Intracranial Penetrating Taser Dart Injury
Christopher Riba, Emmelyn Samones, W. Seth Dukes

TL;DR
A man suffered a taser dart injury to his skull, highlighting the potential risks of such injuries despite initial lack of severe symptoms.
Contribution
This case report highlights the rare but serious risk of intracranial injury from taser darts.
Findings
Taser dart penetrated the left frontal bone without active hemorrhage.
Patient eloped before medical intervention, risking severe consequences.
No immediate neurologic deficits were observed despite the injury.
Abstract
A healthy 52-year-old male presents to the emergency department after being tased and found to have an intracranial penetrating taser dart injury to the left frontal bone. The patient displayed somnolence with disorientation but no focal neurologic deficits on initial evaluation. Radiograph and computed tomography imaging demonstrated taser penetration into the cranial vault without clear evidence of active hemorrhage. Management with neurosurgery was planned; however, the patient eloped before intervention, a decision that could have had severe consequences. The patient later reported that the barb was removed in a nonmedical setting and denied known complications. Tasers can penetrate the skull and intracranial vault, posing risks of hemorrhage and infection. Although the patient reported no medical complications, emergency physicians remain vigilant for such sequelae during patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1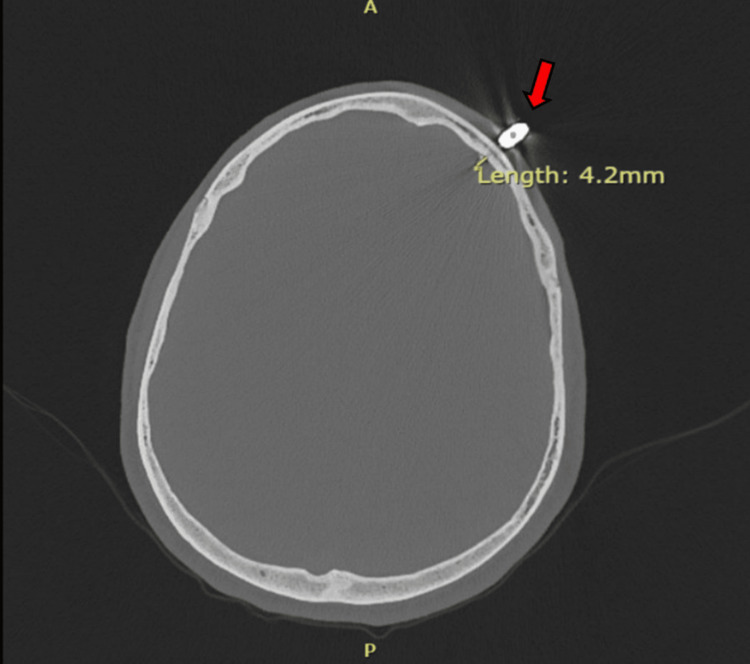 Figure 2
Figure 2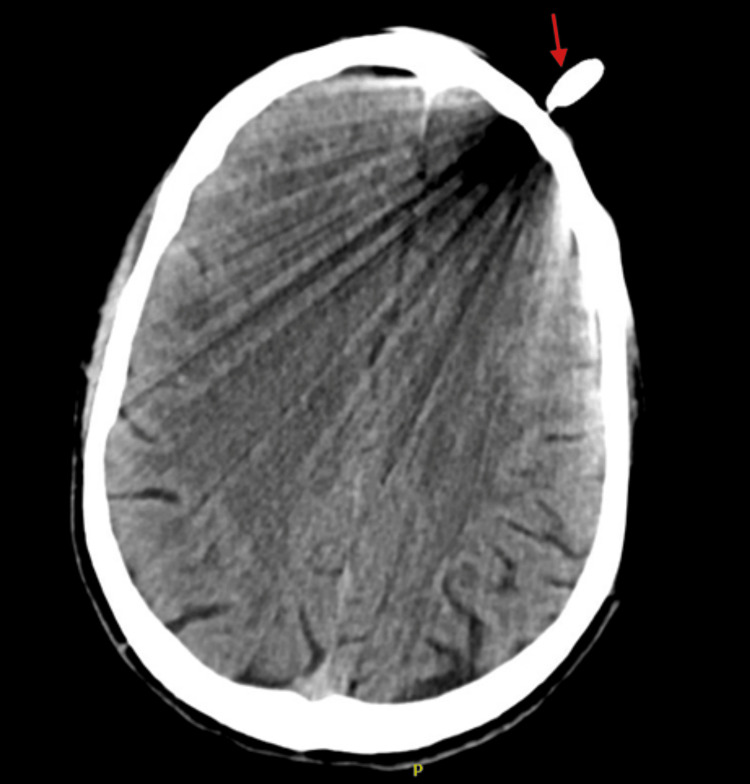 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRestraint-Related Deaths · Traumatic Ocular and Foreign Body Injuries · Child Abuse and Related Trauma
Introduction
The taser is a conducted energy weapon and is a nonlethal alternative to firearms commonly used by law enforcement. It incapacitates targets by launching two barbed projectiles that deliver numerous electrical pulses that stimulate motor neurons, inducing pain and transient paralysis. While designed to be nonlethal, injury from taser use is not unheard of, and many post-tasered individuals are taken to the emergency department to be evaluated for related injuries [1,2]. Currently, routine laboratory tests, electrocardiograms, and imaging are not recommended, with more extensive testing being used based on case circumstances and clinical judgment [3]. In this report, we present a unique and unexpected case of a man brought to our facility after tasing and found to have an intracranial penetrating taser injury.
Case presentation
A 52-year-old male without known significant past medical history arrived by ambulance due to concern for a head injury. Per emergency medical services (EMS), the patient was involved in a foot chase with police, during which the patient was tased and apprehended. The taser barb struck the patient in the forehead and back. During evaluation by police, the patient displayed waxing and waning consciousness and was oriented only to self. At that time, the patient endorsed only drinking alcohol. Still, per EMS, a bystander at the scene with the patient reported the patient had also recently smoked methamphetamine and marijuana. Despite these circumstances, the patient was cooperative and was subsequently brought to the emergency department for further evaluation.
Upon intake, the patient’s vital signs were unremarkable; however, the physical examination revealed significantly reduced responsiveness, with orientation limited to self and year corresponding to a Glasgow Coma Scale of 13 (eye = 3, verbal = 4, motor = 6). No focal neurologic deficits were noted, and a single taser barb was identified embedded within the left side of the patient’s forehead. Removal attempts were halted appropriately due to resistance. A radiograph of the skull revealed a taser barb penetrating deep to the calvarium without other fractures noted; possible intracranial penetration was not excluded (Figure 1).
Radiograph of the skull displaying taser barb projecting over the left frontal bone
The patient, in critical condition, was subsequently trauma activated, and consults to trauma surgery and neurosurgery were placed. According to neurosurgery's recommendations, a computed tomography (CT) angiogram of the head, with and without contrast, was necessary for further characterization. Results of the imaging found that the taser bolt extended 4 millimeters intracranially, beyond the inner table of the cranial vault (Figures 2, 3).
Computed tomography angiogram of the head with and without contrast displaying metallic foreign body embedded within the left frontal cranium (red arrow) and extending 4 millimeters intracranially, beyond the inner table
Computed tomography angiogram of the head with and without contrast with brain displaying metallic foreign body embedded within the left frontal cranium (red arrow) with significant beam artifacts
There was no evidence of extra-axial contrast extravasation, suggesting that an acute hemorrhage was unlikely to have occurred. However, the beam artifact from the metallic dart limited the detection of subtle hemorrhage. Given these findings, neurosurgery recommended admission for surgical removal of the barb, with intravenous ceftriaxone administered for infection prophylaxis. The patient eloped from the emergency department before these interventions were performed, and all attempts to contact the patient at that time were unsuccessful.
One year after these events, the patient was successfully contacted and provided information about what occurred following his elopement from the emergency department. The patient reported that several hours after he left, he met with several people, all of whom attempted to remove the barb. Ultimately, one individual was able to rip the barb free using a pair of pliers but found that the tip of the barb appeared to be missing. The patient denied subsequent healthcare visits for fevers, headaches, altered mentation, neck stiffness, or other symptoms of infection or hemorrhage. He denied recurrent headaches since this incident and stated that the only remaining evidence of his injury is a small, dense subdermal "bead" that is palpable over his left forehead. The patient believes the “bead” is a small piece of metal that remains in his forehead.
Discussion
This case underscores the rarity of a complication of taser use: skull penetration by a bolt with intrusion into the cranial cavity. It illustrates a scenario where no medical intervention was undertaken, yet the patient survived without reported complications. The taser device administers its incapacitating electrical current through two metal barbed projectiles, each nine millimeters in length. These are launched via travel distances, the travel of roughly 7-11 meters at a velocity of 250 feet per second [1,2]. The force with which these barbs are launched is designed to allow secure penetration of the clothing and epidermis, enabling continual metal contact while administering the electrical impulses. While not intended, the produced forces have been reported to break bones and occasionally injure deeper structures [4,5]. Research using human skulls has demonstrated that it is theoretically possible for taser barbs to fracture and even pierce the human cranium [6]. However, this case illustrates a rare real-world instance of this occurring.
It is imperative that patients who present after being tased are initially evaluated and resuscitated as needed using the standard advanced trauma life support and advanced cardiac life support. If there is any difficulty removing the barb, it is recommended that all attempts to remove the taser barb be halted until radiograph or CT imaging is obtained to evaluate for penetrance into other structures, such as bone [3,7-9]. Should this complication be identified, it is important to contact surgical specialists early, as retained metallic fragments in the cranium can result in traumatic brain injury, infection, and seizures [10,11]. This case report supports this practice and demonstrates that while taser darts are not intended to produce forces capable of serious injuries, they can produce sufficient energy to penetrate even the cranial vault. All emergency medicine physicians should be mindful of this possible complication while evaluating their patients.
Conclusions
This case demonstrates that tasers can produce sufficient force to pierce through the skull and penetrate the vault. While the patient reported no medical complications, the risks of this injury include significant intracranial hemorrhage and infection. For this reason, emergency medicine physicians should be cognizant of this possible complication of taser use during evaluation and have a system-based response prepared that includes protocolized imaging and specialist consultation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Physiology and pathology of TASER electronic control devices J Forensic Leg Med Kroll MW 1731771620091932907110.1016/j.jflm.2008.12.012 · doi ↗ · pubmed ↗
- 2TASER 10 - Axon Axon.com 7 2024 2024102024 http://Axon.com
- 3The Taser weapon: a new emergency medicine problem Ann Emerg Med Koscove EM 12051208141985406199410.1016/s 0196-0644(85)81030-1 · doi ↗ · pubmed ↗
- 4A brain penetration after Taser injury: controversies regarding Taser gun safety Forensic Sci Int Le Blanc-Louvry I Gricourt C TouréE Papin F Proust B 011221201210.1016/j.forsciint.2012.03.02722521367 · doi ↗ · pubmed ↗
- 5Intracranial taser dart penetration: literature review and surgical management J Surg Case Rep Kaloostian P Tran H 102012201210.1093/jscr/2012.6.10PMC 386218924960679 · doi ↗ · pubmed ↗
- 6Penetration depths of conducted electrical weapon probes into human skull phantoms Am J Forensic Med Pathol Bolliger SA Gort S Kaelin B Barrera V Thali MJ Martinez RM 1021074020193086496110.1097/PAF.0000000000000471 · doi ↗ · pubmed ↗
- 7Intracranial penetration of a TASER dart Am J Emerg Med Rehman TU Yonas H Marinaro J 3425200710.1016/j.ajem.2006.12.01717606107 · doi ↗ · pubmed ↗
- 8Taser and Taser associated injuries: a case series Am Surg Mangus BE Shen LY Helmer SD Maher J Smith RS 862865742008 https://pubmed.ncbi.nlm.nih.gov/18807679/18807679 · pubmed ↗