revealed a higher prevalence of CAD, arrhythmia, and DM among patients in the MIS group. There were no significant differences between groups regarding tumor location, multiplicity, pathological T staging, synchronous bladder tumors, or receipt of adjuvant treatment.
Table 1. Baseline demographic data of variables the UTUC patientsVariablesOverallPropensity score matchedOpen(N = 695MIS(N = 1735p value^a^Open(N = 586MIS(N = 1172p value^a^N%N%N%N%Gender Men31945.975243.30.25125844.051343.80.919 Women37654.198356.732856.065956.2Age < 7040759.294854.90.05433557.270460.10.244 ≥ 7028040.877845.125142.846839.9Comorbidity CAD263.817510.2< 0.001264.4524.41.000 Arrythmia26638.894455.2< 0.00126545.252044.40.734 HTN9213.421712.70.6298714.815012.80.236 DM12718.545826.8< 0.00112521.326522.60.543 Malignancy (no UTUC/bladder UC)7410.820812.20.3486911.815513.20.390Cell type Urothelial64692.9159391.80.63054092.2107091.30.698 UC with variants446.31297.4417.0948.0 Others50.7130.750.980.7Laterality Left35050.687850.60.99029951.060251.40.893 Right34249.485749.428749.057048.6Tumor location Renal pelvis31345.279345.70.92226745.651744.10.847 Ureter24935.962636.121236.243537.1 Renal pelvis + ureter13118.931618.210718.322018.8Multifocality No45064.9111464.60.86938365.474864.20.634 Yes24335.161135.420334.641735.8RNU histology Low grade649.424013.9< 0.001589.914112.1< 0.001** High grade47069.3144483.541070.299785.3 G214421.2452.611619.9312.7Pathological stage T pTis/pTa/pT129945.378745.60.08126845.753345.50.116 pT214321.735620.612521.3234(20.0 pT318628.253831.216828.737632.1 pT4324.8442.6254.3292.5Urinary bladder tumor No50172.2132576.50.05342873.088875.90.109 Previous history of bladder UC588.41076.2508.5695.9 Concurrent Bladder UC13519.530117.410818.421318.2CIS No59187.8133177.3< 0.00151087.086273.8< 0.001 Yes8212.239022.77613.030626.2Lymphovascular invasion No57284.0138781.70.19148883.494082.40.590 Yes10916.031018.39716.620117.6Surgical margin Free63796.5167297.00.55856596.4113797.00.501 Positive233.5523.0213.6353.0Tumor necrosis No59093.7140382.9< 0.00152993.695883.1< 0.001 Yes406.328917.1366.419516.9Adjuvant chemotherapy No58684.3144083.00.43049684.695581.50.100 Yes10915.729517.09015.421718.5Adjuvant radiation therapy No67497.0168296.90.96656997.1113797.00.921 Yes213.0533.1172.9353.0RNU date Before the end of 201037253.528816.6< 0.00128749.013911.9< 0.001 After the start of 201132346.5144783.429951.0103388.1Bladder-cuff excision Open incision53477.2106963.5< 0.00144175.671462.9< 0.001 Transurethral incision15722.71508.914124.21109.7 Laparoscopy10.128316.810.217915.8 Robot assisted00.017610.500.013011.4 LESS00.050.300.030.3Clavien-Dindo classification No49973.1105964.50.00441571.769063.00.008 Grade I578.318211.1518.812911.8 Grade II10715.733120.19316.123221.2 Grade III91.3402.491.6282.6 Grade IV91.3261.691.6151.4 Grade X20.350.320.310.1Mortality No28040.3121570.0< 0.00125643.788075.1< 0.001 UTUC related16123.226215.112220.815513.2 Non-UTUC related25236.325214.520635.213511.5 Surgery related20.360.320.320.2Disease free No21330.640123.1< 0.00116828.725421.70.001 Yes48269.4133476.941871.391878.3IVR after RNU No49471.1121870.20.66842171.883070.80.655 Yes20128.951729.816528.234229.2Complication ESRD608.818610.90.132549.31089.30.983 Ileus71.0372.20.06261.0252.20.094 Ventral hernia20.3382.20.00120.3221.90.009 Follow up (months) ^c^54.444.60.00656.141.6< 0.001Median (IQR)22.8–103.725.6–76.324.3–102.424.5–70.7Following a median follow-up of 54.4 months, 1215 (70%) patients in the MIS group remained alive without disease recurrence, and 1334 (76.9%) were disease-free. In comparison, after a median follow-up of 44.6 months, 482 (69.4%) patients in the open RNU group were recurrence-free, and 280 (40.3%) were still alive. The use of MIS surged from 16.6% before the end of 2010 to 83.4% after the start of 2011, while the proportion of open RNU cases steadily declined, reaching 46.5% since 2011^a^Chi-Squared test calculated for the difference Variables. ^b^ Student’s t-test calculated for the difference in means. ^c^ Wilcoxon rank-sum test calculated for the difference in medians. * < 0.05, ** < 0.01
Propensity-score matching analysis
PSM was performed to compare MIS and open RNU cases, with each open RNU patient matched to two MIS patients. This resulted in a cohort of 1172 (66.7%) MIS patients and 586 (33.3%) open RNU patients. After matching, baseline characteristics—including gender, age, tumor location, pathological T stage, and comorbidities—were balanced between the two groups. Despite a higher proportion of patients with high-grade UC, concomitant CIS, and tumor necrosis in the MIS group, these patients demonstrated improved survival outcomes, including OS, CSS, and DFS. Adjusted Kaplan-Meier survival estimates are presented in Fig. 2. While MIS RNU was associated with improved survival outcomes, it was also linked to a higher incidence of postoperative morbidities requiring intervention.
Fig. 2. Kaplan–Meier survival curves: unadjusted (top row) and adjusted (bottom row) analyses for overall survival, cancer-specific survival, and disease-free survival
Univariable adjustment
In the PSM univariate analysis of OS, CSS, and DFS, significant favorable predictors included the MIS approach, age below 70, negative surgical margins, and surgical dates after January 2011. Unfavorable predictors included ureteral and multifocal UC, concurrent bladder UC, LVI, tumor necrosis, advanced pathological T staging, and receipt of adjuvant radiotherapy (Supplementary Table 1).
Multivariable adjustment
The PSM-adjusted multivariable analysis revealed that patients undergoing MIS had significantly better survival outcomes compared to those undergoing open RNU, with longer OS (odds ratio [OR]: 0.662; p < 0.001), CSS (OR: 0.659; p = 0.002), and DFS (OR: 0.646; p < 0.001) (Supplementary Table 2. Adverse predictors of survival included ureteral UC, concurrent bladder UC, positive surgical margins, LVI, tumor necrosis, and advanced pathological T staging.
Discussion
In the present study, the original cohort showed better OS, CSS, and DFS with the MIS approach for patients with UTUC. After balancing baseline characteristics, potential confounders—including sex, age, tumor location, pathologic T stage, and comorbidities—were comparable between the open and MIS groups. Despite a higher prevalence of adverse pathologic features (high-grade urothelial carcinoma, tumor necrosis, and carcinoma in situ) in the MIS group, PSM analysis still indicated that MIS may provide superior oncologic control compared with open RNU. Notably, both before and after PSM, a higher proportion of high-grade disease was presented in the MIS group. Multivariate analyses showed that tumor grade was not an independent predictor of overall survival, consistent with our previous findings [7].
Surgical margin status remains a critical prognostic factor. A multicenter database previously identified margin status as an independent predictor of metastasis-free survival after RNU [8]. Ditonno et al. recently reported a 4.7% positive margin rate among over 1100 patients in the ROBotic surgery for Upper tract Urothelial cancer STtudy (ROBUUST) 2.0 database who underwent robotic RNU [9]. In the current study, comparable positive margin rates were observed in the MIS and open groups (3.0% vs. 3.6%, respectively). Likewise, Rajan et al. found lower positive margin rates with robotic versus open or laparoscopic RNU in well-balanced studies [10], and Trecarten et al. linked MIS to reduced positive margin rates and lower 90-day mortality [4]. On the other hand, a meta-analysis by Veccia et al. showed that open RNU had the poorest 5-year CSS among 87,291 patients [11]. Despite limitations in the quality of evidence comparing surgical approaches for UTUC, an increasing body of data supports comparable or even superior survival outcomes with the MIS approach. A prior analysis comparing robotic and laparoscopic RNU was conducted based on the Taiwanese UTUC collaboration cohort [12]. Baseline characteristics were balanced using the overlap weighting method, and perioperative as well as survival outcomes were comparable between both groups.
Management of the distal ureter and bladder cuff is pivotal for oncologic control. Our study reflects contemporary Taiwanese practice, employing transurethral incision and open, laparoscopic, or robotic BCE. Because a deep, narrow pelvis can hamper MIS distal ureteral dissection, surgeons often adopt a hybrid technique. Consequently, IVR did not differ between groups; however, MIS—including laparoscopic BCE (15.8%) and robotic BCE (11.4%)—was associated with fewer systemic recurrences. The likely advantage stems from superior visualization and precise manipulation, permitting complete bladder-cuff resection and reducing residual ureteral stump risk [13]. Data from 17 centers (185 robotic and 91 laparoscopic cases) showed a higher likelihood of adequate BCE with robotic surgery [14]. MIS affords unobstructed access to the distal ureter, enabling clear identification of Waldeyer’s sheath, meticulous intramural ureter dissection, watertight cystorrhaphy, and avoidance of urine spillage.
With increased experience in distal ureterectomy and BCE—via open or MIS approaches—surgeons usually encounter two key tubular structures at the distal ureter: (i) the medial umbilical ligament, which crosses anterior to the ureter below its midpoint [15]; and (ii) the superior vesical artery, which traverses the ureterovesical junction. Ligation and division of the superior vesical artery allow caudal ureteral traction, exposing the fibromuscular Waldeyer’s sheath around the intramural segment. The detrusor muscle at the ureteral hiatus can then be sharply divided. This tenting maneuver permits en bloc removal of the intramural ureter and minimizes the risk of a residual stump.
Although Kapoor et al. [16] and Tsuboi et al. [17] reported better IVR-free survival with transvesical versus extravesical BCE, the extravesical technique is increasingly favored in MIS RNU because it shortens operative time. It also avoids cystotomy closure and reduces the risk of tumor-bearing urine spillage. However, inaccurate identification of the distal ureter during extravesical BCE can compromise oncologic control; the magnified, three-dimensional view of MIS, combined with careful attention to anatomic landmarks, mitigates this risk.
This study has several limitations. First, not all patients in the MIS group underwent laparoscopic or robotic intracorporeal BCE. However, our cohort reflects real-world practices in managing UTUC, where patient factors such as obesity or a deep and narrow pelvis can hinder adequate exposure of the distal ureter, necessitating open BCE for proper oncological control. Second, detailed information regarding the use of transvesical or extravesical BCE and the presence of residual ureteral stumps could not be comprehensively assessed due to the multicenter retrospective nature of the study. Variations existed in the BCE technique, and this potential confounder could not be incorporated into the multivariate or propensity-score models. Finally, the MIS approach did not demonstrate a significant advantage in reducing postoperative morbidities. This finding may be attributable to the learning curve and the varying levels of surgical experience across institutions.
Conclusion
This study demonstrates that MIS approaches, including laparoscopic and robotic RNU, may offer superior survival outcomes to open RNU for patients with UTUC. Despite a higher prevalence of adverse pathological features in the MIS cohort, propensity-score-matched analysis revealed significantly improved survival outcomes.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ditonno F, Franco A, Wu Z, Wang L, Abdollah F, Simone G et al (2024) Robot-assisted nephroureterectomy: surgical and mid-term oncological outcomes in over 1100 patients (ROBUUST 2.0 collaborative group). BJU Int 134(6):967–97510.1111/bju.1652639263834 · doi ↗ · pubmed ↗
- 2Rajan K, Khalifa A, Geraghty R, Parmar K, Kanda Swamy G, Gomez Rivas J et al (2023) Oncological efficacy of robotic nephroureterectomy vs. open and laparoscopic nephroureterectomy for suspected non-metastatic UTUC—a systematic review and meta-analysis. Cancers (Basel) 15(20):492610.3390/cancers 15204926 PMC 1060560737894293 · doi ↗ · pubmed ↗
- 3Chang CL, Tsai CY, Cheng PY, Wu WJ, Tsai YC (2025) Robot-assisted radical nephroureterectomy: a safe and effective option for upper tract urothelial carcinoma, especially for novice surgeons. Cancers (Basel) 17(9):139410.3390/cancers 17091394 PMC 1207111240361320 · doi ↗ · pubmed ↗