Left Ventricular Noncompaction Cardiomyopathy in an Elderly Patient: A Case Report
Reza Alavi, Hector Armando Sanchez Garcia, Mohamad Ahmad, Rami Akel

TL;DR
An elderly woman was diagnosed with a rare heart condition called left ventricular noncompaction cardiomyopathy, which was previously undetected despite her age and symptoms.
Contribution
Highlights the underrecognition of left ventricular noncompaction cardiomyopathy in elderly patients and emphasizes the need for advanced imaging for diagnosis.
Findings
LVNC was diagnosed in an 85-year-old woman with heart failure and atrial fibrillation.
ECG showed T-wave inversions and echocardiography revealed a noncompacted-to-compacted ratio >2:1.
The case suggests LVNC can remain undiagnosed until later in life despite being congenital.
Abstract
Left ventricular noncompaction is a rare cardiomyopathy, often underrecognized in older adults, characterized by prominent myocardial trabeculations and deep intertrabecular recesses. These structural abnormalities can lead to heart failure, arrhythmias, and thromboembolic events. We report the case of an 85-year-old woman with a history of heart failure with preserved ejection fraction and atrial fibrillation who presented with chest pain and dyspnea. Her electrocardiogram (ECG) revealed new diffuse T-wave inversions. Coronary angiography showed no obstructive disease. Transthoracic echocardiography demonstrated features consistent with left ventricular noncompaction cardiomyopathy (LVNC), including a noncompacted-to-compacted ratio greater than 2:1, along with a reduced left ventricular ejection fraction (LVEF) of 25-30% (normal LVEF >55%). Cardiac MRI was recommended to further…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
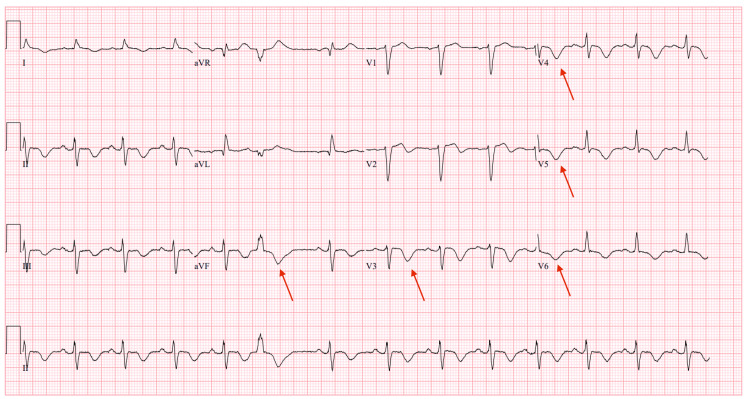 Figure 1
Figure 1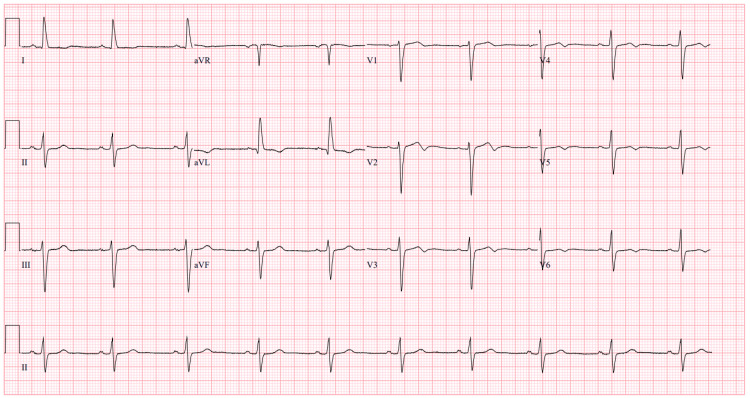 Figure 2
Figure 2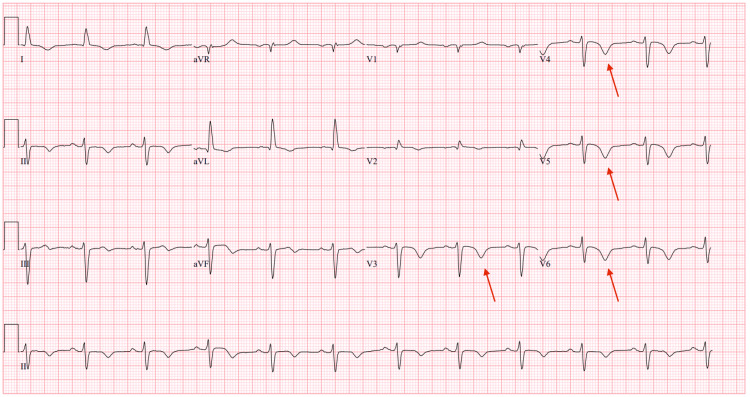 Figure 3
Figure 3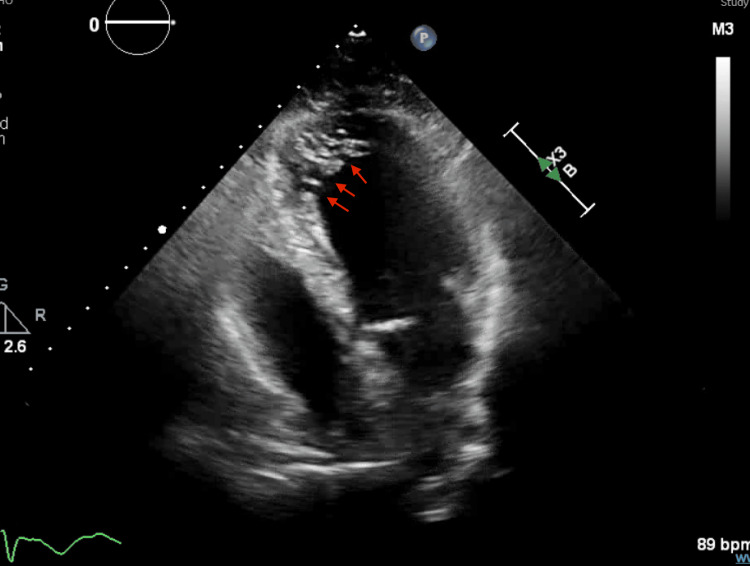 Figure 4
Figure 4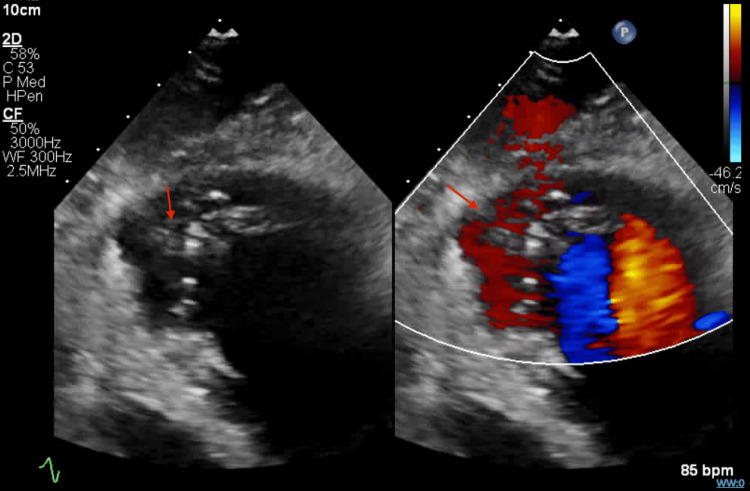 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Neurogenetic and Muscular Disorders Research · Williams Syndrome Research
Introduction
Left ventricular noncompaction cardiomyopathy (LVNC) is a rare and underrecognized form of cardiomyopathy resulting from incomplete myocardial compaction during embryogenesis. It is characterized by excessive trabeculations and deep intertrabecular recesses, which can lead to heart failure, arrhythmias, and thromboembolic events. The reported prevalence ranges from 0.01% to 0.3% in the general population, with recognition in elderly patients remaining uncommon, potentially due to underdiagnosis rather than true absence [1-3]. Early recognition is essential to prevent complications and guide therapy. Diagnosis is typically made using echocardiography, which includes criteria such as a two-layered myocardium with a noncompacted-to-compacted ratio greater than 2:1 in end-systole, multiple prominent trabeculations, and color Doppler evidence of deep recesses within the ventricular cavity [1-3]. Cardiac MRI can provide additional diagnostic confirmation, using Petersen’s criterion (noncompacted-to-compacted ratio >2.3 in diastole) or Jacquier’s criterion (>20% of trabeculated mass relative to global LV mass) [4-5]. Differentiating LVNC from mimickers, such as hypertrophic cardiomyopathy, apical thrombus, or normal prominent trabeculations, is crucial to avoid misdiagnosis. The clinical spectrum ranges from asymptomatic individuals to patients with severe systolic dysfunction or life-threatening arrhythmias. Genetic testing and family screening are advised, given associations with autosomal dominant, X-linked, and mitochondrial inheritance patterns [4-5]. Management strategies for LVNC are similar to those for other forms of heart failure, with the addition of anticoagulation therapy at a lower threshold due to the increased risk of thromboembolic events [6].
Case presentation
An 85-year-old Caucasian woman with a history of heart failure with preserved ejection fraction (HFpEF), paroxysmal atrial fibrillation, hypertension, and type 2 diabetes mellitus presented to Bayonet Point Hospital with acute-onset substernal chest pain and exertional dyspnea. Her symptoms improved with sublingual nitroglycerin. On admission (hospital day 1), her high-sensitivity troponin was markedly elevated at 1393 ng/mL (normal <0.04 ng/mL). Differential diagnosis for this elevation included type 2 myocardial infarction due to supply-demand mismatch or myocarditis, particularly given the absence of obstructive coronary artery disease.
An ECG on admission showed sinus rhythm with diffuse T-wave inversions (Figure 1), whereas her baseline outpatient ECG showed normal sinus rhythm without T-wave abnormalities (Figure 2). Repeat ECGs during hospitalization revealed progressive T-wave inversions, with partial resolution noted prior to discharge (Figure 3). This change could reflect resolving myocardial strain, treatment response, or nonspecific repolarization abnormalities of uncertain significance.
Admission ECG showing sinus rhythm with diffuse T-wave inversionsThe red arrows highlight these T-wave inversions.
Baseline ECG prior to admission showed a normal sinus rhythm
ECG before discharge showing partial resolution of T-wave changesThe arrows show fewer T-wave inversions compared to the ECG shown in Figure 1.
Emergent coronary angiography (hospital day 1) revealed non-obstructive coronary arteries. Transthoracic echocardiography performed on hospital day 2 demonstrated a reduced left ventricular ejection fraction of 25-30% (normal >55%) and prominent trabeculations in the apical and mid-ventricular segments. Still frames captured at end-systole and end-diastole showed a noncompacted-to-compacted myocardial ratio >2:1 (Figure 4), meeting echocardiographic criteria for LVNC. Color Doppler imaging demonstrated flow within deep intertrabecular recesses (Figure 5), further supporting the diagnosis.
Echocardiographic image at end-systole demonstrating prominent trabeculations with a noncompacted-to-compacted myocardial ratio >2:1The red arrows indicate some of the excessive trabeculations within the left ventricle. The noncompacted-to-compacted ratio was measured in end-systole using the Jenni criteria, confirming the diagnosis of left ventricular noncompaction.
Color Doppler imaging in systole shows flow through intertrabecular recessesThe red arrows show some of the trabeculations in the left ventricle.
Cardiac MRI was offered to confirm the extent of noncompaction and assess for fibrosis, but the patient declined due to age and comorbidities, limiting definitive tissue characterization and volumetric assessment. Genetic testing and family screening were considered, given the congenital nature of LVNC and its autosomal dominant, X-linked, or mitochondrial inheritance patterns, but were deferred pending outpatient cardiology evaluation.
She was started on guideline-directed medical therapy, including metoprolol succinate, sacubitril-valsartan, dapagliflozin, and apixaban. She was discharged with a wearable cardioverter defibrillator and scheduled for outpatient cardiology follow-up to evaluate for implantable cardioverter-defibrillator placement.
Discussion
This case underscores the importance of considering LVNC as a cause of new-onset systolic heart failure, particularly in elderly patients with overlapping comorbidities. LVNC can clinically or structurally mimic HFpEF or ischemic cardiomyopathy in older adults due to shared features such as diastolic dysfunction, reduced compliance, and symptoms of congestion despite preserved or mildly reduced ejection fraction [3,5]. Diagnostic pitfalls include attributing symptoms solely to hypertensive heart disease, atrial fibrillation, or coronary artery disease without evaluating for underlying structural cardiomyopathies [3].
The diagnosis of LVNC in this patient was notable for several reasons, including the atypical age of onset, the delay in diagnosis, the successful noninvasive diagnosis, and the presence of electrocardiographic abnormalities that served as early diagnostic clues. Although LVNC is more often recognized in pediatric populations, cases in older adults, while rare, have been reported, suggesting under-recognition rather than true absence [5,7].
One notable ECG finding in our patient was T-wave inversions in the inferolateral leads. These repolarization changes have been described in LVNC and may reflect subendocardial ischemia or architectural repolarization abnormalities due to excessive trabeculations. However, T-wave inversions are neither specific nor sensitive for LVNC and can be incidental or related to comorbid ischemic heart disease, limiting their diagnostic utility without supporting imaging [8-11].
The prognostic implications of LVNC in elderly patients remain uncertain, as most data derive from younger cohorts; however, potential risks include arrhythmias, thromboembolic events, and progressive heart failure, necessitating individualized risk stratification [3,5,6]. While device therapy, such as ICD implantation, is considered in LVNC patients with reduced ejection fraction, its utility in older adults requires assessment of the overall goals of care [3,5].
Genetic evaluation and family screening are standard in LVNC due to its hereditary nature, but in this case, testing was not pursued given the patient’s advanced age, absence of family history, and limited implications for her immediate management [4,5].
As highlighted in the literature, LVNC is often misdiagnosed or underrecognized in older adults, largely due to overlapping cardiac comorbidities and nonspecific presentations [3]. This case raises questions about the true prevalence of LVNC in the aging population and underscores the need for greater clinical vigilance to ensure appropriate diagnosis and management [3,5].
Conclusions
This case illustrates the diagnostic challenges of LVNC in the elderly, particularly in patients with overlapping cardiovascular comorbidities. It underscores the importance of revisiting prior diagnoses and imaging when new cardiac dysfunction emerges. While echocardiography can often establish the diagnosis, advanced imaging modalities such as cardiac MRI may be essential in selected or equivocal cases to confirm the diagnosis and assess the extent of noncompaction. Early identification can significantly influence clinical management, as in this patient, where the diagnosis prompted guideline-directed medical therapy for heart failure and consideration of anticoagulation given the risk of thromboembolism. Although implantable defibrillator placement was not pursued due to the patient’s advanced age and goals of care, she was discharged with a wearable cardioverter-defibrillator for interim protection, as device therapy is often indicated in LVNC patients with reduced ejection fraction. Genetic evaluation and family screening were discussed but ultimately not pursued given her age and lack of immediate implications for her management. Future research should focus on defining the epidemiology of LVNC in older adults, validating diagnostic criteria in this population, and evaluating treatment outcomes to guide optimal care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Left ventricular non-compaction: from recognition to treatment Curr Pharm Des Ganame J 4844902120152548395010.2174/138161282104141204143212 · doi ↗ · pubmed ↗
- 2A rare case of left ventricular non-compaction with coronary artery anomaly complicated by ST-elevation myocardial infarction and subcutaneous defibrillator implantation Int J Environ Res Public Health Prandi FR Illuminato F Galluccio C 119202210.3390/ijerph 19020791 PMC 877542435055613 · doi ↗ · pubmed ↗
- 3Left ventricular non-compaction cardiomyopathy Lancet Towbin JA Lorts A Jefferies JL 81382538620152586586510.1016/S 0140-6736(14)61282-4 · doi ↗ · pubmed ↗
- 4European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus statement on the state of genetic testing for cardiac diseases Heart Rhythm Wilde AA Semsarian C Márquez MF 019202210.1016/j.hrthm.2022.03.122535390533 · doi ↗ · pubmed ↗
- 5Ventricular non-compaction review Heart Fail Rev Srivastava S Yavari M Al-Abcha A Banga S Abela G 106310762720223423243810.1007/s 10741-021-10128-3 · doi ↗ · pubmed ↗
- 6The pivotal role of cardiovascular imaging in the identification and risk stratification of non-compaction cardiomyopathy patients Heart Fail Rev Mavrogeni SI Markousis-Mavrogenis G Vartela V 100710152520203178485910.1007/s 10741-019-09898-8 · doi ↗ · pubmed ↗
- 7Isolated noncompaction of the left ventricular myocardium—a review of the literature two decades after the initial case description Clin Res Cardiol Engberding R Yelbuz TM Breithardt G 4814889620071753456810.1007/s 00392-007-0528-6 · doi ↗ · pubmed ↗
- 8Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy Heart Jenni R Oechslin E Schneider J Attenhofer Jost C Kaufmann PA 6666718620011171146410.1136/heart.86.6.666PMC 1730012 · doi ↗ · pubmed ↗