High-throughput measurement of adipocyte size with open-source software using whole-slide adipose tissue images
Alan Ramalho, Marie-Frédérique Gauthier, Ina Maltais-Payette, Giada Ostinelli, Frédéric Hould, Laurent Biertho, André Tchernof

TL;DR
This study developed a fast, open-source automated method to measure fat cell sizes in tissue samples, which is useful for studying metabolic health.
Contribution
A validated open-source automated method for high-throughput adipocyte diameter measurement using whole-slide images.
Findings
Automated and manual methods showed strong correlation (r = 0.87) in measuring adipocyte diameters.
Omental adipocyte sizes correlated with cardiometabolic risk markers using both methods.
No significant differences were found between manual and automated methods for subcutaneous adipose correlations.
Abstract
The aim of this study was to create and validate a high-throughput method based on open-source software for the measurement of adipocyte diameters in white adipose tissue histological sections. Human omental and subcutaneous adipose tissue samples collected during bariatric surgery were used to prepare haematoxylin and eosin-stained histological slides. Adipocyte diameters were measured both manually and with an automated procedure created using ImageJ. Comparative analysis of our automated method with the manual measurement and associations of the mean adipocyte diameters with cardiometabolic markers were used to validate our method. A total of 377 adipose samples (190 participants) were included in the analysis. Pearson correlation of mean adipocyte diameters showed a strong linear relationship between methods (r = 0.87, p < 0.0001). Omental adipocyte diameters of both methods were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
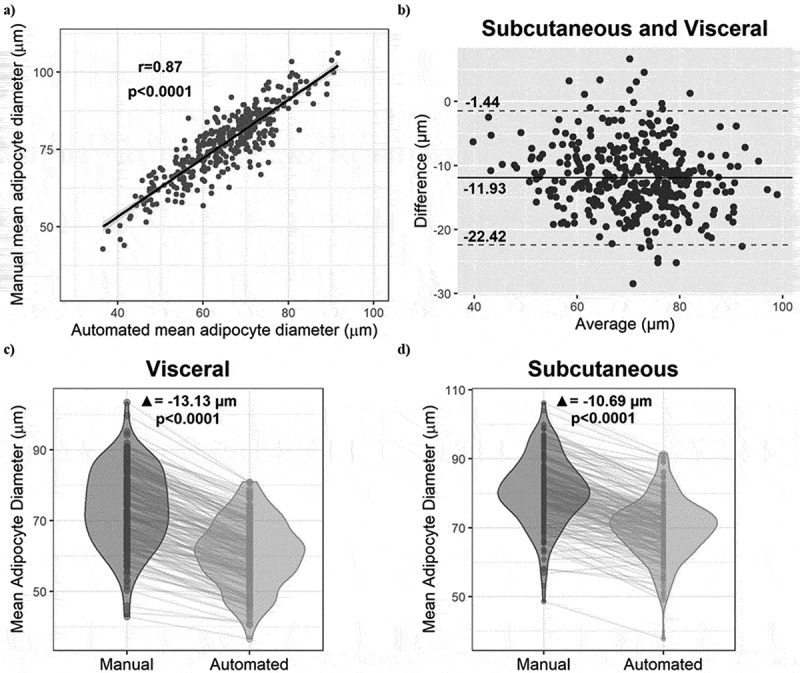 Figure 1
Figure 1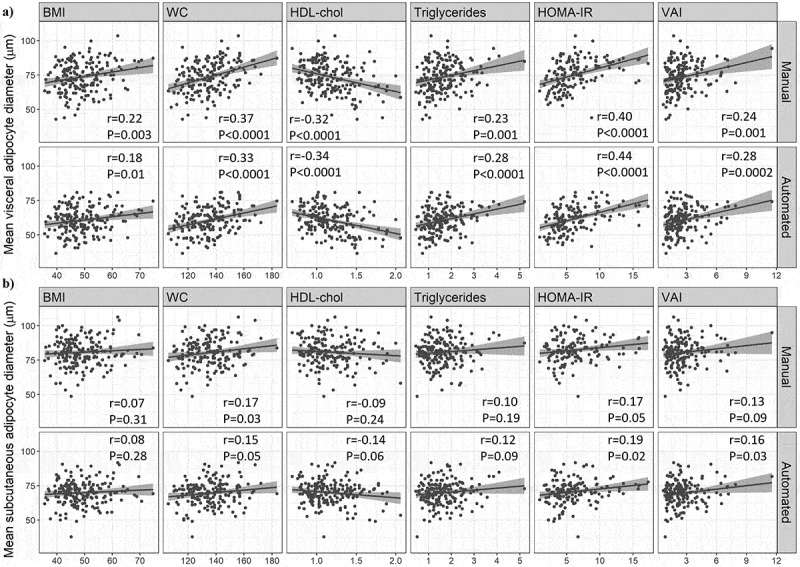 Figure 2
Figure 2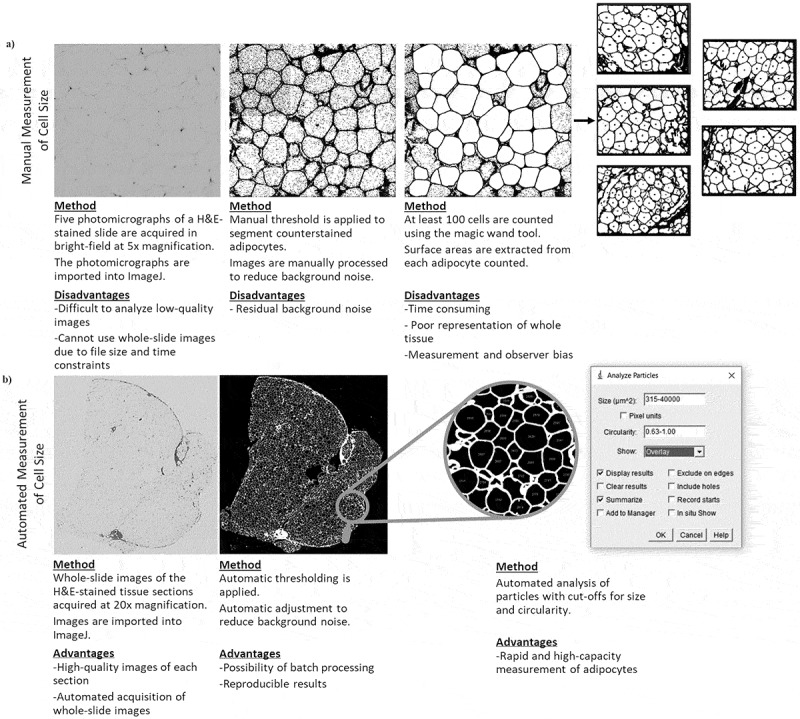 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5- —Natural Sciences and Engineering Research Council of Canada10.13039/501100000038
- —Fonds de Recherche du Québec (FRQ)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Disease and Adiposity · Adipose Tissue and Metabolism · Adipokines, Inflammation, and Metabolic Diseases
Introduction
The worldwide burden of cardiometabolic diseases continues to increase, emphasizing the importance of cardiometabolic research [1]. However, this research is hindered by a lack of reliable cardiometabolic health markers. Body mass index (BMI) has long been used as it is easily obtained, but it is a poor indicator of individual cardiometabolic risk. Other metrics that better estimate this risk and its drivers are increasingly favoured in clinical practice and in research [2]. One such metric is adipocyte size. A major driver of obesity-related cardiometabolic dysregulation is adipose tissue dysfunction, which is characterized by low free fatty acid uptake, impaired triglyceride synthesis, impaired lipid storage, insulin resistance, fibrosis, immune cell infiltration, increased proinflammatory cytokine secretion, reduced adipogenesis, and adipocyte hypertrophy [3–6]. These last two characteristics indicate the importance of the mechanism of adipose tissue expansion in the development of disease. Studies have shown that expansion via hyperplasia (adipogenesis), typical of subcutaneous (SC) depots, seems to favour the preservation of cardiometabolic health [3,4]. Conversely, expansion via hypertrophy, the enlargement of existing adipocytes, is indicative of adipose tissue dysfunction, visceral obesity, metabolic dysregulation, and increased cardiometabolic risk [3–5,7]. Consequently, adipocyte size is commonly used in cardiometabolic research as a marker of adipose tissue function and cardiometabolic health [5,7,8]. Furthermore, analysis of adipocyte size can help better understand the pathophysiological processes of obesity and characterize treatment responses to dietary interventions, nutraceuticals, bioactive compounds, and medication [9,10]. However, measurement of adipocyte size is affected by unresolved issues.
Currently, there is no gold standard method to measure adipocyte size [5,7]. There are three main methods utilized in research: imaging of collagenase digestion-isolated adipocytes, sizing of osmium tetroxide-fixed cells, and histomorphometry [4,5]. Histomorphometry involves analysing haematoxylin and eosin (H&E) -stained histological slides of adipose tissue using an optical microscope to measure the diameter or cross-sectional area of the adipocytes [5]. This method is considered to be the most reliable, but still has drawbacks [9]. First, tissue fixation reduces volume of the cells by approximately 15% and there are inherent assumptions including uniform cell size distribution [5,11]. Furthermore, inter-laboratory sample processing differences are important to consider as improper technique can result in distortion, crush artefacts, and staining artefacts that can impede measurement [5,7,9,11]. Differences can also exist regarding specificities in cell sizing protocols which may influence the final results and the ability to compare results between laboratories [12,13]. The most important drawbacks, however, are that this method is very labour-intensive, time consuming, and has a high risk of measurement and observer bias as it requires the measurer to visually identify each adipocyte in the tissue section and then measure their diameter or cross-sectional surface area [8,9,14]. Due to the time required, only 100 to 300 cells per sample are typically measured, decreasing estimation accuracy [11,14]. The latter issues are inherent to manual histomorphometry and could be resolved with automation.
The advent of biological image analysis software has enabled such automation to be possible. To address the main drawbacks of the histomorphometric method, several teams have developed automated programmes or protocols to detect and measure adipocyte size using histological slides [8–10,13–18]. However, many of these automated solutions have issues such as adaptability, cost, reliability, accessibility (both short- and long-term), and usability. Many tools cannot be sufficiently adapted to account for considerable procedural differences, such as initial sample quality, fixation, paraffin embedding, microtomy, staining, and imaging [12]. The costs of paid software solutions and required equipment can be prohibitive [14]. Some software tools have been discontinued or are not accessible through secure channels [8,10,17,18]. A noteworthy exception to these issues is ImageJ (National Institutes of Health, USA). ImageJ is a free easily accessible open-source scientific image processing and analysis software platform originally created by the National Institutes of Health of the United States [19]. ImageJ is relatively easy to use and has been widely adopted by the scientific community.
Many of the current software solutions typically analyse digital photomicrographs of the tissue sample, limiting the number of adipocytes measured [10,11,14]. Photomicrographs are used for manual analysis as manually measuring each adipocyte in a complete section would require an exorbitant amount of time. Cell sizing software tools should be capable of analysing whole-slide images of the tissue samples to maximize the number of adipocytes measured [14]. However, many of the free software options were not designed to do this due to file size restrictions. Recent advancements in both file size capacity of software tools (including ImageJ) and the affordability of slide scanners for the acquisition of high-quality whole-slide images have opened the door for significant progress in this regard [14].
Ultimately, the issues with the current histomorphometric methods enumerated above, namely variations between cell sizing protocols, the considerable labour and time requirements as well as the risk of measurement and observer bias impede the use and reliability of this method. The aim of this study was to develop and validate an easy-to-use method to measure adipocyte size in whole tissue images. We hypothesized that measurements can be performed automatically and that average adipocyte diameter measurements obtained with the automated method are consistent with those obtained with the manual method, while requiring significantly less time and measuring a larger number of cells per sample. Additionally, we hypothesized that the results obtained with the automated method are at least non-inferior to those of the manual method for the prediction of cardiometabolic risk markers.
Results
Manual and automated cell size measurements
2.1.
Regarding the initial elaboration phase of our study, the average adipocyte diameters from 16 samples obtained with the manual and automated methods were compared for the purpose of establishing measurement parameters. Spearman correlation analysis showed a strong significant association between the methods (r = 0.90, p < 0.0001). Paired t-test analysis indicated that the average adipocyte diameters obtained with the two methods were not significantly different (p = 0.10) (data not shown).
For the validation study, 370 and 374 samples (for the manual method and automated method, respectively) of the 377 samples from the 190 participants were included in the analysis ([Table 1 and Table 2](#t0001 t0002)). As shown in Table 2, the average adipocyte diameter for all tissues from both depots combined was 77.1 ± 11.0 µm and 65.2 ± 10.1 µm for the manual and automated method, respectively. These average diameters were shown to be significantly different by paired t-test (p < 0.0001) (data not shown). The approximate amount of time dedicated to the manual analysis was 10 minutes per tissue compared to 0.8 minute per tissue for the automated method (based on a subgroup of 300 samples). The automated method detected an average of 879 ± 511 cells compared to 130 ± 34 cells for the manual analysis (p < 0.0001). The relationship between the methods was not significantly influenced by biological sex, as determined with multiple linear regression (data not shown).Table 1.Anthropometric and biochemical characteristics of the participants. n or Mean ± SDMin – MaxParticipants (n)190 Sex (male/female)46/144 Age (years)38.0 ± 8.619–59BMI (kg/m^2^)49.0 ± 7.335.6–74.8Visceral adiposity index (VAI)2.65 ± 1.620.69–11.26Waist circumference (cm)135 ± 14106–184Triglycerides (mmol/L)1.64 ± 0.760.45–5.20HDL-cholesterol (mmol/L)1.18 ± 0.270.69–2.06LDL-cholesterol (mmol/L)2.73 ± 0.731.13–6.25Total cholesterol (mmol/L)4.63 ± 0.882.54–9.47Glucose (mmol/L)5.4 ± 0.44.2–7.7HOMA-IR6.2 ± 3.30.9–17.3Apo B (g/L)0.96 ± 0.210.52–1.96Data are presented as total number (n) for the first two rows, and as mean plus or minus standard deviation (SD) and minimum-maximum values in the remaining rows. BMI: body mass index; HDL: high-density lipoprotein; LDL: low-density lipoprotein; HOMA-IR: homoeostasis model assessment of insulin resistance; apo B: apolipoprotein B.Table 2.Results of the histomorphometric analyses of all samples using the manual and automated methods. Manual methodAutomated methodSamples analysed (n)370374Time required for analysis^a^10 minutes/section0.8 minute/sectionAverage number of cells measured^b^130±34 cells879±511 cellsAverage cell diameter^b^77.1±11.0 µm65.2±10.1 µm^a^Includes time required for file processing and handling. ^b^Data are presented as mean plus or minus standard deviation (SD).
Comparisons between manual and automated cell size measurements
2.2.
A Pearson correlation analysis was performed between the manual and automated mean cell size (for the two depots) and is presented in Figure 1a. The Pearson coefficient of r = 0.87 indicates that the two methods are strongly consistent. We observed in the Bland-Altman plot in Figure 1b an average difference of −11.93 µm between the mean automated and manual cell diameters, as well as limits of agreement of −1.44 µm and −22.42 µm. Most of the data points are within the limits of agreement, indicating good agreement between methods. The magnitude of the difference does not appear to vary based on the average diameter, suggesting the absence of systematic bias related to the magnitude of the measurement [20]. Multiple linear regression analysis also indicated that the association between automated and manual average adipocyte diameter measurements does not vary significantly across tertiles of manual average adipocyte diameters (data not shown). Figure 1c,d show that the average cell size measured with the automated method is significantly smaller compared to the manual method in both the visceral and SC depots (−13.13 µm, p < 0.0001 and −10.69 µm, p < 0.0001, respectively) and this is also true for the majority of individual samples. Figure 1.Comparison of adipocyte diameters measured by the two methods. (a) Pearson correlation of all mean cell diameters (omental and SC) between the manual and automated methods. (b) Bland-Altman plot of the agreement between the automated and manual analyses. (c) Paired t-test between the two methods in omental adipose tissue samples. (d) Paired t-test between the two methods in subcutaneous adipose tissue samples.(a) Scatterplot with a trendline showing a strong positive correlation between manual mean adipocyte diameters on the y-axis and automated mean adipocyte diameters on the x-axis, in micrometres. The Pearson r is 0.87 and the p-value is less than 0.0001. (b) Bland-Altman scatterplot of the difference between automated and manual average diameters on the y-axis and the average on the x-axis, in micrometres, both tissue depots combined. The mean difference is -11.93 micrometres, and the limits of agreement are -1.44 and -22.42 micrometres, respectively. (c) Violin plot of the mean omental adipocyte diameters, in micrometres, as measured using the manual and automated methods, respectively, with lines connecting individual tissue samples. The automated diameters are consistently smaller than the manual ones, with an average difference of -13.13 micrometres and a p-value less than 0.0001. (d) Violin plot of the mean subcutaneous adipocyte diameters, in micrometres, as measured using the manual and automated methods, respectively, with lines connecting individual tissue samples. The automated diameters are consistently smaller than the manual ones, with an average difference of -10.69 micrometres and a p-value less than 0.0001.
Associations with metabolic markers
2.3.
The participants for this study were on average 38.0 ± 8.6 years old, including 46 males and 144 females with an average BMI of 49.0 ± 7.3 kg/m^2^ and an average waist circumference of 135 ± 14 cm (Table 1). Pearson correlation analyses were performed to evaluate the association between cardiometabolic health markers and the mean adipocyte diameter obtained with each measurement method (i.e. manual and automated) for each adipose tissue depot. The results are presented in Figure 2. The automated cell size method was not significantly different from the manual method for any of the correlations between average adipocyte diameter and cardiometabolic health markers for either depot, as determined using Meng’s Z-test (data not shown). Figure 2.Comparison of the associations between average adipocyte diameter and metabolic health markers according to adipocyte measurement method. (a) Pearson correlations between mean adipocyte diameter (measured using both the manual and automated methods) and BMI (body mass index), WC (waist circumference), HDL-Chol (high-density lipoprotein cholesterol), triglycerides, HOMA-IR (Homoeostasis model assessment of insulin resistance) and VAI (visceral adiposity index) in omental adipose tissue samples. (b) Pearson correlations between mean adipocyte diameter (measured using both the manual and automated methods) and BMI (body mass index), WC (waist circumference), HDL-Chol (high-density lipoprotein cholesterol), triglycerides, HOMA-IR (Homoeostasis model assessment of insulin resistance) and VAI (visceral adiposity index) in subcutaneous adipose tissue samples.(a) A series of 12 Scatterplots of the associations between mean visceral adipocyte diameter in micrometres measured using the manual and automated methods, respectively, and body mass index, waist circumference, high-density lipoprotein cholesterol, triglycerides, the Homoeostatic Model Assessment for Insulin Resistance, and the visceral adiposity index. (b) A series of 12 Scatterplots of the associations between mean subcutaneous adipocyte diameter in micrometres measured using the manual and automated methods, respectively, and body mass index, waist circumference, high-density lipoprotein cholesterol, triglycerides, the Homoeostatic Model Assessment for Insulin Resistance, and the visceral adiposity index.
Regarding the omental depot, we observed in Figure 2a, although not significantly different between methods, a slightly stronger correlation and lower p-value with the automated method with triglyceride (TG) levels (r = 0.28, p < 0.0001 vs r = 0.23, p = 0.001), HDL-Cholesterol (HDL-Chol) (r = −0.34, p < 0.0001 vs r = −0.32, p < 0.0001), the homoeostasis model assessment of insulin resistance (HOMA-IR) (r = 0.44, p < 0.0001 vs r = 0.40, p < 0.0001), and the visceral adiposity index (VAI) (r = 0.28, p = 0.0002 vs r = 0.24, p = 0.001) compared to the manual method.
Regarding the SC depot (Figure 2b), although not significantly different between methods, a slightly higher correlation strength was observed with the automated method for the association with HOMA-IR (r = 0.19, p = 0.02 vs r = 0.17, p = 0.05) and VAI (r = 0.16, p = 0.03 vs r = 0.13, p = 0.09) compared to the manual method. Notably, the association with VAI became significant with the automated method.
No significant associations were observed with total Cholesterol (Chol), LDL-Chol, and apolipoprotein B (apoB) with either method in either depot.
Discussion
Our analysis shows that our automated method for measuring adipocyte size is rapid, valid, and reliable. Pearson correlation analysis shows a strong agreement between both methods for the determination of mean adipocyte diameters. Pearson correlation analyses and Meng’s Z-test also demonstrate that the strength of the associations between different cardiometabolic health markers and mean adipocyte diameters measured using the automated method were equivalent to the associations with the manual method. Adipocyte size is often used in research as a marker of adipose tissue function and cardiometabolic health. As such, the significant associations between other cardiometabolic health markers and the automated mean adipocyte diameter and their agreement with the associations with the manual mean adipocyte diameters clearly demonstrate the validity of our method. It should be noted that the weight status of the participants in this study likely influenced these associations. Expansion through hypertrophy has its limitations as adipocytes can only increase in volume up to a certain point [3,5]. Mean fat cell size eventually plateaus in individuals with large adiposity excess as can be the case with candidates for bariatric surgery [3,5,13]. This plateauing weakens the ability to detect significant associations with other variables [5]. This may explain the lack of significant associations with some of the cardiometabolic risk markers and why the associations observed with BMI and waist circumference (WC) were weaker than expected based on data from other studies [4,11].
Despite the strong association between methods, the paired t-test, grouped violin plots, and the Bland-Altman plot demonstrate that the automated mean adipocyte diameters are on average significantly smaller than those of the manual method. The average difference between the two methods is 11.9 µm. Because there is no gold standard method for cell size measurement, it is possible that this difference reflects better estimation of average cell size by our automated method compared to the manual method. The manual method is dependent on the judgement of the user in both the selection of the tissue section subregions to use and the identification of adipocytes to measure. The selection of subregions is ideally completely randomized, but many factors such as section edges, damaged subregions, and fibrotic subregions can influence this selection. This may result in preferentially identifying better-looking subsections. Large adipocytes may be easier to notice and identify visually than smaller ones, which could result in an overestimation of average size with the manual approach. The automated method targets the entire section, thereby eliminating such biases. Analysing the entire histological section instead of a few subregions also greatly increases the number of cells measured for each sample. Increasing the number of cells measured increases the likelihood that the estimation of average cell size is accurate [14]. Other teams have obtained similar differences in mean adipocyte size. Maguire et al. and Palomäki et al. [13,14], both observed that mean cell size was smaller when using an automated method with whole-slide images compared to methods that used photomicrographs of tissue sections. Interestingly, Maguire et al. [14] only observed this in high-fat diet mice, and the opposite was true for chow-fed mice. Like us, Palomäki et al. [13] used adipose tissue samples from patients with obesity, but the difference that they observed between sizing methods was much smaller at −0.8 µm. This may be due to methodological differences between their study and ours as they manually measured approximately 300 cells per sample using photomicrographs while also using a smaller number of tissue samples [13]. Due to these reasons and the significant correlations with cardiometabolic risk markers previously discussed, it is possible that our automated method produces a more reliable estimation of mean adipocyte size compared to the manual method.
Our method has several advantages compared to the manual method. As discussed, our automated method is significantly faster and uses whole-slide images of H&E-stained tissue sections, significantly increasing the number of adipocytes measured. The automated detection of adipocytes reduces the potential for observer and measurement bias. Our method is also very easy to implement as its main component is a macro for ImageJ, that we provide here and can easily be copied, making it very accessible. The only software needed is ImageJ, which is free, easily accessible, and can be run on low-powered computers. The fact that ImageJ was developed by the NIH and that it has a dedicated userbase provides good assurance that it should be maintained for the foreseeable future. ImageJ is also easy to learn, especially for this application.
As mentioned, other teams have developed automated protocols using software, but many of these solutions have issues including software cost, short- and long-term accessibility, and the inability to use whole-slide images. Notable exceptions to most of these issues are Adiposoft, a plugin created for ImageJ, and QuPath, another free open-source software for the analysis of digital biological images [9,14,21]. Adiposoft was created and validated to analyse the number and size of white adipocytes from adipose tissue histological sections [9,22]. Originally, it only analysed photomicrographs but is now capable of analysing whole-slide images. Indeed, Adiposoft is a capable programme solution, but we encountered issues when attempting to use it with our samples. While Adiposoft analysed many of our samples without issue, there were significant problems with some samples such as adipocytes not being detected and the identification of large empty areas as adipocytes. Our experience suggests that it may not be readily adaptable Adiposoft, using its current configuration options, to certain experimental conditions. Adiposoft also outputs a unique spreadsheet for each image, complicating data management when analysing many samples. QuPath is a powerful tool for the analysis of whole-slide images and large 2D data [21]. Maguire et al. developed an interactive plugin for QuPath for the measurement of adipocytes [14]. Their results show that their method reliably measures adipocyte number and size from whole-slide images [14]. However, their method involves several steps that require both QuPath and ImageJ. The adaptability of their method to different experimental conditions is also uncertain. The QuPath method developed by Palomäki et al. only uses tools that are already built into QuPath and no other analysis software is required. Their analysis shows that the method is valid for good and average quality whole-slide images and photomicrographs [13]. However, the method requires training a pixel classifier with good quality histology sections of adipose tissue [13]. This step increases the complexity and requires technical knowledge, which may hinder other teams from adopting the method. Ultimately, even with free software solutions capable of analysing whole-slide images, there are issues that hinder their adoption. In contrast, our method is more straightforward and simpler to implement. It requires only ImageJ and our macro, which is arguably easier. Our macro uses standard image processing methods, which should allow other teams to easily understand it and adapt it to their experimental conditions. Furthermore, the macro does not need to be downloaded, maximizing its accessibility.
Our study has several strengths. First, to validate our automated approach, we used both correlation analyses and Bland-Altman plots to evaluate the strength of the linear relationship and agreement between the methods, respectively. While a strong correlation is expected, it does not indicate that there is good agreement [20]. Bland-Altman plots evaluate the differences between the methods, allowing for a better determination of comparability [20]. Second, 367 white adipose tissue samples obtained from male and female human participants were analysed by both methods. Such a large sample size greatly increases the validity of our analysis and is much larger than samples used by other teams in the validation of their cell-sizing tools [14–16]. Furthermore, we used both SC and omental adipose tissue samples from patients from two different cohorts, which indicates how our automated approach can be applied to different scenarios. Third, we evaluated how the methods influence the associations between cardiometabolic health markers and mean cell diameters to establish the validity and usefulness of our automated analysis.
This study does have some limitations. First, all the samples came from participants with obesity undergoing bariatric surgery. As such, it cannot be stated for certain that our method would adequately perform in populations without obesity. This is unlikely to be an issue due to obesity being a very heterogeneous disease and that we used a very large sample size which included varied types of cellular morphologies. Rodent white adipose tissue is similar to that of humans regarding morphology and gross anatomical regions, indicating rodent tissues could likely be analysed with our method [17]. Second, all the histological slides were prepared by the histology department at our Institute by highly trained technicians using high-quality equipment. The slides were typically of high quality. As such, our method may not function well with lower quality slides. However, poor quality slides are an impediment to all sizing methods, and, as mentioned, our macro can be adapted to optimize its performance to different experimental conditions. Our method also requires the use of whole-slide images with uniform illumination, but the recent decrease in the cost of slide scanners alleviates this issue [14]. Third, only mean adipocyte diameter was considered and not adipocyte size distribution in each sample. As only approximately 100 adipocytes were measured per sample, it is possible that some size subgroups would be underrepresented with the manual method, resulting in the comparison of the two methods in this regard to be of questionable relevance.
In conclusion, we have successfully developed a rapid, automated method for the measurement of adipocytes in H&E-stained histological sections of white adipose tissue. This automated method consists of a straightforward macro for ImageJ that analyses whole-slide images of histological white adipose tissue sections. We have shown that this method is valid and reliable. Compared to the usual manual method, our automated method allows for the measurement of a much greater number of cells while requiring considerably less time. Furthermore, our method can easily be adopted and adapted by other teams, which could increase uniformity between laboratories.
Methods
Participants characteristics and tissue sampling
4.1.
Participants are patients who underwent bariatric surgery and were recruited through the Biobank infrastructure at the Institut universitaire de cardiologie et de pneumologie de Québec – Université Laval. All participants provided written, informed consent. This study was approved by the medical ethics committees of Laval University (approval numbers 2017–2710, 2021–3398 and 2019–3218) and adheres to the principles of the Declaration of Helsinki. Clinical and anthropometric characteristics such as age, sex, height, weight, BMI, and waist circumference were recorded during the pre-surgery consultation or on the morning of surgery. Fasting blood samples were obtained and lipid profiles (total Chol, HDL-Chol, LDL-Chol, TG, and apoB levels) and haematological parameters (fasting insulin, fasting glucose, and HbA1c) were measured by the biochemistry department of the Institute. Omental and SC adipose tissue samples were collected from the greater omentum and the abdominal SC adipose tissue compartment, respectively, during surgery and immediately frozen at −80°C. Approximately 60 to 80 mg of frozen adipose tissue was fixed in 10% formalin (Sigma-Aldrich®, HT501128) overnight at 4°C and embedded in paraffin the following day in accordance with our validated protocol [12]. Five-µm sections were mounted on glass microscope slides and stained with H&E. For each tissue sample, the same histology slide was used for both the manual and automated measurements of cell size. However, 5 subregions of the tissue section were used for the manual assessment, whereas the automated method assessed the entire section. HOMA-IR was calculated according to the equation: fasting insulin (µU/mL) * fasting glucose (mmol/L)/22.5 [23]. VAI was calculated using validated sex-specific equations [24]. The equations are as follows: [24].
Initially, a small group of 16 samples were selected for the elaboration of the automated method and an initial validation. The samples were obtained from four participants (two men and two women, 45 ± 9.7 years old, BMI 48 ± 6.6 kg/m^2^ at the time of bariatric surgery). This group allowed us to determine the parameters for the automated protocol in a variety of cell size ranges using adipose tissue samples from two depots.
Subsequently, validation of the method was performed using 377 white adipose tissue samples (188 omental and 189 subcutaneous) from 190 participants who had undergone bariatric surgery and were included in this study. Due to issues encountered during sizing, the results from 370 and 374 tissue samples that were analysed by the manual and automated methods, respectively, were used in the analyses.
Manual adipose cell size measurements
4.2.
Briefly, five subregions with minimal damage and artefacts were randomly acquired from each histological adipose tissue section using a Leica DMLB microscope (Leica, Wetzlar, Germany) coupled with a MotiCam580 (Motic, British Columbia, Canada) at 5x magnification for each sample and saved in TIF format. Manual histomorphometric analyses were performed blinded to patient identity or type of depot according to the method described by Laforest et al. [12]. Each digital photomicrograph was converted to 8-bit, the background was subtracted, background noise was reduced using a median filter, and a manual threshold was applied to convert the images to binary in order to segment adipocytes using ImageJ (National Institutes of Health, USA). The thresholds were specifically chosen for each subregion to achieve the best segmentation of adipocytes, as determined by the measurer. The cross-sectional area of each adipocyte was manually measured using the wand tool on each image. Incomplete cells on the edge of the images were excluded. The paintbrush tool was used to smooth the cell surface or fill-in membranes when needed. A minimum of 100 cells per tissue were measured as this is the minimum number of adipocytes required to accurately estimate average surface area while minimizing variance [17]. The cross-sectional areas were used to calculate diameters, expressed in µm.
Automated adipose cell size measurements
4.3.
Whole-slide images were acquired with an Axio Scan Z1 slide scanner (Zeiss, Oberkochen, Germany) at 20x magnification and saved in TIF format. The whole-slide digital images were then imported into ImageJ and processed by our automated cell sizing macro. The macro first converted the whole-slide digital images to 8-bit images and then into binary. The threshold used for binary conversion was adjusted and optimized automatically for each image using triangle thresholding. Triangle thresholding was chosen as it resulted in the best segmentation of the adipocytes among the multiple thresholding methods tested during the elaboration and initial validation phase. The automatic thresholding compensates for variations in illumination and H&E staining intensity observed across samples during image acquisition. The operations erosion and outlier removal were also applied automatically by the macro to reduce background noise. The operations to reduce noise were selected based on the testing during the elaboration and initial validation phase. The macro then automatically performed area analysis through a particle analysis component in ImageJ.
The particle analysis is based on the size and the circularity of objects. Minimum and maximum size cut-offs of 315 and 40,000 µm^2^ (equivalent to a diameter of 20 and 225 µm), respectively, were applied so all objects inferior to 20 µm and superior to 225 µm in diameter were excluded. The minimum cut-off enabled the exclusion of objects unlikely to be adipocytes. The maximum cut-off is important to account for potentially damaged tissues. Objects larger than 225 µm in diameter likely represent two or more cells where the cell membrane collapsed or was damaged during tissue processing. This would result in an overestimation of cell size. The roundness of mature adipocytes allows the use of circularity as an important component of this analysis. Different circularity value cut-offs were tested during the initial elaboration and validation phase. The circularity cut-off values have been selected to maximize the number of detected cells while having the best fit with the manual cell sizes without including false detections due to poor tissue quality (cell damage). Once the steps of the procedure were established, the different parameters were incorporated into a macro file in ImageJ to perform automatic fast-paced analysis on all images. The macro is as follows:
run(‘8-bit’);
setAutoThreshold(‘Triangle dark’);
//run(‘Threshold…’);
setOption(‘BlackBackground’, false);
run(‘Convert to Mask’);
run(‘Erode’);
run(‘Remove Outliers…’, ‘radius = 2.5 threshold = 50 which = Bright’);
run(‘Erode’);
run(‘Remove Outliers…’, ‘radius = 5.5 threshold = 50 which = Bright’);
run(‘Analyze Particles…’, ‘size = 315–40000 circularity = 0.63–1.00 display exclude summarize add’);
Surface areas were extracted and converted to diameters expressed in µm. For quality assurance, when the number of detected cells was less than 200, the whole-slide image was visually inspected to determine why the count was low. If there was an issue in cell detection, the threshold was manually adjusted to improve segmentation and the image was reanalysed. If the detection of cells appeared accurate, the initial results were kept if the total number of cells detected was greater than 100. If less than 100 cells were detected, this was considered insufficient, and the results were omitted from subsequent analyses. A simplified schematic overview of the two methods is presented in Figure 3. Figure 3.Overview of the manual and automated adipocyte measurement procedures. (a) Schematic overview of the manual adipocyte diameter measurement procedure in ImageJ with disadvantages of each step. (b) Schematic overview of the automated adipocyte diameter measurement procedure in ImageJ with advantages of each step.(a) A 4-panel diagram with images outlining the manual image processing and cell sizing for an adipose tissue photomicrograph, accompanied by a text description of the main steps and disadvantages below the images. The text specifies that the images were acquired in brightfield at five times magnification. (b) A 3-panel diagram with images outlining the automated image processing and cell sizing of a whole-slide adipose tissue, accompanied by a text description of the main steps and advantages below the images. The text specifies that images were acquired at 20 times magnification.
Statistical analyses
4.4.
Spearman correlations and paired t-tests were used for the initial validation with 16 adipose tissue samples with GraphPad Prism 10.0.3 (GraphPad Software, LLC, San Diego, USA).
For the final validation of the automated method using 377 adipose tissue samples from 190 patients, the strength of association between the mean adipocyte diameters from each method was analysed using paired t-tests, linear regression, and Pearson correlations. Disagreement between the mean adipocyte diameters from each method was evaluated using Bland-Altman plots. Separate multiple linear regression analyses with interaction terms were used to determine the influence of biological sex and tertiles of manual average adipocyte diameters. In the latter analysis, the average manual adipocyte diameter measurements were centred to reduce collinearity between predictor variables. Pearson correlations were used to analyse the association between mean adipocyte diameters from each method with different markers of cardiometabolic health (BMI, WC, total Chol, HDL-Chol, LDL-Chol, TG, apoB, HOMA-IR, and VAI). Meng’s Z-test for correlated correlation coefficients was used to determine if the correlations differed significantly based on the method used. Statistical analysis was performed using RStudio® 2024.04.2 Build 764 (Posit Software, PBC, Boston, Mass. USA) with R version 4.3.3 and with GraphPad Prism® Version 10.3.1 (509) (GraphPad Software, LLC, San Diego, USA).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lindstrom M, De Cleene N, Dorsey H, et al. Global burden of cardiovascular diseases and risks collaboration, 1990–2021. J Am Coll Cardiol. 2022 Dec 20;80(25):2372–11. doi: 10.1016/j.jacc.2022.11.00136517116 · doi ↗ · pubmed ↗
- 2Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020 Aug 4;192(31):E 875–91. doi: 10.1503/cmaj.19170732753461 PMC 7828878 · doi ↗ · pubmed ↗
- 3Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013 Jan;93(1):359–404. doi: 10.1152/physrev.00033.201123303913 · doi ↗ · pubmed ↗
- 4Ye RZ, Richard G, Gévry N, et al. Fat cell size: measurement methods, pathophysiological origins, and relationships with metabolic dysregulations. Endocr Rev. 2022 Jan 12;43(1):35–60. doi: 10.1210/endrev/bnab 01834100954 PMC 8755996 · doi ↗ · pubmed ↗
- 5Laforest S, Labrecque J, Michaud A, et al. Adipocyte size as a determinant of metabolic disease and adipose tissue dysfunction. Crit Rev Clin Lab Sci. 2015;52(6):301–313. doi: 10.3109/10408363.2015.104158226292076 · doi ↗ · pubmed ↗
- 6Lessard J, Laforest S, Pelletier M, et al. Low abdominal subcutaneous preadipocyte adipogenesis is associated with visceral obesity, visceral adipocyte hypertrophy, and a dysmetabolic state. Adipocyte. 2014 Jul 1;3(3):197–205. doi: 10.4161/adip.2938525068086 PMC 4110096 · doi ↗ · pubmed ↗
- 7Chen HC, Farese RV. Determination of adipocyte size by computer image analysis. J Lipid Res. 2002 Jun;43(6):986–989. doi: 10.1016/S 0022-2275(20)30474-012032175 · doi ↗ · pubmed ↗
- 8Okamoto Y, Higashiyama H, Inoue H, et al. Quantitative image analysis in adipose tissue using an automated image analysis system: differential effects of peroxisome proliferator-activated receptor-alpha and -gamma agonist on white and brown adipose tissue morphology in AKR obese and db/db diabetic mice. Pathol Int. 2007 Jun;57(6):369–377. doi: 10.1111/j.1440-1827.2007.02109.x 17539968 · doi ↗ · pubmed ↗