Giant Tubular Adenoma of the Breast in an Adolescent: Diagnostic Challenges and Literature Review
Monica Mishra, Seetu Palo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
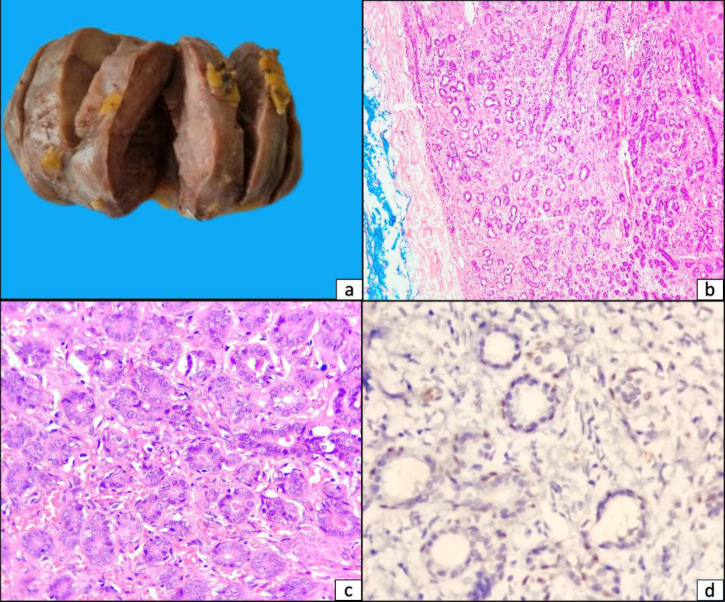 Figure 1
Figure 1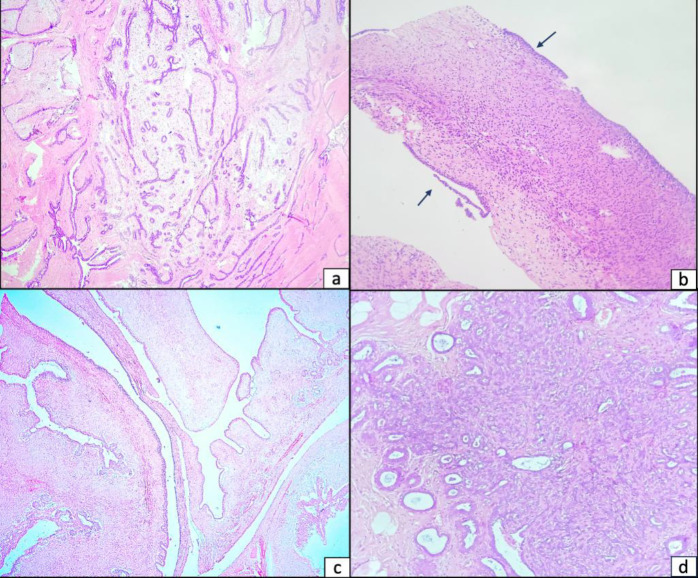 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Breast Cancer Treatment Studies · Cancer and Skin Lesions
**Dear Editor, **
Tubular adenomas are rare, comprising 0.13% to 1.7% of all benign breast neoplasms (1). While the tumor size varies between 1 cm and 7.5 cm, it seldom surpasses 5 cm, with only a very few reports of ‘giant tubular adenoma’ are on the record. We present a case of giant tubular adenoma in a young female along with a brief discussion on differential diagnoses and diagnostic difficulties in differentiating them from other fibroepithelial and benign proliferative breast lesions. This case represents the third-largest giant tubular adenoma documented in an adolescent till date, with a size of 12×10×8 cm and adds to the growing but still limited body of literature in this regard. Additionally, this report consolidates previously scattered data by including a comparative summary of clinicopathological attributes of all published giant tubular adenoma cases [Table 1] (2-10).
A 17-year-old female presented with gradually enlarging, non-tender lump in the right breast for over two years. Upon examination, a mobile, firm lump measuring 12×10 cm was noted. There was no axillary lymphadenopathy. Ultrasound revealed a well-defined, solid, hypoechoic lesion with no vascularity (BIRADS-III, likely fibroadenoma). Fine needle aspiration cytology was also suggestive of fibroadenoma. Lumpectomy was performed. Grossly, the mass was homogenously solid, measuring 12×10x8 cm and weighing 400 grams. Microscopy revealed tubular adenoma with closely arranged uniform glandular structures (with preserved outer myoepithelial cell layer) in scant fibrous stroma, without atypia or malignancy [Figure 1]. Post-operative period was uneventful.
Giant tubular adenomas of the breast present a diagnostic dilemma primarily due to their clinical and radiological resemblance to other breast lesions, particularly fibroadenomas and phyllodes tumors. Tubular adenomas appear similar to fibroadenomas on mammography and ultrasound, that is, as solid, well-delineated, hypoechoic masses (1,11). In some instances, they can mimic malignant masses with microcalcifications, posing diagnostic dilemma (12). In such cases, a core biopsy under image guidance is helpful in pre-operative diagnosis. Microscopically, while fibroadenomas often contain a mix of epithelial and stromal components [Figure 2a], tubular adenomas are composed of closely packed, uniform tubules with minimal stroma. Fine needle aspiration cytology cannot reliably distinguish tubular adenoma from fibroadenoma due to overlapping cytomorphological features as typified by our case as well. Sengupta et al analyzed 33 cases of tubular adenoma of the breast, wherein cytology confirmed the diagnosis in only 2 cases, while radiological evaluation failed to correctly identify any cases (12). Phyllodes tumors, especially benign or borderline forms, may mimic tubular adenomas both clinically and radiologically, as seen in the provisional diagnosis of the current case. Unlike tubular adenomas, phyllodes tumors exhibit predominance of stromal component with increased stromal cellularity [Figure 2b,c]. Clinically, phyllodes tumors carry a risk of recurrence and potential for malignant transformation, necessitating their distinction from tubular adenomas, which are benign at large.
While other benign lesions—such as lactating adenoma, ductal adenoma, nipple adenoma, microglandular adenosis, tubular adenosis and sclerosing adenosis —may enter the differential diagnosis, these are less frequently confused with giant tubular adenomas and were not prominent considerations in this case (2,11). Lactating adenomas, which share similarities with tubular adenomas under different physiological conditions, can be distinguished by the presence of prominent cytoplasmic vacuoles in the tubule-lining epithelium and abundant luminal secretions indicative of lactational changes. Microglandular adenosis is characterized by the proliferation of small, round tubules lined by a single layer of epithelial cells. This distinguishes it from tubular adenoma, as immunohistochemistry confirms the absence of myoepithelial cells in microglandular adenosis. Sclerosing adenosis can resemble tubular adenoma in morphology but typically features a more abundant and sclerosed stromal component, glandular distortion and absence of capsule [Figure 2d].
The only malignant lesion that closely resembles tubular adenoma is tubular carcinoma, which may appear deceptively benign histologically. Tubular carcinoma is characterized by stellate infiltrative growth pattern and absence of outer myoepithelial cell layer in the tubules (13). In diagnostically challenging cases, immunohistochemical staining for myoepithelial markers such as p63 and calponin can aid in distinguishing tubular adenoma from tubular carcinoma.
The impact of giant tubular adenomas on patient outcomes is generally positive, given the benign nature of the condition, but requires careful surgical planning to ensure satisfactory cosmetic results owing to large size. Although malignant transformation of tubular adenoma has been documented in four reported cases, the risk of carcinoma remains low (14).
To conclude, giant tubular adenoma of the breast represents an extremely rare clinical entity, posing diagnostic challenges. Given its clinical and radiological resemblance to other fibroepithelial lesions—such as fibroadenoma and phyllodes tumor—it should be included in the differential diagnosis of large, well-circumscribed, palpable breast masses in young females. Imaging modalities such as ultrasound and fine needle aspiration cytology often lack sufficient specificity to reliably differentiate these entities due to overlapping features. Hence, core needle biopsy is preferred for establishing a definitive preoperative diagnosis for guiding appropriate surgical intervention, achieving favourable cosmetic outcomes, and avoiding unnecessary overtreatment. This case highlights the importance of histopathological confirmation for large breast masses to prevent misdiagnosis. Greater clinical awareness of this entity can aid in timely diagnosis and tailored management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodrigues RA Azevedo CLAP Djahjah MCR Pereira TSS Tubular adenoma of the breast: Radiological and ultrasound findings Radiol Bras 20185134123036966910.1590/0100-3984.2017.0012 PMC 6198833 · doi ↗ · pubmed ↗
- 2Efared B SidibéIS Abdoulaziz S Hammas N Chbani L El Fatemi H Tubular Adenoma of the Breast: A Clinicopathologic Study of a Series of 9 Cases Clin Med Insights Pathol 20181111795557187574992944978010.1177/1179555718757499 PMC 5808954 · doi ↗ · pubmed ↗
- 3Düşünceli F Manukyan MN Midi A Deveci U Yener N Giant Tubular Adenoma of the Breast: A Rare Entity The Breast Journal 20121879802209850610.1111/j.1524-4741.2011.01186.x · doi ↗ · pubmed ↗
- 4Huang Y Zhang H Zhou Q Ling L Wang S Giant tubular adenoma of the accessory breast in the anterior chest wall occurred in a pregnant woman Diagn Pathol 20154106010.1186/s 13000-015-0286-0PMC 445591526040320 · doi ↗ · pubmed ↗
- 5Kalipatnapu S Samuel V Johnson M Perookavil Daniel KA Case Report of a Giant Tubular Adenoma With a Concurrent Fibroadenoma of the Breast World J Oncol 2015650232898335510.14740/wjon 954e PMC 5624680 · doi ↗ · pubmed ↗
- 6Miller MC Johnson P Kim S Choi L Tubular adenomas of the breast: a rare diagnosis BMJ Case Rep 20182018 bcr 2018224631 10.1136/bcr-2018-224631 PMC 611935630150335 · doi ↗ · pubmed ↗
- 7Mazingi D Mbanje C Jakanani G Muguti GI Mandizvidza V Bopoto S Maffucci's syndrome in association with giant tubular adenoma of the breast: Case report and literature review Int J Surg Case Rep 201963147523158532610.1016/j.ijscr.2019.09.012PMC 6796655 · doi ↗ · pubmed ↗
- 8Chehab J Montes H Zabrano M Giant tubular adenoma of the breast, a rare bening pathology: A case report Rev Oncol Ecu 2022321228