A case of jejunal cancer arising from ectopic pancreas
Makoto Eizuka, Yosuke Toya, Ryo Sugimoto, Mizuki Komai, Ako Yamada, Taku Kimura, Shunichi Yanai, Naoki Yanagawa, Akira Sasaki, Takayuki Matsumoto

TL;DR
A 74-year-old man was diagnosed with jejunal cancer originating from ectopic pancreatic tissue, highlighting the need to consider this rare condition in submucosal tumor diagnoses.
Contribution
This case report presents a rare instance of cancer arising from ectopic pancreas in the jejunum.
Findings
CT and DBE identified a jejunal mass with mucosal changes and luminal stenosis.
Histopathology confirmed moderately differentiated adenocarcinoma from ectopic pancreatic tissue.
The case emphasizes the importance of considering ectopic pancreas as a potential source of submucosal tumors.
Abstract
A 74-year-old man presented with intestinal obstruction. CT (computed tomography) revealed a 25-mm mass in the proximal jejunum. Double-balloon endoscopy (DBE) identified a smooth, asymmetrically localized mass with oozing and luminal stenosis covered with the mucosa of swollen villi. Small bowel radiography demonstrated jejunal obstruction. Histopathological examination of the resected specimen confirmed moderately differentiated adenocarcinoma arising from ectopic pancreatic tissue of Heinrich type I. Our case suggests that cancer arising from ectopic pancreas should be considered as a candidate diagnosis of a submucosal tumor in the jejunum.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
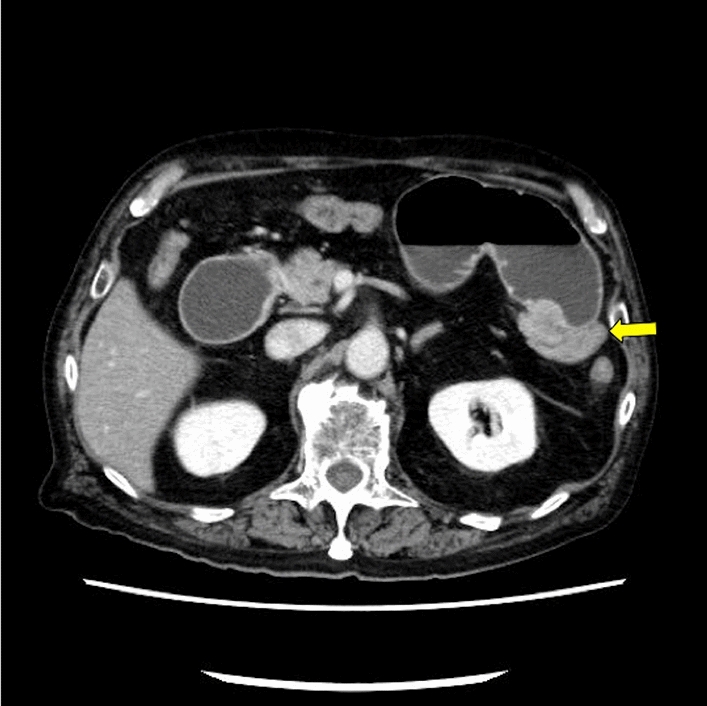 Figure 1
Figure 1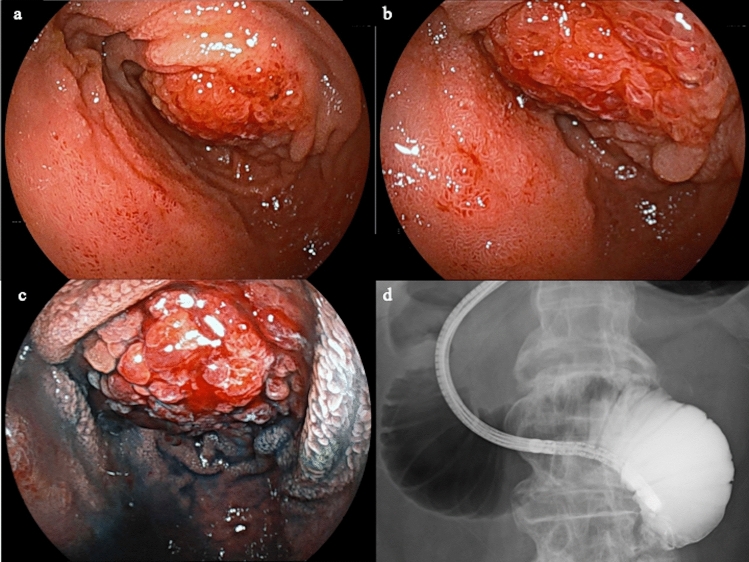 Figure 2
Figure 2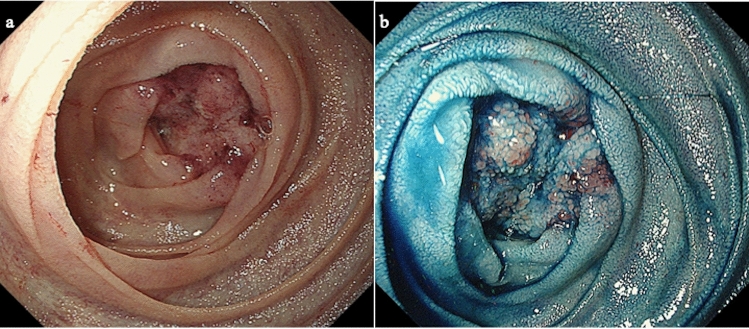 Figure 3
Figure 3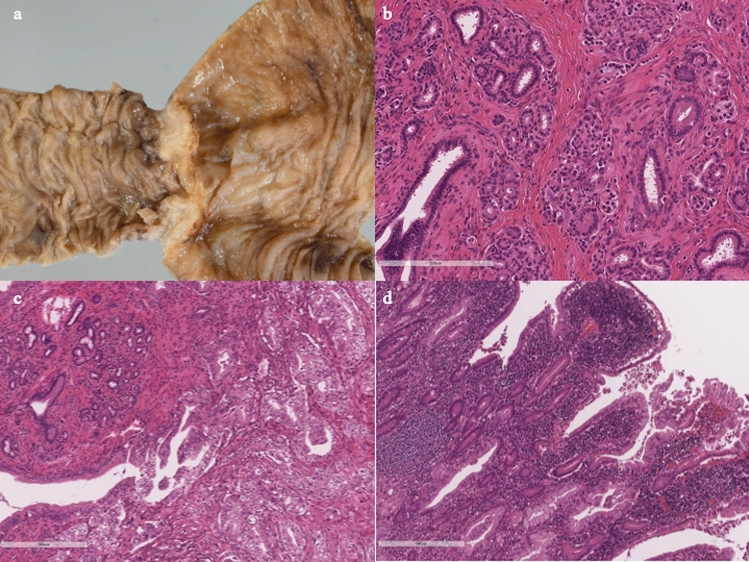 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Esophageal and GI Pathology
Introduction
Ectopic pancreas is a developmental anomaly, which is characterized by the existence of pancreatic tissue in the gastrointestinal tract. It occurs a subepithelial lesion (SEL), particularly in the stomach and in the small intestine [1, 2]. As well as the normal pancreas, ectopic pancreas manifests pancreatitis, cystic formation, and bleeding, and, rarely, it transforms to cancer [3, 4].
We herein report a case of cancer arising from ectopic pancreas in the jejunum, which could be observed endoscopically.
Case presentation
A 74-year-old man visited his neighboring hospital with anorexia, vomiting, and abdominal pain for a month. The patient did not have any specific medical history or medication. Because abdominal CT revealed small bowel dilation, he was admitted with a diagnosis of intestinal obstruction. Although his symptoms transiently relieved, he again complained of vomiting after he started the oral intake. Consequently, he was transferred to our hospital for further evaluation.
On admission, physical examination revealed abdominal distention and epigastric tenderness. Laboratory showed an elevated C-reactive protein (CRP) level of 0.88 mg/dl, an increased CA19-9 level of 684 ng/ml, and a low albumin level of 2.9 g/dl. Hemoglobin value was normal at level of 14.2 g/dl. Contrast enhanced CT identified a high-density mass measuring 25 mm in the jejunum distal to the ligament of Treitz, and proximal bowel dilation. Regional lymph nodes were not enlarged (Fig. 1).Fig. 1. Contrast enhanced computed tomography revealed a 25 mm high-density mass in the jejunum (yellow arrow) with proximal bowel dilation
Double-balloon endoscopy (DBE) revealed a reddish and friable protrusion with luminal narrowing in the jejunum with luminal stenosis (Fig. 2a, b). Chromoendoscopy with indigo carmine revealed enlarged villous structure in the center of the lesion (Fig. 2c). The scope could not pass the narrowing. Small intestinal radiography during oral DBE also demonstrated jejunal obstruction (Fig. 2d).Fig. 2a, b Double-balloon endoscopy revealed a smooth mass in the jejunum with bleeding and asymmetrical luminal stenosis. c Chromoendoscopy with indigo carmine enhanced visualization of enlarged villi. **d **Small intestinal radiography during oral DBE demonstrated jejunal obstruction
Histopathological examination of the biopsy specimens obtained from the villous structure showed non-neoplastic villous epithelium. Because the endoscopic and histologic findings were suggestive of malignant subepithelial tumor, small bowel resection was performed.
During surgery, it was confirmed that the tumor was located in the jejunum, 30 cm distal to the ligament of Treitz. Intraoperative endoscopy from the anal side of the lesion revealed severe stenosis and fold convergence (Fig. 3a). Chromoendoscopy using indigo-carmine enhanced the irregular margin of the depressed area suggesting malignancy (Fig. 3b). Macroscopically, the tumor was a whitish subepithelial lesion-like, measured 15 × 14 mm in size (Fig. 4a). Histopathological examination of the resected specimen revealed pancreatic tissue in the submucosa, including pancreatic ducts, acinar cells, and islets of Langerhans (Fig. 4b), leading to a diagnosis of ectopic pancreas of Heinrich type I. In addition, it was evident that the tumor contained confluent growth of cancer cells with clear cytoplasm, consistent with moderately differentiated adenocarcinoma (Fig. 4c). The tumor was not regarded as a collision of pancreatic tissue and cancer, because areas of transition from ectopic pancreas to carcinoma were found (Fig. 4c). The center of the tumor was covered by villous hyperplasia with the infiltration of predominant lymphocytes in the lamina propria (Fig. 4d). Based on these findings, the tumor was diagnosed as a cancer arising from ectopic pancreas in the jejunum. Because there was a lymph node metastasized with cancer, the final pathological diagnosis was pT4aN1M0, pStage IIIA according to the TNM classification system for malignant tumors [5].Fig. 3a Intraoperative endoscopy from the anal side revealed severe stenosis and fold convergence. b Chromoendoscopy using indigo carmine facilitated the irregular margin of the depressed areaFig. 4a Tumor was a whitish subepithelial lesion-like, measured 15 × 14 mm in size. b Histopathological examination of the resected specimen revealed pancreatic tissue in the submucosa, including pancreatic ducts, acinar cells, and islets of Langerhans (Heinrich type I). c Histopathological examination revealed moderately differentiated adenocarcinoma, with observed areas of transition from ectopic pancreas to cancer. d Inflammatory cell infiltration, mainly consisting of lymphocytes, was observed in the lamina propria
The patient recovered uneventfully after the surgery, and he has been doing well under an adjuvant chemotherapy with S-1 at a daily dose of 120 mg in accordance with the clinical practice guideline for pancreatic cancer [6].
Discussion
While ectopic pancreas can occur anywhere within the gastrointestinal tract, the most common site of involvement has been known to be the stomach, followed by the duodenum, the jejunum and the ileum [7, 8]. In most cases, ectopic pancreas is asymptomatic and is incidentally found during endoscopy or autopsy [9]. Even in symptomatic patients, the symptoms are nonspecific, including abdominal pain, bleeding, or vomiting due to obstruction [4]. However, it should be noted that the pancreatic tissue possibly shows malignant transformation, although the incidence ranges from 0.7 to 1.8% [10] among the autopsy cases. Nevertheless, it still remains obscure whether ectopic pancreas has a higher burden for cancer development when compared to the pancreas [11].
In a literature review of 54 cases of cancer originating from ectopic pancreas, Cazacu IM, et al. reported that the majority of the cases were symptomatic, and they occurred in middle-aged men. In addition, there was a trend that the background ectopic pancreas was classified as Heinrich type I and exhibited a subepithelial-like appearance macroscopically [11]. When we attempted an online search of PubMed during a period from 1995 until 2025, we identified only eight cases of pancreatic cancer arising from an ectopic pancreas in the jejunum, including our present case (Table 1) [9, 12–16]. Such a small number of jejunal cancers in the literature may be explained by the rarity of jejunal ectopic pancreas. In those cases, the tumors occurred in middle-aged or elderly patients. While the symptoms were nonspecific and variable, the tumors were associated with increase in serum CA19-9 levels. In addition, four of the eight tumors had lymph node metastasis or peritoneal dissemination, and four tumors occurred from ectopic pancreas of Heinrich type I.Table 1. Published cases of pancreatic cancer arising from an ectopic pancreas in the jejunumReferenceAge, years, genderSymptomsCA 19–9, U/mlDistance from the ligament of Treitz, cmSize, mmMetastasisHeinrich typeMakhlouf et al. [12]71, maleNone(CT image abnormalities)UnknownUnknown25NoneIMakhlouf et al. [12]61, maleAbdominal pain, vomitingUnknown815PeritoneumIArao et al. [13]63, maleEpigastric discomfort and vomiting6100Unknown40Lymph node and liverIIFujita et al. [14]64, femaleAbdominal distension, epigastric painUnknown4520Lymph nodeUnknownSong et al. [15]74, maleAbdominal pain88.4Unknown30NoneIYamaoka et al. [9]69, femaleNone(CT image abnormalities)635Unknown (100 cm from incisor teeth)28Lymph nodeIIYamamoto et al. [16]76, maleAbdominal distention, vomitingUnknown2035NoneIIOur case74, maleAnorexia, vomiting,abdominal pain6843015NoneICA19-9 carbohydrate antigen 19-9, CT computed tomography
It has been reported that ectopic pancreas in the small bowel is observed as a non-specific, SEL-like lesion under endoscopy [17]. In contrast, there have been only limited descriptions regarding the endoscopic features of jejunal cancer arising from ectopic pancreas. In our case, the boundary of the tumor was observed as SEL-like tumor, suggesting a diagnosis of gastrointestinal mesenchymal tumor, malignant melanoma and metastatic small intestinal tumor [14]. Unlike those small bowel tumors, however, the tumor of our patients had central depression with villous hyperplasia and severe jejunal stricture. These findings may be explained by severe fibrosis induced by desmoplastic reaction to cancer cells and, presumably, repeated inflammation occurring in the pancreatic tissue, particularly the lamina propria. In addition to these endoscopic findings, ectopic pancreatic cancer should be considered as a differential diagnosis in a case of small bowel SEL with intestinal obstruction and elevated serum CA19-9.
In conclusion, we could observe cancer arising from ectopic pancreas by way of enteroscopy. Although this condition is extremely rare, SEL-like tumor accompanied by luminal constriction and surface changes may be characteristic of small bowel cancer originating from ectopic pancreas.