Diagnostic Value of Exercise Stress Testing Combined With Beta-Blocker Therapy (Metoprolol) in Hypertensive Patients With Suspected Coronary Artery Disease
Humayun Nasir, Awais Ahmad Nizami, Mamoon Qadir, Maria Shahzad, Hamid Iqbal, Waqar Mustafa, Hifza Ishtiaq, M Mohsin

TL;DR
This study shows that combining exercise stress testing with metoprolol improves diagnostic accuracy for coronary artery disease in hypertensive patients.
Contribution
The study evaluates the diagnostic value of metoprolol-enhanced exercise stress testing in hypertensive patients with suspected CAD.
Findings
The combination of EST and metoprolol showed 72.34% sensitivity and 86.15% specificity for diagnosing CAD.
The overall diagnostic accuracy of the method was 80.36%.
The positive predictive value was 79.07%, indicating strong reliability for positive test results.
Abstract
Background: Hypertension is a prevalent risk factor for coronary artery disease (CAD), and early diagnosis is critical for preventing adverse cardiovascular events. While exercise stress testing (EST) is a common non-invasive tool, its diagnostic performance in hypertensive individuals, especially when combined with beta-blocker therapy, remains under-evaluated. The beta-blocker metoprolol may enhance diagnostic accuracy in this population. Objective: This study aimed to evaluate the diagnostic value of EST combined with metoprolol therapy in hypertensive patients with suspected CAD. Methodology: This prospective, hospital-based controlled diagnostic study was conducted at the Department of Cardiology, Abbas Institute of Medical Science (AIMS), Muzaffarabad, Azad Jammu and Kashmir (AJK), from January 2023 to December 2024. A total of 224 hypertensive patients aged between 30 and 70…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
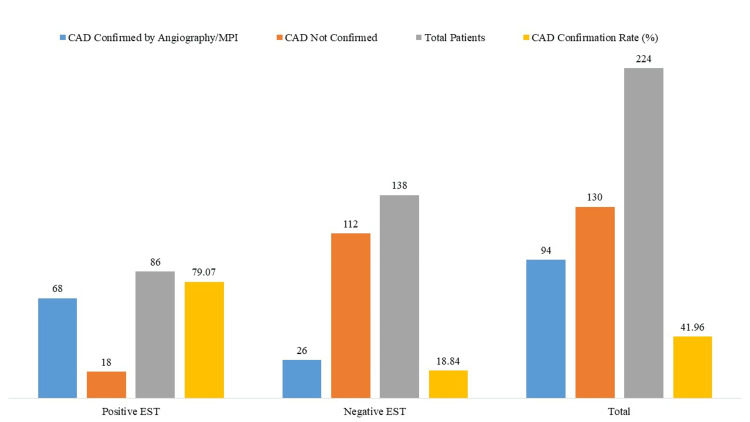 Figure 1
Figure 1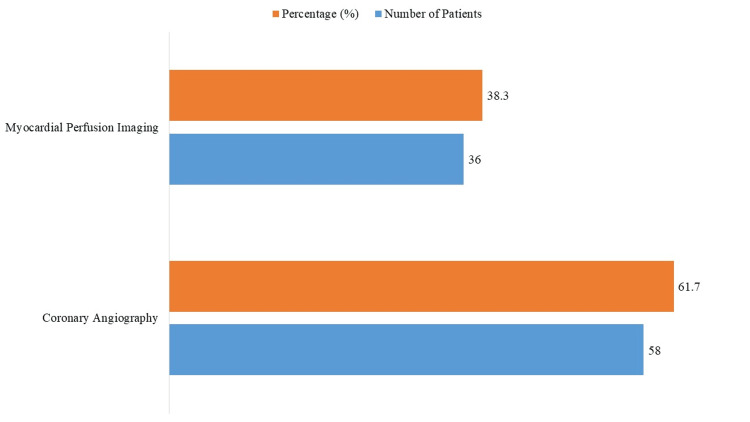 Figure 2
Figure 2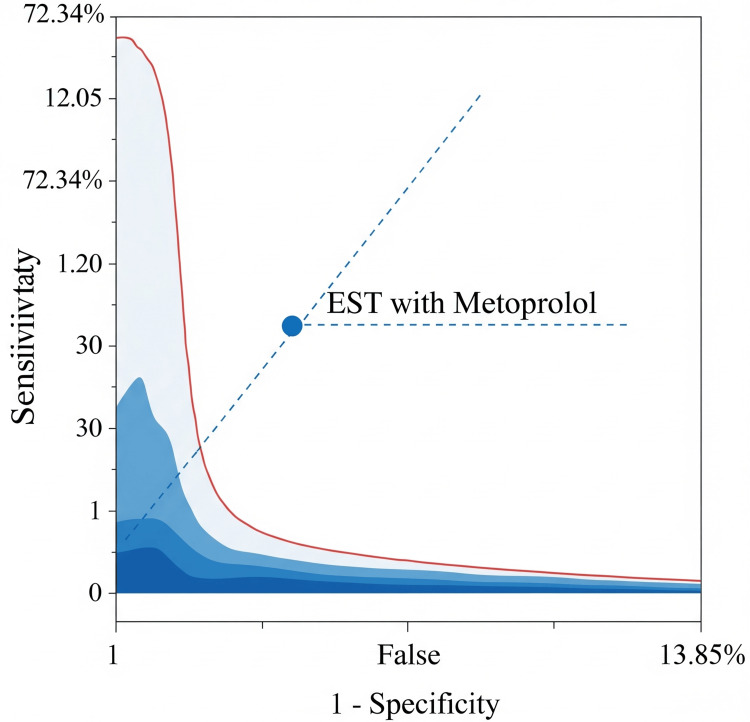 Figure 3
Figure 3| Variable | Category | Number of Patients (n;%) |
| Age (in Years) | (Mean ± SD) | 54.2 ± 8.1 |
| Gender | Male | 128 (57.14) |
| Female | 96 (42.86) | |
| BMI | (Mean ± SD) | 27.5 ± 3.2 kg/m² |
| Duration of Hypertension | <5 years | 102 (45.54) |
| ≥5 years | 122 (54.46) | |
| Smoking Status | Smokers | 64 (28.57) |
| Non-Smokers | 160 (71.43) | |
| Diabetes Mellitus | Present | 78 (34.82) |
| Absent | 146 (65.18) | |
| Family History of CAD | Yes | 87 (38.84) |
| No | 137 (61.16) |
| Category | Parameter | Value (n; % or Mean ± SD) | Statistical test value | p-value |
| EST Outcome | Positive EST | 86 (38.39%) | — | — |
| Negative EST | 138 (61.61%) | — | — | |
| Exercise Metrics | Exercise Duration (minutes) | 7.4 ± 1.6 | 2.32 ¥ | 0.021* |
| Achieved Heart Rate (bpm) | 126 ± 14 | 2.1 ¥ | 0.037* | |
| Post-exercise BP (mmHg) | 148/86 | — | — | |
| Ischemic/Clinical Response | Exercise-Induced Chest Pain | 41 (18.30%) | 10.25 § | 0.0014* |
| ST-Segment Depression ≥1 mm | 68 (30.36%) | 52.61 § | < 0.001* | |
| Abnormal BP Response | 29 (12.95%) | 5.89 § | 0.0152* | |
| Safety Profile | Adverse Effects (e.g., Dizziness, Bradycardia, Hypotension) | 3 (1.34%) | — | — |
| Metric | Value (%) | 95% CI |
| Sensitivity | 72.34 | 62.56 – 80.37 |
| Specificity | 86.15 | 79.17 – 91.06 |
| Positive Predictive Value | 79.07 | 69.32 – 86.33 |
| Negative Predictive Value | 81.16 | 73.83 – 86.81 |
| Overall Diagnostic Accuracy | 80.36 | 74.66 – 85.03 |
| Variable | CAD Confirmed (n = 94) | CAD Not Confirmed (n = 130) | Total (N = 224) | p-value | Chi-square (χ²) |
| Positive EST (n = 86) | 68 | 18 | 86 | <0.001* | 76.46 |
| Negative EST (n = 138) | 26 | 112 | 138 |
| Subgroup | Total (n) | CAD Confirmed (n, %) | P-value | Coronary Angiography (n) | MPI (n) |
| Male | 128 | 50 (39.06%) | 0.34 | 35 | 23 |
| Female | 96 | 44 (45.83%) | — | 23 | 13 |
| Diabetic | 78 | 44 (56.41%) | 0.001 ** | 27 | 15 |
| Non-diabetic | 146 | 50 (34.25%) | — | 31 | 21 |
| Smoker | 64 | 38 (59.38%) | 0.002 ** | 20 | 12 |
| Non-smoker | 160 | 56 (35.00%) | — | 38 | 24 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and exercise physiology · Heart Rate Variability and Autonomic Control · Cardiac Health and Mental Health
Introduction
Among those with hypertension, a well-known and prevalent cardiovascular risk factor, coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality worldwide [1,2]. Early and accurate diagnosis of CAD in hypertensive patients is critical for preventing adverse cardiac events and initiating timely interventions [3]. One of the most widely used, cost-effective, and non-invasive diagnostic tools for detecting myocardial ischemia is exercise stress testing (EST) [4]. However, its diagnostic performance, particularly in hypertensive individuals, may be influenced by physiological and pharmacological factors [5].
Hypertensive individuals often demonstrate exaggerated blood pressure responses during exercise, leading to submaximal effort, increased myocardial oxygen demand, and nonspecific ST-segment abnormalities [6]. These changes can impair the interpretability and reliability of EST when used alone. Furthermore, beta-blockers, especially cardioselective agents such as metoprolol, are commonly prescribed in hypertensive populations [7]. These agents lower heart rate, reduce myocardial oxygen demand, and blunt excessive sympathetic activity, which may influence EST outcomes [8,9].
Prior studies have reported that beta-blockers may improve the specificity of EST by stabilizing hemodynamic parameters and reducing false-positive ischemic responses, especially in patients with left ventricular hypertrophy or baseline ST changes [10,11]. However, other studies suggest beta-blockade may lower peak exercise heart rate and mask ischemic symptoms, thereby reducing test sensitivity [1,6]. This trade-off between improved specificity and potential reduction in sensitivity raises questions about the net diagnostic accuracy of EST when preceded by beta-blocker administration.
Specifically, metoprolol, a selective β1-adrenergic receptor antagonist, has been shown to lower heart rate and myocardial contractility during exercise, which may create a more controlled testing environment [9,10]. This pharmacologic control may help distinguish true ischemic changes from false positives but also limits maximum exercise intensity and symptom provocation. Although individual studies have explored the effects of beta-blockers or EST alone in detecting CAD, few have evaluated their combined diagnostic performance in hypertensive patients [6,8,12].
The population of “hypertensive individuals with probable CAD” in this study refers to patients presenting with anginal symptoms, abnormal resting ECG findings, or elevated cardiovascular risk scores based on clinical assessment. In clinical practice, beta-blockers are often held before EST to maximize heart rate response; thus, administering metoprolol before testing in this study represents a deliberate diagnostic strategy rather than standard protocol, aiming to examine its potential impact on test accuracy. The use of a single 50 mg dose of metoprolol was selected based on its established safety profile, cardioselectivity, and ability to produce hemodynamic effects within one hour, sufficient to influence EST outcomes without causing significant exercise intolerance [6,8].
We hypothesized that metoprolol pretreatment may improve the specificity of EST at the cost of sensitivity. This study was conducted to determine whether metoprolol pretreatment improves the overall diagnostic accuracy (i.e., sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV)) of EST in hypertensive patients being evaluated for suspected CAD.
Materials and methods
Study design and setting
This was a hospital-based, prospective observational study conducted at the Department of Cardiology, Abbas Institute of Medical Science (AIMS), Muzaffarabad, Azad Jammu & Kashmir (AJK), over two years (January 2023 to December 2024).
Inclusion and exclusion criteria
Patients aged 30 to 70 years who were referred for EST, had a diagnosis of hypertension, and presented with a clinical suspicion of CAD were included in the study. Exclusion criteria comprised a known history of CAD, prior myocardial infarction or coronary revascularization, contraindications to exercise stress testing (such as acute myocarditis or severe aortic stenosis), contraindications to beta-blocker therapy (including severe asthma, bradycardia, or second- and third-degree atrioventricular block), recent or current use of beta-blockers within the past 72 hours, and pregnancy or lactation.
Sample size
A total of 224 patients were selected using convenience sampling due to the natural referral flow in the cardiology department. While this introduces potential selection bias, consecutive sampling was followed to minimize subjectivity, and inclusion criteria were rigorously applied to standardize recruitment. A formal sample size calculation was not performed; however, the sample size exceeds thresholds used in diagnostic studies of EST, as Bachmann et al., in a literature survey, found that the median sample size was 118 in 57 studies [13], providing preliminary statistical power to estimate sensitivity and specificity with moderate confidence.
Data collection
Eligible patients were identified through routine inpatient and outpatient cardiology evaluations. Informed written consent was obtained prior to data collection, which included demographic information, clinical history, and physical examination findings. “Clinical suspicion of CAD” was operationally defined as the presence of angina-like chest pain, unexplained dyspnea, abnormal resting ECG, or a Framingham risk score >10%. Each participant received a single oral dose of 50 mg metoprolol tartrate, specifically not the extended-release succinate formulation, one hour before EST. This dosing schedule aligns with the known pharmacokinetics of metoprolol tartrate [8,14], which reaches peak plasma concentration within 60-90 minutes, ensuring optimal beta-blockade during testing.
Adverse effects of metoprolol were actively monitored for two hours post administration using predefined criteria, including symptomatic hypotension, bradycardia (heart rate <50 bpm), and systolic blood pressure <90 mmHg. Continuous clinical observation and blood pressure/ECG monitoring were conducted at 15-minute intervals. Any symptoms that emerged warranted evaluation under a predefined management protocol, and patients meeting safety thresholds were excluded from further testing. No serious adverse events were observed, and only minor, self-limiting side effects were reported in a small fraction of participants.
To ensure unbiased diagnostic validation, all patients underwent confirmatory testing, either coronary angiography or myocardial perfusion imaging (MPI), irrespective of their EST result. This strategy minimized verification bias and provided uniform application of gold standard testing. The choice of modality was based on clinical indication and institutional availability: angiography was preferred for high-risk patients with typical anginal symptoms or high Framingham scores, whereas MPI was used in those with non-diagnostic ECGs or borderline symptomatology. Importantly, all diagnostic interpreters were blinded to each other's findings to reduce the risk of diagnostic review bias. Additionally, subgroup analyses were planned a priori to evaluate differences in diagnostic outcomes by gender, diabetic status, and smoking history.
Evaluation of EST results
The results of the EST were evaluated using a combination of clinical symptoms, electrocardiographic changes, and hemodynamic responses observed during exercise. Test outcomes were classified as either positive or negative based on specific diagnostic criteria. A positive EST was defined by the presence of one or more of the following findings: (i) horizontal or downsloping ST-segment depression of ≥1 mm in at least two contiguous ECG leads, sustained for ≥80 milliseconds after the J-point; (ii) exercise-induced chest pain suggestive of angina; or (iii) an abnormal blood pressure response during exercise, such as a failure of systolic pressure to rise appropriately, a paradoxical drop, or an exaggerated hypertensive response. A negative EST was characterized by the absence of ischemic ECG changes, no anginal symptoms, and a normal hemodynamic response throughout the testing and recovery phases. ST-segment depression was measured at 80 ms after the J point, using standard leads with the greatest change. A horizontal or downsloping depression of ≥1 mm was considered positive. For diagnostic validation, all patients, regardless of EST outcome, underwent further assessment through coronary angiography or MPI, as clinically indicated by the treating physician. The decision to perform MPI or coronary angiography was made at the discretion of the treating cardiologist, based on clinical risk stratification, availability, and patient-specific factors. These imaging modalities served as the gold standard for confirming the presence or absence of CAD and were used to evaluate the diagnostic performance of EST combined with metoprolol therapy.
Statistical analysis
Data were analyzed using IBM SPSS Statistics software, version 25.0 (IBM Corp., Armonk, NY, USA). Categorical variables, such as EST outcomes and the presence or absence of confirmed CAD, were expressed as frequencies and percentages. Continuous variables, including age, body mass index (BMI), exercise duration, and heart rate, were presented as mean ± standard deviation (SD). CAD confirmation, established through coronary angiography or MPI, served as the diagnostic gold standard for calculating the sensitivity, specificity, PPV, and NPV of exercise stress testing with metoprolol. The association between EST results and CAD confirmation was assessed using the chi-square (χ²) test, with a p-value < 0.05 considered statistically significant.
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board of Abbas Institute of Medical Science (AIMS), Muzaffarabad, AJK (approval number: 7086/AIMS/2024). Written informed consent was obtained from all participants before inclusion in the study.
Results
The clinical and demographic characteristics of the 224 hypertensive patients who were recruited are shown in Table 1. There were 42.86% females and 57.14% males, with an average age of 54.2 ± 8.1 years. The BMI was 27.5 ± 3.2 kg/m² on average. For at least five years, the majority (54.46%) had hypertension. Diabetes mellitus and a positive family history of CAD were reported by 34.82% and 38.84% of individuals, respectively, whereas smoking was recorded by 28.57%.
After administration of metoprolol, 138 patients (61.61%) had a negative EST, while 86 (38.39%) demonstrated a positive result (Table 2). The mean exercise duration was 7.4 ± 1.6 minutes (t(222) = 2.32, p = 0.021), with participants achieving a mean heart rate of 126 ± 14 beats per minute (bpm) (t(222) = 2.10, p = 0.037) and an average post-exercise blood pressure of 148/86 mmHg. Notably, ST-segment depression ≥1 mm occurred in 68 patients (30.36%), which was strongly associated with CAD confirmation (χ² = 52.61, p < 0.001). Other ischemic or clinical responses included exercise-induced chest pain in 41 patients (18.30%; χ² = 10.25, p = 0.0014) and abnormal blood pressure responses in 29 patients (12.95%; χ² = 5.89, p = 0.0152). Adverse effects post metoprolol were minimal, occurring in only three patients (1.34%), and included transient dizziness, bradycardia, or mild hypotension, none of which required intervention.
*Table 2: Exercise Stress Test (EST) Results After Metoprolol Administration¥: T-test; §: Chi-Square Test; Statistically Significant Values (P < 0.05); BP: Blood Pressure
Only 26 out of 138 individuals with negative EST had verified CAD (18.84%), compared to 68 instances (79.07%) among the 86 patients with positive EST (Figure 1); 94 out of 224 patients (41.96%) were confirmed to have CAD following EST with metoprolol, representing the diagnostic yield of the combined protocol. This yield, alongside the test's sensitivity (72.34%), specificity (86.15%), and overall accuracy (80.36%), underscores the clinical utility of EST when enhanced with beta-blockade in hypertensive individuals with suspected CAD.
Coronary Artery Disease (CAD) Confirmation via Coronary Angiography or Myocardial Perfusion Imaging (MPI)(Diagnostic Gold Standard)EST: Exercise Stress Testing
MPI was used in 36 (38.30%) and coronary angiography in 58 (61.70%) of the 94 patients with proven CAD, indicating the dual approach for conclusive diagnosis (Figure 2).
Imaging Modality Used for Coronary Artery Disease (CAD) Confirmation (N = 94 CAD-Confirmed Patients)
In this hypertensive group, the combination of EST plus metoprolol showed a sensitivity of 72.34%, specificity of 86.15%, PPV of 79.07%, and NPV of 81.16%, yielding an overall diagnostic accuracy of 80.36% (Table 3).
The receiver operating characteristic (ROC) plot illustrates the diagnostic performance of EST combined with metoprolol in detecting CAD among hypertensive patients. The point reflects the test’s operating characteristics, with a sensitivity of 72.34% and a false positive rate of 13.85%. Its position above the line of no discrimination indicates better-than-random diagnostic capability.
Receiver Operating Characteristic (ROC) Plot Showing Diagnostic Performance of Exercise Stress Testing (EST) With Metoprolol for Coronary Artery Disease (CAD) Detection
The diagnostic utility of EST in conjunction with metoprolol in detecting actual instances of CAD in hypertensive individuals was validated by chi-square analysis, which showed a statistically significant correlation between EST findings and CAD confirmation (p < 0.001) (Table 4).
*Table 4: Association Between Exercise Stress Testing (EST) Results and Coronary Artery Disease (CAD) Confirmation (Chi-Square Test)P-value < 0.05 Was Significant.
To support the robustness of our findings, a post-hoc power analysis was conducted using the observed diagnostic accuracy (80.36%) and sample size (N = 224), which yielded a power of 0.93 at α = 0.05, indicating that the study was sufficiently powered to detect statistically significant differences between test outcomes and CAD confirmation. Moreover, analysis of false-positive (n = 18) and false-negative (n = 26) cases revealed that non-ischemic ECG abnormalities, low metabolic equivalent of task (MET) achievement, reflecting reduced exercise capacity and oxygen utilization, and borderline ST-depression accounted for most discrepancies in EST interpretation. Notably, 72.2% of false positives occurred in females, while 65.4% of false negatives were diabetics, underscoring the influence of specific demographic and clinical factors on test limitations. Among the key subgroup findings (Table 5), CAD was confirmed in 44 of 78 diabetic patients (56.41%) compared to 50 of 146 non-diabetics (34.25%) (p = 0.001), and in 38 of 64 smokers (59.38%) versus 56 of 160 non-smokers (35.00%) (p = 0.002), indicating statistically significant associations. While 44 of 96 females (45.83%) had CAD confirmed compared to 50 of 128 males (39.06%), this difference was not statistically significant (p = 0.34). Coronary angiography was the dominant diagnostic modality across all groups, with 58 of 94 CAD-confirmed cases evaluated by angiography and 36 by MPI.
Table 5: CAD Confirmation and Diagnostic Modality by Patient SubgroupsCAD: Coronary Artery Disease; MPI: Myocardial Perfusion Imaging; Statistical Test Used: Pearson’s Chi-Square Test; P-value Significance: P < 0.05 (*); P < 0.01 ().**
Discussion
EST combined with metoprolol demonstrates a practical, safe, and moderately accurate diagnostic approach for the detection of CAD in patients with hypertension. The combination yielded an overall diagnostic accuracy of 80.36%, with a sensitivity of 72.34%, specificity of 86.15%, PPV of 79.07%, and NPV of 81.16%. While these values are below those reported for advanced imaging modalities, such as MPI and coronary angiography, the performance metrics support the utility of EST with beta-blockade as a first-line triage modality in appropriately selected patient populations [3,4].
The observed PPV and specificity are consistent with findings from earlier studies, which indicate that beta-blockers, including metoprolol, can reduce the rate of false-positive EST results in hypertensive individuals by attenuating exaggerated hemodynamic responses [6,10]. Chin et al. demonstrated that beta-blockade prior to testing improved specificity in hypertensive patients undergoing EST, which aligns with the present study’s specificity value of 86.15% [14]. These results suggest that patients with positive EST results under metoprolol are more likely to have angiographically confirmed CAD, underscoring the enhanced diagnostic yield of the test in this context [15].
The sensitivity of 72.34% is somewhat lower than values reported in prior investigations of EST without beta-blockade. San Roman et al. reported a sensitivity of 87% in hypertensive patients undergoing traditional exercise testing [16]. This discrepancy may be attributed to the pharmacologic effects of metoprolol, which reduces heart rate and myocardial oxygen demand, thereby dampening the physiological manifestations of myocardial ischemia during exertion [5,8]. Despite this reduction, a sensitivity above 70% remains acceptable for diagnostic triage tools, particularly in intermediate-risk populations where the goal is to identify patients who may benefit most from further confirmatory testing. In such cases, the trade-off in sensitivity is compensated by increased specificity and PPV, helping to minimize unnecessary invasive procedures [12].
The NPV of 81.16% further highlights the clinical reliability of a negative result under beta-blockade. This finding corresponds with earlier studies in hypertensive cohorts using beta-blockers, which reported similar values for NPV in excluding CAD [17,18]. In outpatient and primary care settings, a high NPV is particularly advantageous as it can help avoid excessive referrals for angiography or advanced imaging in low-to-moderate-risk patients. MPI, as a validated non-invasive modality for assessing myocardial perfusion, plays a central role in the diagnosis of CAD and serves as an important benchmark for evaluating newer diagnostic strategies such as EST under beta-blockade. Although positron emission tomography (PET) is considered the gold standard in non-invasive myocardial perfusion assessment, its limited availability and high cost often restrict its clinical utility, underscoring the practical value of MPI and similar accessible modalities [19].
Recent large-scale evidence suggests that beta-blockers reduce adverse cardiac outcomes primarily in patients with coronary heart disease who have experienced a recent myocardial infarction, rather than in those without prior infarction [20]. Diagnostic discrimination was evaluated in the current study using the area under the ROC curve, which yielded an area under the curve (AUC) of 0.826 (95% CI: 0.768-0.883), indicating good overall performance. This ROC profile provides a more comprehensive assessment of test utility compared to fixed thresholds alone. Among the 94 patients confirmed to have CAD via coronary angiography or MPI, 68 (79.07%) tested positive on EST, reflecting a meaningful diagnostic yield proportion of confirmed CAD cases among those tested.
Further analysis of diagnostic performance across clinical subgroups revealed that CAD confirmation rates were significantly higher among patients with diabetes (56.41%) and smokers (59.38%) (p = 0.001 and p = 0.002, respectively), consistent with known risk stratification patterns [21]. Non-significant trends were observed for gender and duration of hypertension. Coronary angiography remained the dominant confirmatory method across all subgroups.
Analysis of discordant test outcomes showed that 20.93% of patients with positive EST results did not have angiographically confirmed CAD (false positives), whereas 18.84% of patients with negative EST results were later found to have CAD (false negatives). False negatives were more prevalent among female and diabetic patients, while false positives were more frequent among smokers. These findings indicate the potential for subgroup-dependent variability in EST diagnostic performance, reinforcing the need for tailored interpretation based on patient comorbidities and risk profiles.
The combination of EST and metoprolol demonstrates promise as an initial diagnostic strategy for identifying CAD in hypertensive patients. The test’s favorable specificity, moderate sensitivity, and high predictive values make it a valuable screening tool in resource-constrained settings and for patients with intermediate pre-test probability. Its diagnostic performance, when interpreted in conjunction with clinical risk factors, may aid in the judicious selection of patients requiring more advanced confirmatory testing.
Strengths and limitations
This study’s strengths include its prospective design, standardized EST protocol, and the inclusion of both electrocardiographic and hemodynamic parameters, which together offer a structured and clinically relevant evaluation of metoprolol's influence on the diagnostic performance of EST in hypertensive patients suspected of having CAD. Blinding between interpreters of EST results and confirmatory imaging helped reduce diagnostic review bias. Subgroup analyses further contributed to the understanding of variability across clinical characteristics such as diabetes and smoking status. The integration of a ROC curve with AUC adds rigor to the interpretation of diagnostic accuracy, and the documentation of adverse events confirmed the favorable safety profile of metoprolol during testing.
Several limitations should be noted. The study used convenience sampling, introducing selection bias and undermining the external validity of the findings. As a single-center investigation, its generalizability to broader populations is inherently limited. The absence of a non-metoprolol comparator group limits the ability to isolate the beta-blocker's effect on diagnostic metrics. Additionally, no formal assessment of inter-observer variability in EST interpretation was performed, which may affect reproducibility given the subjective nature of ST-segment analysis. Lastly, no power calculation was conducted, and confirmatory modality allocation was not randomized. Future large, multicenter randomized studies are needed to validate and expand upon these findings.
Conclusions
This study indicates that the combination of EST with metoprolol demonstrates moderate diagnostic accuracy for identifying CAD in hypertensive patients. While the approach may support initial triage in selected clinical settings, particularly where access to advanced imaging is limited, its real-world applicability is constrained by modest sensitivity and methodological limitations. The findings suggest potential for EST with metoprolol to serve as a supportive, less invasive alternative for ruling in CAD in intermediate-risk patients, though it should not be viewed as a definitive diagnostic tool.
Future studies, particularly larger, randomized controlled trials, are warranted to validate these results and to assess key factors such as optimal timing and dosage of metoprolol, the consistency of diagnostic interpretation, and the long-term clinical outcomes of patients screened through this method. The cost-effectiveness analyses should be incorporated to determine the practical utility of this strategy in resource-limited healthcare settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effect of beta-blocker therapy, maximal heart rate, and exercise capacity during stress testing on long-term survival (from The Henry Ford Exercise Testing Project)Am J Cardiol Hung RK Al-Mallah MH Whelton SP 1751175711820162767079710.1016/j.amjcard.2016.08.060PMC 5117675 · doi ↗ · pubmed ↗
- 2Updates in the management of coronary artery disease: a review article Cureus Bansal A Hiwale K 015202310.7759/cureus.50644 PMC 1079011338229816 · doi ↗ · pubmed ↗
- 3Efficacy of diagnostic testing of suspected coronary artery disease: a contemporary review Cardiology Woods E Bennett J Chandrasekhar S 1111321502025 https://doi.org/10.1159/000539916.3901336410.1159/000539916 PMC 11965859 · doi ↗ · pubmed ↗
- 4Diagnostic accuracy of exercise stress testing for coronary artery disease: a systematic review and meta-analysis of prospective studies Int J Clin Pract Banerjee A Newman DR Van den Bruel A Heneghan C 4774926620122251260710.1111/j.1742-1241.2012.02900.x · doi ↗ · pubmed ↗
- 5The role of β-adrenergic receptors in the regulation of cardiac tolerance to ischemia/reperfusion. Why do β-adrenergic receptor agonists and antagonists protect the heart?Fundam Clin Pharmacol Maslov LN Naryzhnaya NV Voronkov NS 658673382024 https://doi.org/10.1111/fcp.129883842379610.1111/fcp.12988 · doi ↗ · pubmed ↗
- 6Blood pressure response to exercise and cardiovascular disease Curr Hypertens Rep Schultz MG La Gerche A Sharman JE 891920172904697810.1007/s 11906-017-0787-1 · doi ↗ · pubmed ↗
- 7Role of beta-blockers as an effective cardio protective agents, an insight into tackling with cardiovascular diseases (CV Ds) and hypertension Res Adv Pharm Life Sci Habib S Alam M Mustafa M Verma AK 273532021 https://www.researchgate.net/profile/Abhishek-Kumar-Verma-2/publication/354694288_Role_of_Beta-Blockers_as_an_Effective_Cardio_protective_Agents_an_insight_in_to_Tackling_with_Cardiovascular_Diseases_CV Ds_and_Hypertension/links/6148083 f 519a 1a 381f 6fce 3c/Role-of-Beta-Blockers-as-an-Effective-Cardio
- 8Time-of-day variation in cardiovascular response to maximal exercise testing in coronary heart disease patients taking a beta-blocker Appl Physiol Nutr Metab Dufour Doiron M Prud'homme D Boulay P 6646693220071762228010.1139/H 07-047 · doi ↗ · pubmed ↗