False-Positive Detection of Haemophilus influenzae by a Multiplex PCR Panel in a Neonate With Late-Onset Group B Streptococcal Bacteremia
Koji Yokoyama, Ayako Okamoto, Misako Ohkusu, Naruhiko Ishiwada

TL;DR
A neonate with Group B Streptococcal bacteremia was falsely diagnosed with Haemophilus influenzae using a multiplex PCR panel, highlighting the need for confirmatory testing and improved diagnostic clarity.
Contribution
This case highlights a diagnostic limitation of multiplex PCR panels and advocates for better algorithmic transparency and validation.
Findings
A neonate's CSF tested falsely positive for Haemophilus influenzae using the FilmArray ME panel.
Confirmatory PCR and culture testing showed no evidence of H. influenzae or meningitis.
The false positive was due to borderline amplification of one H. influenzae target interpreted as positive.
Abstract
Here, we report the case of a term neonate with late-onset Group B Streptococcal (GBS) bacteremia in whom the FilmArray® Meningitis/Encephalitis (ME) panel (BioFire Diagnostics, Salt Lake City, UT, US) falsely detected Haemophilus influenzae in the cerebrospinal fluid (CSF). Although the CSF showed mild pleocytosis and elevated protein, there were no clinical signs of bacterial meningitis. Confirmatory testing, including multiplex PCR targeting H. influenzae (siaT), GBS (cfb), and 16S rRNA, as well as CSF culture, yielded negative results. Repeat FilmArray testing under controlled conditions was also negative. A manufacturer's investigation revealed borderline amplification of only one of the H. influenzae targets, which was interpreted algorithmically as positive. This discordance highlights a key limitation of multiplex PCR panels: the lack of transparency in signal interpretation and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
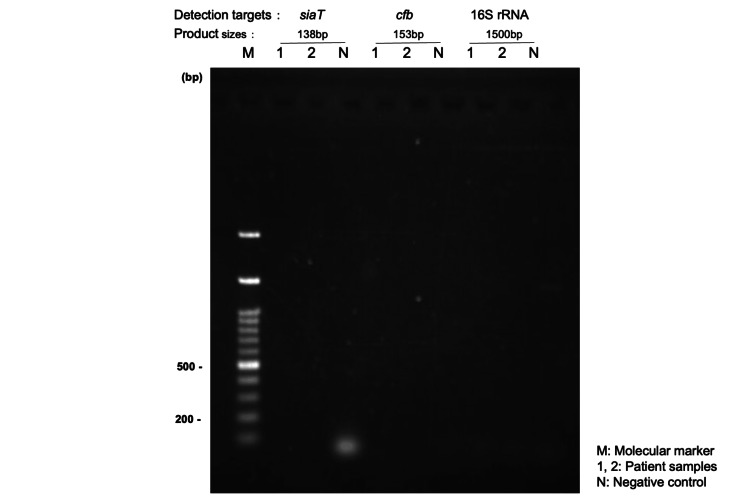 Figure 1
Figure 1| Day of life | Clinical event | Diagnostic or therapeutic action |
| 0 | Term birth | GBS-positive mother, intrapartum antibiotics administered |
| 19 | Fever, poor feeding | Hospital admission, empirical ABPC started |
| 20 | Suspected severe infection | Initial FilmArray ME panel detected GBS (blood) and |
| 22-28 | Clinical improvement | Monotherapy with ABPC continued |
| 29 | Discharge | Stable, afebrile, feeding well |
| Test method | Sample | Target organism(s) | Result | Notes |
| FilmArray ME panel | CSF | H. influenzae | Positive | Only Hinf1 target showed delayed amplification; Hinf2 negative |
| CSF culture (initial) | CSF | – | Negative | Sample contaminated with blood |
| PCR (Chiba Univ, manual) | CSF | siaT, cfb, 16S rRNA | Negative | All targets negative; confirmatory testing performed |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Bacterial Infections and Vaccines · Pneumonia and Respiratory Infections
Introduction
The FilmArray® Meningitis/Encephalitis (ME) panel (BioFire Diagnostics, Salt Lake City, UT, US) enables rapid multiplex PCR-based detection of 14 pathogens directly from the cerebrospinal fluid (CSF) and is widely used for diagnosing meningitis and encephalitis. Its analytical performance, including turnaround time and target coverage, has been evaluated in multicenter validation studies [1]. Furthermore, a systematic review and meta-analysis confirmed that the assay has high pooled sensitivity and specificity across diverse clinical settings [2]. Multiplex PCR simultaneously detects multiple pathogens in a single reaction, enabling rapid diagnosis; however, false positives can lead to unnecessary treatments, which may pose particular risks in neonates. Despite these strengths, false-positive results, particularly for Haemophilus influenzae, remain a critical concern. Here, we present a neonatal case with a false-positive H. influenzae result and discuss the clinical and laboratory implications.
Case presentation
A male term neonate, born at 39 weeks 2 days via vaginal delivery, received ampicillin at the onset of labor due to maternal carriage of Group B Streptococcus (GBS). At 21 days of life, the patient developed fever and lethargy, prompting evaluation for late-onset sepsis. He was an only child with no recent exposure to other young children. A blood culture was positive for GBS. Although maternal colonization was identified at 36 weeks of gestation, a throat swab obtained from the neonate at birth was negative. Initial CSF analysis revealed mildly elevated cell counts (total 103/μL; 53 mononuclear, 50 polymorphonuclear), likely due to traumatic lumbar puncture, with visible blood contamination. CSF protein was elevated (142 mg/dL), while glucose was within the normal range (51 mg/dL; concurrent blood glucose 90 mg/dL). These findings are inconsistent with typical bacterial meningitis; however, the FilmArray ME panel returned a positive result for H. influenzae. Because of the lack of definitive signs of meningitis and discordance with the panel result, the CSF specimen was reanalyzed at an independent facility. Multiplex PCR targeting H. influenzae (siaT), GBS (cfb), and 16S rRNA failed to detect bacterial DNA, and the CSF culture was negative. The same CSF specimen was retested with the FilmArray ME panel under controlled conditions at an independent facility. To minimize contamination risk, the sample was handled in a class II biosafety cabinet using sterile, single-use consumables, and all procedures were performed by trained personnel following the manufacturer’s protocols. The timeline of the clinical events and diagnostics is presented in Table 1.
No amplification of any targets was observed on gel electrophoresis (Figure 1).
Gel electrophoresis results for the PCR targeting specific bacterial genesDNA extracted from the cerebrospinal fluid (CSF) was amplified with primers specific for Haemophilus influenzae (siaT), Group B Streptococcus (GBS, cfb), and universal 16S rRNA. Expected product sizes: siaT, 138 bp; cfb, 153 bp; 16S rRNA, ~1.5 kbp. No amplification was observed.Lane M, marker; Lane 1, neat (undiluted) CSF; Lane 2, 1:2 diluted CSF; Lane N, negative control.
The manufacturer concluded that the initial detection of H. influenzae likely resulted from low-level environmental contamination during sample handling. Immunological evaluations, including immunoglobulin and complement levels, were within normal limits. The patient had no signs of immunodeficiency during the 10 months of follow-up.
The parents of the patient provided informed consent for the publication of this case, and the study was approved by the Institutional Review Board of the Japanese Red Cross Wakayama Medical Center (Approval No. 1481).
Discussion
We describe a false-positive H. influenzae result on the FilmArray ME panel without supporting clinical or laboratory evidence. A summary of the CSF test results is provided in Table 2.
Although the overall false-positive rate for H. influenzae on this panel is <0.1% [3], a previous study reported that 77.8% (14/18) of H. influenzae-positive cases were not confirmed by qPCR or culture [4]. Other retrospective studies also question the alignment of FilmArray results with discharge diagnoses in low-prevalence settings [5]. Environmental contamination during specimen handling may contribute to false-positive results in highly sensitive assays [6,7]. Despite standard decontamination protocols, such occurrences persist in clinical practice, particularly when handling highly sensitive molecular assays in open systems. Current diagnostic platforms often lack integrated contamination safeguards and transparent signal interpretation tools, which may contribute to rare but consequential false-positive results. In this case, the manufacturer found borderline amplification of only one target (Hinf1), while the confirmatory target (Hinf2) was negative. Nonetheless, the system algorithm reported a positive result, consistent with previously noted limitations in qPCR transparency and cycle threshold (Ct) data interpretation [8,9]. Immunodeficiency was unlikely given the patient's normal immunologic profile and uneventful course. Clinicians should remain cautious when test results conflict with the clinical picture, particularly in neonates for whom overtreatment poses additional risks [10]. Future diagnostic platforms should offer sealed cartridges, automated preprocessing, and visible assay-level confidence metrics to reduce unnecessary interventions [11,12]. Emerging methods, including metagenomic sequencing and microbial cell-free DNA testing, may complement standard diagnostics when dealing with complex central nervous system infections [13]. This case underscores the importance of inter-laboratory validation and careful interpretation when laboratory findings are inconsistent with clinical presentation. Given the clinical implications of false-positive syndromic panel results, systematic reporting and data sharing of such cases across institutions may help refine diagnostic criteria and guide future algorithm development.
Conclusions
We report a case in which the FilmArray ME panel falsely detected H. influenzae in the CSF of a neonate with confirmed GBS bacteremia. The false-positive result was overturned by independent molecular and culture-based testing. This case highlights the importance of confirmatory testing and critical clinical judgment when interpreting syndromic panel results, particularly in neonates for whom overdiagnosis may lead to unnecessary interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Multicenter evaluation of Bio Fire Film Array meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens J Clin Microbiol Leber AL Everhart K Balada-Llasat JM 225122615420162733514910.1128/JCM.00730-16PMC 5005480 · doi ↗ · pubmed ↗
- 2Diagnostic test accuracy of the Bio Fire® Film Array® meningitis/encephalitis panel: a systematic review and meta-analysis Clin Microbiol Infect Tansarli GS Chapin KC 2812902620203176011510.1016/j.cmi.2019.11.016 · doi ↗ · pubmed ↗
- 3Evaluation of a commercial multiplex molecular panel for diagnosis of infectious meningitis and encephalitis J Clin Microbiol Liesman RM Strasburg AP Heitman AK Theel ES Patel R Binnicker MJ 56201810.1128/JCM.01927-17PMC 586984329436421 · doi ↗ · pubmed ↗
- 4Unexpectedly high false-positive rates for Haemophilus influenzae using a meningoencephalitis syndromic PCR panel in two tertiary centers Front Cell Infect Microbiol Zanella MC Cherkaoui A Hinic V Renzi G Goldenberger D Egli A Schrenzel J 6396581120213376338810.3389/fcimb.2021.639658 PMC 7982903 · doi ↗ · pubmed ↗
- 5A retrospective observational study of 1000 consecutive patients tested with the Film Array® Meningitis/Encephalitis panel: clinical diagnosis at discharge and microbiological findings Sci Rep Sunnerhagen T Widén J Handhal S Özkaya Şahin G 40151420243836955210.1038/s 41598-024-54621-9PMC 10874959 · doi ↗ · pubmed ↗
- 6Point-counterpoint: meningitis/encephalitis syndromic testing in the clinical laboratory J Clin Microbiol Bard JD Alby K 56201810.1128/JCM.00018-18PMC 586982729343540 · doi ↗ · pubmed ↗
- 7Implementation of the Film Array ME panel in laboratory routine using a simple sample selection strategy for diagnosis of meningitis and encephalitis BMC Infect Dis Pfefferle S Christner M Aepfelbacher M Lütgehetmann M Rohde H 1702020203208768110.1186/s 12879-020-4904-4PMC 7036261 · doi ↗ · pubmed ↗
- 8Systematic review on the association between respiratory virus real-time PCR cycle threshold values and clinical presentation or outcomes J Antimicrob Chemother Bouzid D Vila J Hansen G Manissero D Pareja J Rao SN Visseaux B 04976202110.1093/jac/dkab 246PMC 846010334555159 · doi ↗ · pubmed ↗