When the Transition Goes Wrong: A Rare Case of Diabetic Ketoalkalosis After Transitioning to Tirzepatide in Insulin-dependent Type 2 Diabetes
Waleed Sultan, Jeanne Spencer

TL;DR
A rare case of diabetic ketoalkalosis occurred in a patient with type 2 diabetes after switching to tirzepatide, emphasizing the need for careful monitoring during medication transitions.
Contribution
This paper reports a rare case of diabetic ketoalkalosis following a transition to tirzepatide in insulin-dependent type 2 diabetes.
Findings
A 57-year-old patient developed diabetic ketoalkalosis after switching to tirzepatide.
The condition was managed successfully with fluids, electrolytes, and insulin.
The case underscores the importance of gradual insulin tapering and close monitoring during medication transitions.
Abstract
Type 2 diabetes mellitus (T2DM) often requires pharmacological management, with newer agents like glucagon-like peptide-1 (GLP-1) receptor agonists (GLP-1 RA) and dual gastric inhibitory polypeptide (GIP)/GLP-1 receptor agonists offering metabolic and cardiovascular benefits. However, transitioning from insulin therapy to these agents can lead to rare complications, such as diabetic ketoalkalosis, a metabolic disturbance marked by simultaneous ketosis and alkalosis. We report an unusual case of diabetic ketoalkalosis, a mixed acid-base disorder, in a 57-year-old female patient with insulin-dependent T2DM following a switch to Mounjaro (tirzepatide). The patient presented with nausea, vomiting, elevated anion gap, ketosis, and a slightly alkalotic venous pH. This was attributed to insulin deficiency and vomiting-induced acid loss and bicarbonate retention. Management with fluids,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
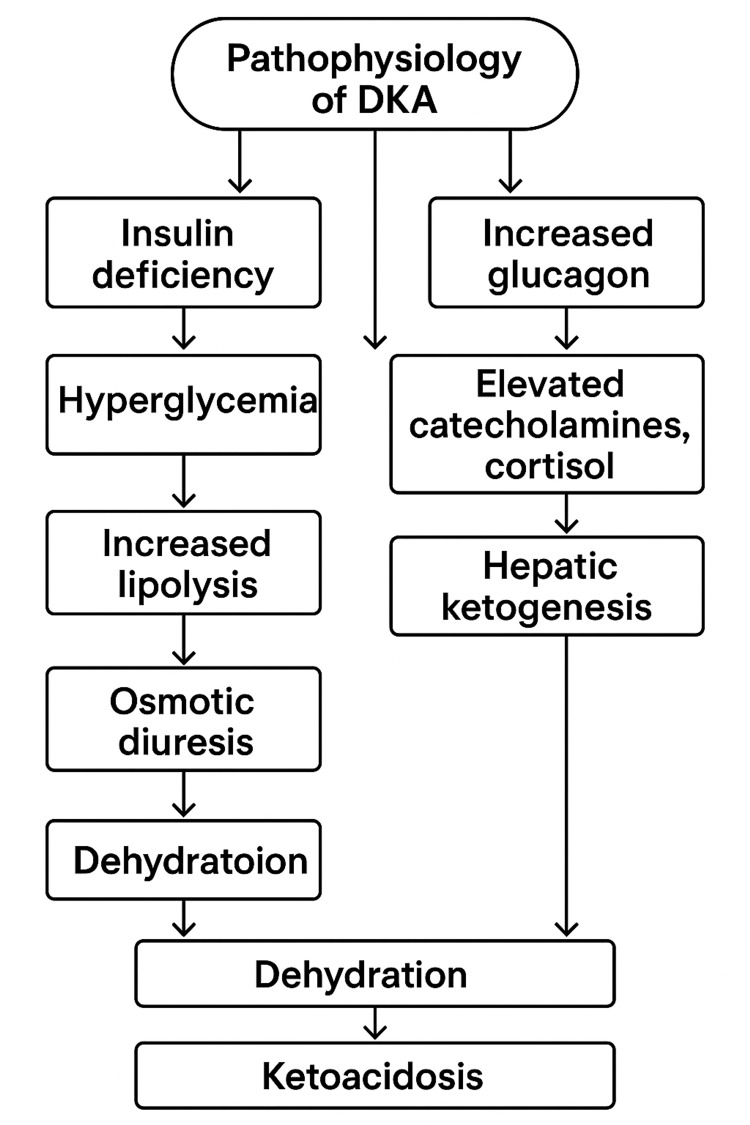 Figure 1
Figure 1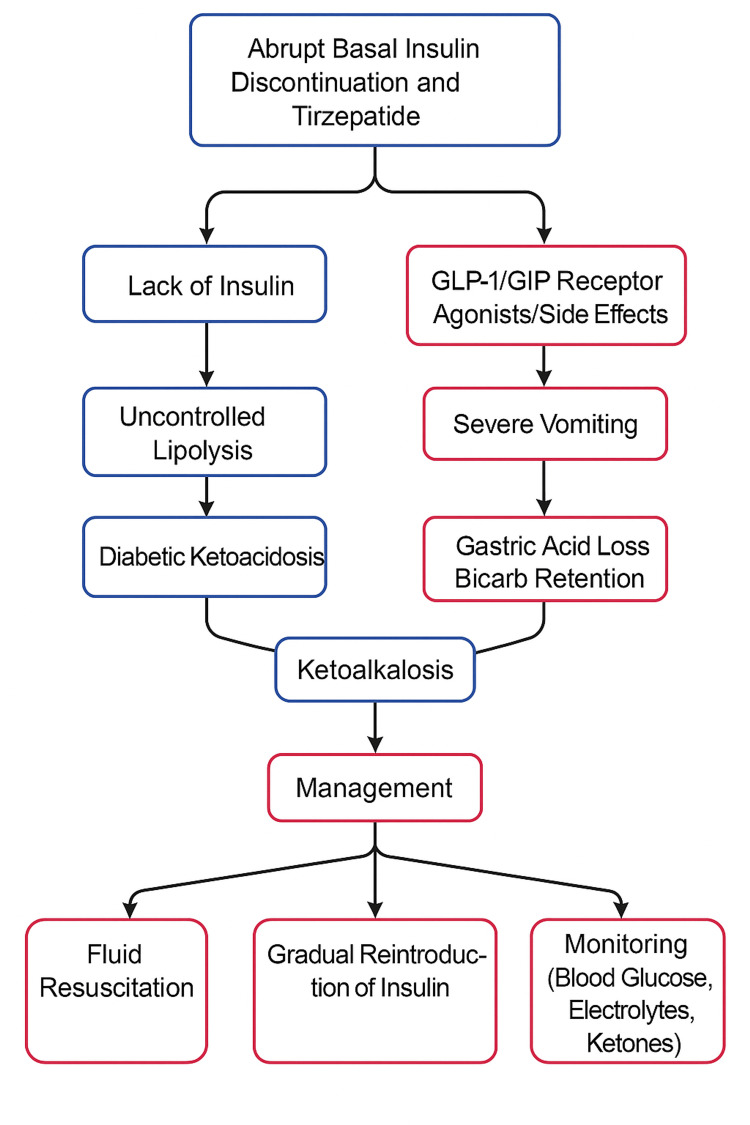 Figure 2
Figure 2| Lab Test | Result | Reference Range | Interpretation |
| Random blood glucose | 320 mg/dL | 70–140 mg/dL | Elevated (Hyperglycemia) |
| Anion gap | 23 mmol/L | 8–16 mmol/L | Elevated (metabolic acidosis) |
| Beta-hydroxybutyrate | 6.7 mmol/L | <0.6 mmol/L | Significantly elevated (ketosis) |
| Lipase | 30 U/L | 12-52 U/L | Normal |
| Serum potassium | 3.2 mmol/L | 3.5–5.0 mmol/L | Low (mild hypokalemia) |
| Serum osmolality | 340 mOsm/kg | 275–295 mOsm/kg | Elevated (hyperosmolar state) |
| Venous pH | 7.45 | 7.32–7.42 | Slightly alkalotic (suggests metabolic alkalosis) |
| Mechanism | GLP-1 Receptor Agonist | GIP Receptor Agonist |
| Primary Target | GLP-1 receptors (β-cells, CNS, stomach, heart) | GIP receptors (β-cells, adipose tissue, CNS) |
| Insulin Secretion | ↑ Glucose-dependent insulin release | ↑ Glucose-dependent insulin release |
| Glucagon Secretion | ↓ Suppressed postprandial glucagon | Context-dependent (↑ during hypoglycemia, ↓ postprandially) |
| Gastric Emptying | ↓ Delayed | Minimal effect |
| Appetite / Satiety | ↑ Satiety, ↓ food intake | Modulates appetite; effect amplified when combined with GLP-1 RA |
| Body Weight | ↓ Weight (via appetite suppression) | Neutral or ↑ when alone; ↓ when combined with GLP-1 RA |
| Adipose Tissue Effects | ↓ Lipogenesis | ↑ Lipid buffering, ↑ insulin sensitivity, ↑ storage capacity |
| β-cell Function | ↑ Proliferation & survival | ↑ Function (less robust alone) |
| Cardiometabolic Effects | ↓ CV events, ↓ inflammation | Under investigation |
| Complication | Cause | Prevention Strategy |
| Hyperglycemia | Rapid insulin reduction or discontinuation | Gradual insulin tapering; frequent blood glucose monitoring |
| Ketosis / Diabetic Ketoacidosis (DKA) | Excessive insulin reduction in insulin-dependent patients | Avoid abrupt basal insulin discontinuation; monitor ketones |
| Gastrointestinal Side Effects | GLP-1-induced delayed gastric emptying | Start at a low dose, then titrate slowly |
| Hypoglycemia | Insulin dose is not reduced appropriately when starting GLP-1/GIP RA | Reduce insulin dose appropriately at initiation; monitor glucose levels |
| Dehydration and Electrolyte Imbalance | Vomiting or reduced food intake | Encourage hydration; monitor electrolytes |
| Weight Loss-Related Muscle Loss | Reduced appetite, rapid weight loss, decreased protein intake | Ensure adequate protein intake; encourage resistance exercise |
| Pancreatitis | GLP-1 receptor activation in susceptible patients | Monitor for severe abdominal pain; discontinue if pancreatitis is suspected. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Diabetes and associated disorders · Diet and metabolism studies
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disease marked by insulin resistance and progressive β-cell dysfunction. Pharmacologic therapy is often required to maintain glycemic control, with insulin traditionally serving as a cornerstone in patients with significant hyperglycemia or β-cell failure [1]. In recent years, incretin-based therapies, including glucagon-like peptide-1 receptor agonists (GLP-1 RA) and dual glucose-dependent insulinotropic polypeptide/glucagon-like peptide-1 receptor agonists (GIP/GLP-1 RA), have gained traction due to their benefits on weight loss, cardiovascular risk, and renal protection [2-4].
Despite these advantages, transitioning insulin-dependent patients to these newer agents may pose metabolic risks. One rare but increasingly recognized complication is diabetic ketoalkalosis, a mixed acid-base disorder characterized by concurrent ketoacidosis and metabolic alkalosis [5,6]. This case report presents a patient with T2DM who developed diabetic ketoalkalosis following abrupt discontinuation of basal insulin during the initiation of tirzepatide (Mounjaro), emphasizing the need for gradual insulin tapering and close monitoring while transitioning from insulin to GIP/GLP-1 RA in high-risk individuals.
Case presentation
A 57-year-old female patient with a history of insulin-dependent type 2 diabetes mellitus presented to the emergency department with intractable nausea and vomiting. She reported that these symptoms had been ongoing but had significantly worsened over the preceding several weeks. This exacerbation followed a recent change in her diabetes regimen; She had been transitioned from a combination of long-acting insulin (40 units nightly) and short-acting insulin (10 units before meals) to tirzepatide (Mounjaro), a dual GLP-1/GIP receptor agonist, approximately seven weeks prior to presentation. The transition was made due to persistently uncontrolled blood glucose levels, with a recent hemoglobin A1c of 12%. The patient completely discontinued the insulin once she started the tirzepatide and hasn't been to a follow-up visit, with poor home glucose monitoring since the transition.
On physical examination, the patient appeared dehydrated, exhibited deep and rapid respirations (Kussmaul breathing), and had a fruity odor on her breath. Initial laboratory evaluation revealed significant metabolic derangements, including findings consistent with both ketoacidosis and metabolic alkalosis, as detailed in Table 1.
The elevated anion gap and markedly raised beta-hydroxybutyrate were consistent with diabetic ketosis with coexisting metabolic alkalosis (mixed metabolic state). Metabolic alkalosis was likely secondary to prolonged vomiting, which masked the typical acidosis seen in diabetic ketoacidosis (DKA).
The patient was managed with a two-liter IV normal saline bolus; she was restarted on her long-acting insulin at a reduced dose of 25 units and a low-dose sliding scale. The patient responded well to this conservative approach and demonstrated rapid clinical improvement and normalization of anion gap and venous pH within 18 hours.
To further evaluate the underlying etiology and rule out type 1 diabetes, her C-peptide level was consistent with type 2 diabetes. Since the patient's condition stabilized quickly and she remained clinically well, she was discharged home on her prior long-acting insulin and sliding scale insulin three times daily, with plans for close outpatient follow-up and monitoring.
Discussion
DKA is a potentially life-threatening condition that primarily affects individuals with type 1 diabetes but can also occur in type 2 diabetes. It results from severe insulin deficiency and increased levels of counter-regulatory hormones, leading to hyperglycemia, ketosis, and metabolic acidosis (Figure 1) [1].
Pathophysiology of DKA.DKA: Diabetic ketoacidosisImage credit: Author-created.
Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptor agonists (RAs) are a class of drugs used in type 2 diabetes management. They mimic the effects of incretin hormones (GLP-1 and GIP), which are naturally released from the gut in response to food intake, enhancing glucose regulation [2,3]. The mechanism of action is summarized in Table 2.
Switching from insulin to GLP-1/GIP receptor agonists (e.g., tirzepatide) may benefit patients with type 2 diabetes, especially those needing weight loss, better glycemic control, or reduced hypoglycemia. The transition should be gradual and individualized. It is suitable for patients on basal insulin with poor control or frequent hypoglycemia, but is not recommended for those with type 1 diabetes or severe insulin deficiency [3]. The SURPASS-5 (Study of Tirzepatide in Participants With Type 2 Diabetes on Insulin Glargine) trial demonstrated that switching to tirzepatide from insulin therapy significantly reduced insulin requirements [7]. Based on these findings, it is recommended to gradually reduce insulin doses when initiating tirzepatide to prevent hypoglycemia and optimize glycemic control [7]. For patients with an HbA1c of 8% or less, a 20% reduction in insulin dose upon starting tirzepatide may be appropriate. While exact dose adjustments should be individualized, monitoring blood glucose levels and making gradual insulin titration is essential for achieving the best outcomes [3,7].
While transitioning from insulin to GLP-1/GIP receptor agonists (e.g., tirzepatide, semaglutide, dulaglutide) offers benefits such as improved glycemic control, weight loss, and reduced hypoglycemia risk, some complications can arise during the switch, as shown in Table 3.
Diabetic ketoalkalosis (DKA-Alk) is a rare condition where metabolic alkalosis coexists with DKA, creating a mixed acid-base disturbance. While DKA is driven by anion gap metabolic acidosis due to ketone buildup from insulin deficiency, vomiting can cause gastric acid loss, leading to bicarbonate retention and hypochloremic alkalosis. Other contributors include osmotic diuresis, respiratory compensation, and excessive bicarbonate use. Patients may show symptoms of both conditions, such as polyuria, nausea, Kussmaul breathing, and confusion. Treatment includes fluid resuscitation, electrolyte replacement, and cautious insulin therapy; bicarbonate is reserved for pH<6.9 [5,6].
In our case, abrupt basal insulin discontinuation during the transition to GLP-1/GIP receptor agonists triggered DKA-Alk. Insulin deficiency led to ketosis, while vomiting caused alkalosis. The patient improved with fluids, insulin, and electrolyte monitoring. The pathophysiology and management are illustrated in Figure 2.
Pathophysiology of mixed metabolic state, diabetic ketolakalosis, and proper management.Image credit: Author-created.
Conclusions
Diabetic ketoalkalosis is a rare but serious complication that can occur during transitions from insulin to GLP-1/GIP receptor agonists. In this case, the abrupt discontinuation of insulin and GLP-1/GIP RA-induced vomiting triggered a mixed acid-base disorder. The patient improved with careful management, including fluid resuscitation, insulin reintroduction, and electrolyte monitoring. This case underscores the importance of gradual insulin tapering and close monitoring to prevent metabolic complications during such transitions. Given the limited literature on diabetic ketoalkalosis during incretin-based transitions, further studies and reports are needed to better understand its incidence, pathophysiology, and optimal management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12. Diagnosis and classification of diabetes: Standards of Care in Diabetes - 2024 Diabetes Care American Diabetes Association Professional Practice Committee 042472024
- 2GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art Mol Metab Nauck MA Quast DR Wefers J Meier JJ 1011024620213306877610.1016/j.molmet.2020.101102 PMC 8085572 · doi ↗ · pubmed ↗
- 3Efficacy and safety of tirzepatide in adults with type 2 diabetes: a perspective for primary care providers Clin Diabetes Kushner P Anderson JE Simon J Boye KS Ranta K Torcello-Gómez A Levine JA 2582724120233709214410.2337/cd 22-0029 PMC 10115620 · doi ↗ · pubmed ↗
- 4The American Diabetes Association releases the Standards of Care in Diabetes - 2024 Diabetes Care American Diabetes Association 2024 https://diabetes.org/newsroom/press-releases/american-diabetes-association-releases-standards-care-diabetes-2024
- 5Euglycemic ketoacidosis Curr Diab Rep Bonora BM Avogaro A Fadini GP 252020203242473010.1007/s 11892-020-01307-x · doi ↗ · pubmed ↗
- 6Diabetic ketoalkalosis: the dark, torrid horse of diabetic emergencies Explor Med Ashinze P Mafua N Banerjee S 54455252024 https://www.explorationpub.com/Journals/em/Article/1001238
- 7Insulin requirements after switching from GLP-1 receptor agonist to dual GIP/GLP-1 receptor agonist in patients with type 2 diabetes mellitus Pharmacotherapy Lahey AM Duprey K Montague RC Schadler AD Naseman KW 2202264520254010885410.1002/phar.70009 · doi ↗ · pubmed ↗