Minimally Invasive Aortic Valve Replacement in a Patient With Interrupted Hepatic Inferior Vena Cava and Duplicated Inferior Vena Cava: A Case Report
Gentaku Hama, McAndrew Merlini, Keijiro Mitube, Tomoya Ohshiro

TL;DR
A 72-year-old woman with a rare vein anomaly successfully underwent minimally invasive heart surgery to replace her aortic valve.
Contribution
This case report presents a successful MICS-AVR in a patient with a rare duplicated and interrupted inferior vena cava.
Findings
MICS-AVR was successfully performed despite a rare vascular anomaly.
Venous cannulation was achieved through alternative routes due to the anomaly.
The patient recovered well and was discharged on postoperative day six.
Abstract
We report a case of a 72-year-old female patient with severe aortic regurgitation and a rare congenital anomaly involving duplicated inferior vena cava (IVC) and interruption at the hepatic segment. She underwent minimally invasive cardiac surgery-aortic valve replacement (MICS-AVR) via right anterior thoracotomy. Venous cannulation was performed through the right internal jugular vein and right femoral vein, while arterial access was achieved through the right femoral artery. Despite suboptimal venous return, cardiopulmonary bypass (CPB) was initiated, and the procedure was completed successfully with hypothermic support. The patient recovered uneventfully and was discharged on postoperative day six. This case highlights the importance of thorough preoperative imaging and intraoperative vigilance when dealing with vascular anomalies in MICS.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1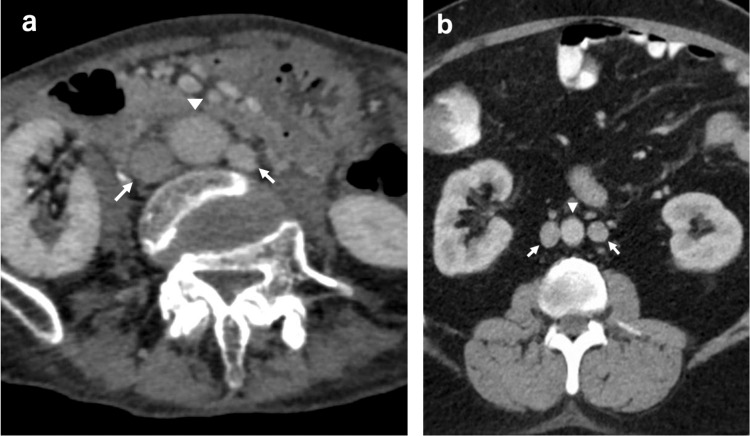 Figure 2
Figure 2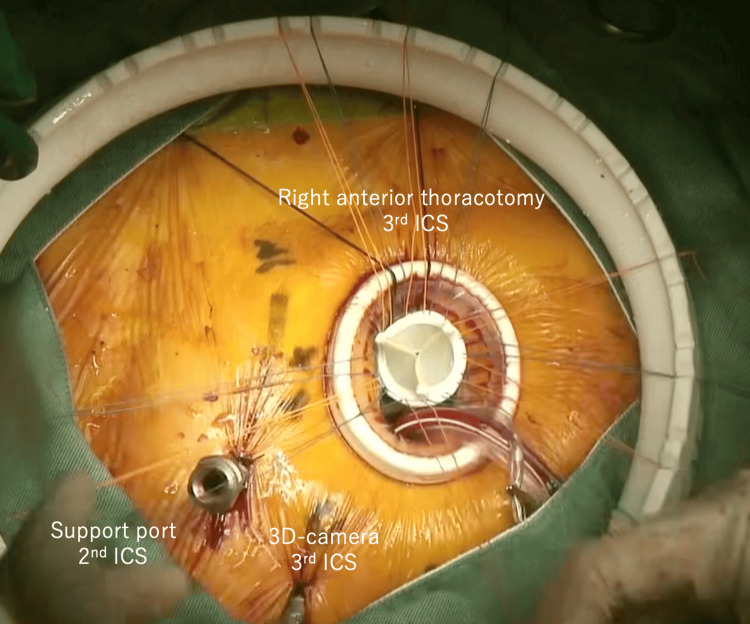 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Coronary Artery Anomalies · Congenital Heart Disease Studies
Introduction
Inferior vena cava (IVC) anomalies, including duplicated IVC and interrupted hepatic IVC, are rare congenital conditions with a prevalence of approximately 0.6% in the general population [1]. These anomalies are often asymptomatic and incidentally found during imaging studies. However, they can pose significant challenges during minimally invasive cardiac surgery (MICS) procedures. The IVC develops between the 4th and 8th weeks of gestation through a complex process involving the postcardinal, subcardinal, and supracardinal veins. Disruptions in this process may result in variations such as duplication or interruption [2,3]. In this report, we present a case of successful MICS-aortic valve replacement (AVR) in a patient with duplicated IVC and interruption at the hepatic segment.
Case presentation
A 72-year-old female patient presented with exertional dyspnea and an abnormal electrocardiogram suggestive of left ventricular hypertrophy during a routine health examination. She had no prior cardiovascular history or known congenital anomalies. Symptoms had persisted for several months. Transthoracic echocardiography revealed severe aortic regurgitation (regurgitant volume: 66 mL) with left ventricular dysfunction (LVDd/Ds, 61/47 mm; EF, 46%). Contrast-enhanced CT revealed a duplicated IVC with an interrupted hepatic segment. Figure 1 shows 3D reconstructed imaging. Axial CT images (Figure 2a) demonstrate duplicated IVC, while Figure 2b, adapted from Li et al. [1], shows a reference image of duplicated IVC.
Three-dimensional CT reconstruction of venous system anomaliesIVC: inferior vena cava3D CT reconstruction of duplicated IVC and hepatic segment interruption. Yellow indicates the left-sided IVC, blue indicates the right-sided IVC, and red indicates the hepatic vein. The arrow highlights the interruption of the hepatic segment, the triangle indicates the left renal vein, through which the left-sided IVC drains into the right-sided system
Axial CT imagesIVC: inferior vena cava(a) Our case shows duplicated inferior vena cava (IVC), with arrows indicating the right- and left-sided IVC, and the triangle indicating the abdominal aorta. (b) Reference image reproduced from Li et al. [1], showing a similar pattern of duplicated IVC
MICS-AVR was performed through a right anterior thoracotomy using a 3D thoracoscopic system. Figure 3 illustrates the surgical setup. Venous cannulation was achieved via the right internal jugular vein (19 Fr) and right femoral vein (17 Fr), with shallow placement of the femoral cannula due to the IVC interruption. Arterial cannulation was via the right femoral artery. Because drainage was insufficient (maximum flow, 2.6 L/min; ideal, 3.3 L/min for BSA 1.37 m²), mild hypothermia (30°C) and vacuum-assisted venous drainage were used to support perfusion. A 23 mm Inspiris Resilia valve (Edwards Lifesciences, Irvine, CA, USA) was implanted. Venous cannulae (Bio-Medicus NextGen, Medtronic, Minneapolis, MN, USA) were used. Left ventricular venting was performed via the left upper pulmonary vein. The postoperative course was uneventful. She was discharged on postoperative day 6. At three-month follow-up, valve function remained stable with no symptom recurrence.
Port placement for MICS-AVR in this caseMICS-AVR: minimally invasive cardiac surgery-aortic valve replacement; ICS: intercostal spaceIntraoperative view showing the typical port configuration used during MICS-AVR: right anterior thoracotomy in the 3rd ICS, support port in the 2nd ICS, and 3D camera port in the 3rd ICS. This setup was not modified despite the vascular anomaly, as venous access was achieved with an adjusted cannulation strategy rather than changes in port placement
Discussion
Li et al. provided a comprehensive review of IVC variants using cross-sectional imaging, which is essential in preoperative planning for MICS [1]. IVC anomalies, although frequently asymptomatic, can present serious technical challenges during venous cannulation. In our case, identification of duplicated IVC with hepatic interruption necessitated a personalized cannulation strategy. Unlike standard AVR procedures, where single femoral venous cannulation is sufficient, we employed a dual-drainage approach. A second cannula was added via the right internal jugular vein, and the femoral cannula was deliberately positioned shallowly below the hepatic interruption.
Previous literature has reported cases of failed cannulation or retroperitoneal hematomas due to unrecognized IVC anomalies [4,5]. In a particularly severe case, fatal hemorrhage occurred during femoral cannulation for venovenous ECMO in a patient with duplicated IVC [6]. Had conventional cannulation been attempted in our case, serious complications might have ensued.
Transesophageal echocardiography (TEE) is critical for verifying cannula positioning. However, anomalous venous pathways can cause guidewires or cannulas to deviate from expected routes, making them difficult to trace. Although fluoroscopy was not required intraoperatively in this case, it remains a valuable modality when visualization is challenging [7].
MICS demands precision in vascular access. While offering advantages in aesthetics and recovery, the presence of IVC anomalies increases procedural complexity and risk [8]. In our case, despite reduced venous return, mild hypothermia allowed safe completion of cardiopulmonary bypass (CPB). Alternative drainage options, such as direct right atrial cannulation or additional cannulation via the left femoral vein, should also be considered.
Conclusions
This case illustrates the importance of recognizing IVC anomalies in MICS. Contrast-enhanced CT enabled detection of duplicated and interrupted IVC, which informed a modified cannulation plan, ensuring procedural safety. Surgeons should remain vigilant for such anomalies and consider preoperative imaging and alternative cannulation routes to minimize risks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The inferior vena cava: anatomical variants and acquired pathologies Insights Imaging Li SJ Lee J Hall J Sutherland TR 1231220213446001510.1186/s 13244-021-01066-7PMC 8405820 · doi ↗ · pubmed ↗
- 2Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings Radiographics Bass JE Redwine MD Kramer LA Huynh PT Harris JH Jr 639652202000 https://pubmed.ncbi.nlm.nih.gov/10835118/1083511810.1148/radiographics.20.3.g 00ma 09639 · doi ↗ · pubmed ↗
- 3Congenital anomalies of the venae cavae: embryological origin, imaging features and report of three new variants Eur Radiol Minniti S Visentini S Procacci C 204020551220021213632310.1007/s 00330-001-1241-x · doi ↗ · pubmed ↗
- 4Incidental finding of interrupted inferior venacava during minimally invasive cardiac surgery Ann Card Anaesth Singh SS Palangadan S Yadav M 234237242021 https://doi.org/10.4103/aca.ACA_170_193388498310.4103/aca.ACA_170_19PMC 8253027 · doi ↗ · pubmed ↗
- 5Interrupted inferior vena cava syndrome discovered incidentally after minimally invasive mitral valve repair in a 31-year-old female patient: a case report Int J Surg Case Rep Abu-Hilal LH Barghouthi DI Abu Keshek T Tamimi H Khatib H Dayeh AH 10862110920233754409510.1016/j.ijscr.2023.108621 PMC 10423890 · doi ↗ · pubmed ↗
- 6Complication of venovenous extracorporeal membrane oxygenation cannulation-the significance of an inferior vena cava anomaly Clin Case Rep Yeung Ng P Wong CC Young K Kwong YY Sin WC 1132113442016 https://doi.org/10.1002/ccr 3.7082798074810.1002/ccr 3.708PMC 5134192 · doi ↗ · pubmed ↗
- 7Cannulation strategies and pitfalls in minimally invasive cardiac surgery Methodist Debakey Cardiovasc J Ramchandani M Al Jabbari O Abu Saleh WK Ramlawi B 1013122016 https://doi.org/10.14797/mdcj-12-1-1010.14797/mdcj-12-1-10PMC 484796027127556 · doi ↗ · pubmed ↗
- 8A case report of an interrupted inferior vena cava and azygos continuation: implications for preoperative screening in minimally invasive cardiac surgery Eur Heart J Case Rep Knol WG Oei FB Budde RP Ter Horst M 052021 https://doi.org/10.1093/ehjcr/ytab 30810.1093/ehjcr/ytab 308PMC 842232834514303 · doi ↗ · pubmed ↗