Epidemiology, Characteristics, and Treatment Outcomes of Mycoplasma pneumoniae Pneumonia in Hospitalized Adults: A 5-Year Retrospective Cohort Study
Karl Hagman, Anna C Nilsson, Magnus Hedenstierna, Johan Ursing

TL;DR
This study analyzed 747 hospitalized adults with Mycoplasma pneumoniae pneumonia in Sweden, finding tetracyclines were linked to better outcomes than other antibiotics.
Contribution
The study identifies tetracyclines as a potentially superior treatment for Mycoplasma pneumoniae pneumonia compared to macrolides and fluoroquinolones.
Findings
The incidence rate of Mycoplasma pneumoniae pneumonia was 8.5 cases per 100,000 person-years.
Tetracycline-treated patients had shorter hospital stays and fever duration compared to those treated with macrolides or fluoroquinolones.
Severe disease was associated with longer symptom duration at admission.
Abstract
This study aimed to describe the incidence rate, patient characteristics, treatments, and outcomes of adults hospitalized with Mycoplasma pneumoniae pneumonia. This retrospective cohort study included adults diagnosed with M pneumoniae pneumonia and admitted to emergency care hospitals in Stockholm County, Sweden, from 2013 to 2017. Patients were identified through positive M pneumoniae polymerase chain reaction and ICD-10 code J15.7 (M pneumoniae pneumonia). Medical records were reviewed manually, and population data were extracted from statistical databases. Incidence rates were calculated, and treatment outcomes were analyzed using regression models. A total of 747 adults with a median age of 42 (interquartile range [IQR], 33–55) years, of whom 55% (385/747) were male, were hospitalized with M pneumoniae pneumonia. The incidence rate was 8.5 cases per 100 000 person-years, peaking…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
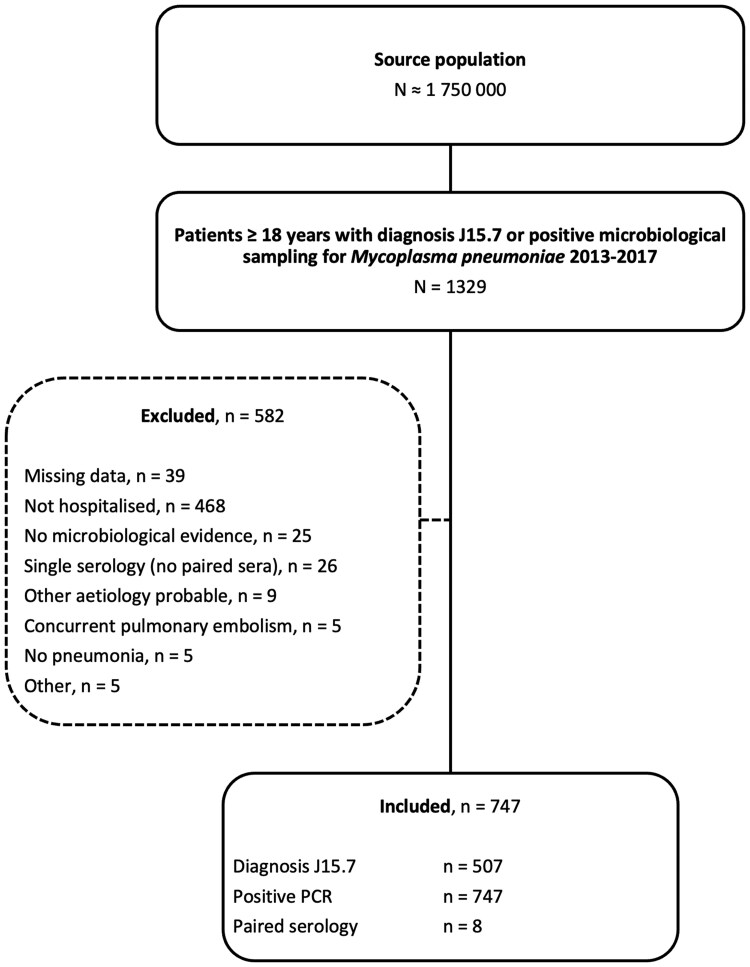 Figure 1
Figure 1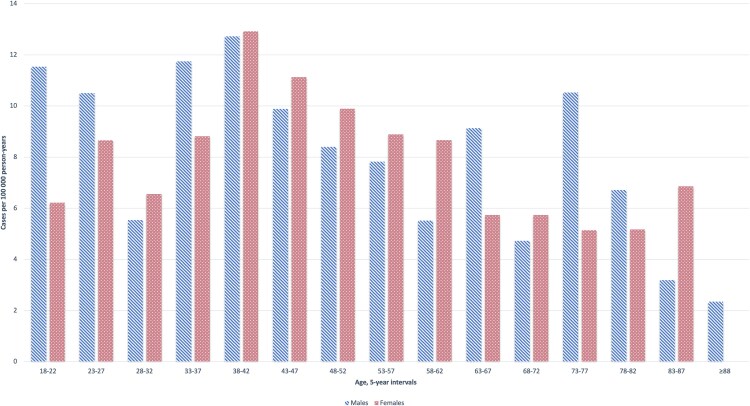 Figure 2
Figure 2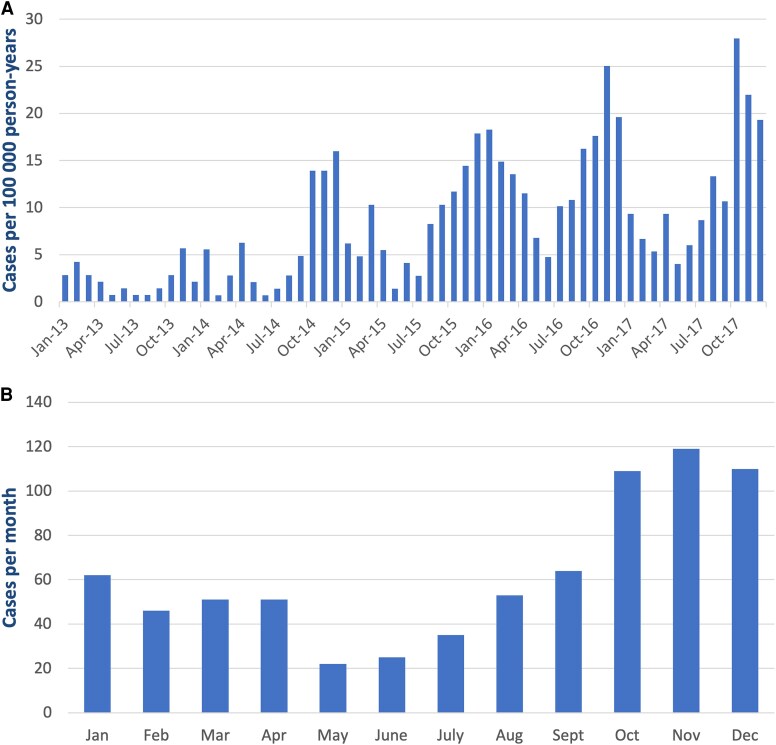 Figure 3
Figure 3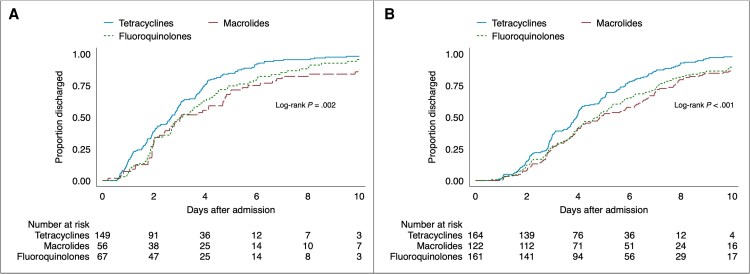 Figure 4
Figure 4| Characteristic | Full Cohort | Mild Disease | Severe Disease |
|---|---|---|---|
| Age, y, median (IQR) | 42 (33–55) | 40 (29–51) | 44 (35–57) |
| Male sex | 385/747 (52) | 124/287 (43) | 261/460 (57) |
| Smoking status | |||
| Nonsmoker | 379/524 (72) | 135/177 (76) | 244/347 (70) |
| Current smoker | 54/524 (10) | 16/177 (9) | 38/347 (11) |
| Previous smoker | 91/524 (17) | 26/177 (15) | 65/347 (19) |
| Comorbidities | |||
| No comorbidity | 420/747 (56) | 179/287 (59) | 250/460 (54) |
| COPD | 13/747 (2) | 3/287 (1) | 10/460 (2) |
| Asthma | 71/747 (10) | 28/287 (10) | 43/460 (9) |
| Other pulmonary disease | 13/747 (2) | 9/287 (3) | 4/460 (1) |
| Cerebrovascular disease | 16/747 (2) | 7/287 (2) | 9/460 (2) |
| Congestive heart failure | 24/747 (3) | 12/287 (4) | 12/460 (3) |
| Liver disease | 5/747 (1) | 4/287 (1) | 1/460 (0) |
| Chronic kidney disease | 19/747 (3) | 10/287 (3) | 9/460 (2) |
| Neoplastic disease | 31/747 (4) | 12/287 (4) | 19/460 (4) |
| Immunosuppression | 40/747 (5) | 17/287 (6) | 23/460 (5) |
| BMI, kg/m2, median (IQR) | 25.5 (23–29) | 24.7 (22–27.7) | 26.1 (23.6–29.7) |
| <18.5 | 12/547 (2) | 7/217 (3) | 5/330 (2) |
| 18.5–24.9 | 227/547 (42) | 108/217 (50) | 119/330 (36) |
| 25–30 | 195/547 (36) | 67/217 (31) | 128/330 (39) |
| >30 | 113/547 (21) | 35/217 (16) | 78/330 (24) |
| Variable | Full Cohort (n = 747) | Mild Disease | Severe Disease |
|---|---|---|---|
| Patient history | |||
| Symptom duration, d | 7 (5–10) | 6 (4–10) | 8 (6–10) |
| Cough | 708/747 (95) | 265/287 (92) | 443/460 (96) |
| Fever | 215/233 (92) | 69/74 (93) | 146/159 (92) |
| Dyspnea | 402/747 (54) | 100/287 (35) | 302/460 (66) |
| Fatigue | 365/747 (49) | 150/287 (52) | 215/460 (47) |
| Productive cough | 310/747 (42) | 108/287 (38) | 202/460 (44) |
| Headache | 140/747 (19) | 75/287 (26) | 65/460 (14) |
| Gastrointestinal symptoms | 46/247 (19) | 24/82 (29) | 22/165 (13) |
| Myalgia/arthralgia | 126/747 (17) | 53/287 (18) | 73/460 (16) |
| Chest pain | 86/747 (12) | 34/287 (12) | 52/460 (11) |
| Sore throat | 63/747 (8) | 26/287 (9) | 37/460 (8) |
| Antibiotic treatment prior to admission | 442/747 (59) | 143/287 (50) | 299/460 (65) |
| >1 antibiotic prior to admission | 60/747 (8) | 25/287 (9) | 35/460 (8) |
| Effective antibiotic prior to admission | 31/747 (4) | 18/287 (6) | 13/460 (3) |
| Findings at clinical examination | |||
| Altered mental status (GCS score <15) | 19/712 (3) | 3/270 (1) | 16/442 (4) |
| Body temperature, °C | 38.7 (38.0–39.4) | 38.7 (38.0–39.4) | 38.6 (38.0–39.3) |
| Fever (≥38°C) | 576/736 (78) | 219/279 (78) | 357/457 (78) |
| Heart rate, beats/min | 104 (93–115) | 102 (90–114) | 106 (94–115) |
| Tachycardia (heart rate >100 beats/min) | 466/732 (64) | 156/276 (57) | 310/456 (68) |
| Systolic BP, mm Hg | 116 (106–127) | 114 (105–123) | 118 (107–129) |
| Diastolic BP, mm Hg | 66 (60–73) | 66 (60–72) | 66 (60–74) |
| Hypotension (systolic BP <90 mm Hg) | 16/735 (2) | 8/278 (3) | 8/457 (2) |
| Respiratory rate, breaths/min | 24 (20–28) | 21 (18–24) | 26 (22–30) |
| Respiratory rate ≥30 breaths/min | 164/729 (23) | 25/277 (9) | 139/452 (31) |
| Hypoxemia (SpO2 <93% or oxygen treatment) | 522/740 (71) | 62/280 (22) | 460/460 (100) |
| Estimated PaO2/FiO2 | 286 (252–324) | 343 (324–367) | 262 (224–283) |
| Extrapulmonary manifestation | 30/747 (4) | 16/287 (6) | 14/460 (3) |
| Laboratory and radiology investigatory results | |||
| Lactate, mmol/L | 1.1 (0.8–1.4) | 1.1 (0.9–1.4) | 1.1 (0.8–1.4) |
| Lactate ≥2 mmol/L | 50/385 (13) | 17/110 (15) | 33/275 (12) |
| C-reactive protein, mg/L | 170 (105–246) | 147 (95–218) | 190 (114–259) |
| Leukocyte count, ×109/L | 9.7 (7.6–12.3) | 8.7 (6.7–10.9) | 10.2 (8.2–13.2) |
| Platelet count, ×109/L | 279 (209–374) | 243 (195–318) | 298 (222–386) |
| Creatinine, µmol/L | 72 (58–88) | 71 (57–88) | 72 (59–88) |
| Lactate dehydrogenase, µkat/L | 4.0 (3.4–5.8) | 3.5 (3.0–3.9) | 4.8 (3.7–6.4) |
| Infiltrates on X-ray or CT scan | 738/745 (99) | 284/287 (99) | 454/458 (99) |
| Bilateral pneumonia on X-ray or CT scan | 362/744 (49) | 92/286 (32) | 270/458 (59) |
| Pleural effusion on X-ray or CT scan | 153/744 (21) | 57/286 (20) | 96/458 (21) |
| Coinfection/colonization | 45/747 (6) | 17/287 (6) | 28/460 (6) |
| | 29.1 (22.6–34.5) | 30.3 (23.4–35.0) | 28.3 (22.4–33.9) |
| Risk scoring | |||
| PSI points | 53 (39–73) | 43 (31–58) | 61 (46–79) |
| PSI risk class I | 149/747 (20) | 112/287 (39) | 37/460 (8) |
| PSI risk class II | 391/747 (52) | 132/287 (46) | 259/460 (56) |
| PSI risk class III | 114/747 (15) | 25/287 (9) | 89/460 (19) |
| PSI risk class IV | 77/747 (10) | 15/287 (5) | 62/460 (13) |
| PSI risk class V | 16/747 (2) | 3/287 (1) | 13/460 (3) |
| Variable | Full Cohort (n = 747) | Mild Disease | Severe Disease |
|---|---|---|---|
| Days from admission to effective antibiotics | 0.7 (0–2.0) | 0.8 (0–2.0) | 0.7 (0–1.9) |
| Initial effective antibiotic | 719/747 (96) | 272/287 (95) | 447/460 (97) |
| Tetracyclines | 313/719 (44) | 149/272 (55) | 164/447 (37) |
| Macrolides | 178/719 (25) | 56/272 (21) | 122/447 (27) |
| Fluoroquinolones | 228/719 (32) | 67/272 (25) | 161/447 (36) |
| Duration of effective antibiotics, d | 8 (7–10) | 8 (7–10) | 8 (7–10) |
| Corticosteroid treatment | 176/747 (24) | 35/287 (12) | 141/460 (31) |
| Corticosteroid dose, mg | 15 (9–20) | 12 (6–19) | 15 (9–20) |
| Duration of corticosteroid treatment, d | 5 (3–6) | 5 (2–5) | 5 (3–7) |
| Duration of fever, d | 2 (1–3) | 1 (1–3) | 2 (1–3) |
| ICU care | 42/747 (6) | 5/287 (2) | 37/460 (8) |
| Duration of ICU care, d | 2 (1–5) | 1 (1–1) | 3 (1–5) |
| In-hospital mortality | 3/747 (0.4) | 0/287 (0) | 3/460 (1) |
| Length of stay, d | 4 (2–6) | 3 (2–5) | 4 (3–7) |
- —Sigurd and Elsa Golje Memorial Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Respiratory viral infections research · Bacterial Infections and Vaccines
Understanding the epidemiological characteristics of Mycoplasma pneumoniae pneumonia is vital for informed diagnostic decisions and optimized treatment strategies, particularly given its recent epidemic reemergence after several years of absence [1]. Mycoplasma pneumoniae infections occurs both endemically and with epidemic peaks approximately every 4 years [2]. A meta-analysis of etiological pneumonia studies in both outpatients and inpatients reported that M pneumoniae accounts for 18% (95% confidence interval [CI], 9%–26%) of cases, with significant heterogeneity due to the infection's epidemiological nature [3]. Additionally, in studies from the United States, M pneumoniae was identified as the most commonly detected bacterial pathogen in children hospitalized with community-acquired pneumonia (CAP) and the second most common in adults [4, 5]. Mycoplasma pneumoniae was found in 2% (43/2272) of adults hospitalized with CAP, corresponding to an incidence rate of 5 cases (95% CI, 4–7) per 100 000 person-years (PY) [4]. Adults with M pneumoniae pneumonia were younger, had fewer comorbidities, and experienced better outcomes compared to CAP of other etiologies [6].
Mycoplasma pneumoniae infections were traditionally diagnosed using serological methods. However, faster and more accurate nucleic acid amplification test (NAAT)–based diagnostics have been introduced in recent decades and are now the most prevalent method [7, 8]. It remains unclear whether the increasing use of NAAT methods for diagnostics will alter our understanding of the epidemiology and patient characteristics of M pneumoniae infections.
Macrolide antibiotics are considered first-line treatment for M pneumoniae infections in many countries due to their low minimum inhibitory concentrations and good tolerability [9]. However, the efficacy of macrolide treatment has been compromised by the increasing prevalence of macrolide-resistant M pneumoniae [10]. Other commonly used classes of antibiotics include tetracyclines and fluoroquinolones. Although there are few head-to-head comparisons, a recent meta-analysis found no significant differences in effectiveness among these antibiotic classes [11]. Treatments such as β-lactam antibiotics are ineffective for M pneumoniae due to its lack of cell wall [12]. Adjunctive corticosteroid treatment of adults hospitalized with M pneumoniae pneumonia was recently reported to correlate with shorter fever duration, but not with shorter time to regression of hypoxemia or length of stay [13].
The aim of this study was to describe the incidence rate, patient characteristics, treatments, and outcomes of adults hospitalized with M pneumoniae pneumonia over a 5-year period after the introduction of NAAT-based diagnostic testing.
METHODS
Study Design, Setting, and Population
This retrospective cohort study included adults (≥18 years of age) with pneumonia caused by M pneumoniae and hospitalized at any of the 7 emergency care hospitals in Stockholm County, Sweden, during 2013 to 2017. The region represents a total source population of about 1.75 million adult inhabitants.
Study subjects were identified by positive M pneumoniae microbiological sampling (polymerase chain reaction [PCR] from airway samples or paired sera) taken at the study hospitals and by searching medical records for the International Classification of Diseases, 10th Revision (ICD-10) code J15.7 (M pneumoniae pneumonia). Airway samples were analyzed at 2 accredited regional clinical microbiology laboratories using multiplex in-house assays based on previously described primers and probes [14]. From 2014, 1 of the laboratories changed to the multiplex assay Anyplex Ⅱ RB5 Detection (Seegene, Seoul, South Korea). Medical records were manually screened by a study physician to determine if patients were eligible for inclusion, and relevant data were extracted. Patients were not included if there was significant missing data, they were not hospitalized, there was no microbiological evidence of M pneumoniae infection (lack of positive PCR or paired sera), there was another more probable etiology for their hospitalization, and if there was no evidence of pneumonia (lack of radiological or clinical signs).
Estimated partial pressure of oxygen in arterial blood (PaO_2_)/fraction of inspired oxygen (FiO_2_) at admission was calculated from peripheral oxygen saturation (SpO_2_)/FiO_2_ as described elsewhere [15]. Included patients were categorized as having mild (estimated PaO_2_/FiO_2_ >300) or severe (estimated PaO_2_/FiO_2_ ≤300) disease at admission. Effective antibiotic treatment was defined as any antibiotics from the fluoroquinolone, macrolide, or tetracycline groups.
Statistical Analysis
Continuous variables were presented as medians (interquartile range [IQR]) and categorical variables as numbers (percentage). Differences between groups were analyzed using the Wilcoxon rank-sum test or Kruskal-Wallis test for continuous variables and Fisher exact test or χ^2^ test for categorical variables. The Spearman rank correlation coefficient was calculated for symptom duration and estimated PaO_2_/FiO_2_.
Population denominator demographic data including number of inhabitants in the region stratified by age and sex for all respective years of the study period were extracted from Statistics Sweden's Statistical Database for calculation of incidence rates. Data on the total number of bacterial pneumonia diagnoses (ICD-10 codes J13–J16 and J18) in hospitalized patients during the study period were extracted from the Swedish National Board of Health and Welfare's National Patient Register.
Median regression models were fitted to investigate the correlation between class of antibiotic treatment during hospitalization, length of stay, and fever duration. Potential confounders (age, sex, estimated PaO_2_/FiO_2_, symptom duration, corticosteroid treatment, and time from admission to effective antibiotics) were included in multivariable analyses. The model allowed for clustering of patients in regards to the hospital they were admitted to. Patients who died or did not receive any effective treatment during hospitalization were excluded from this analysis. Sensitivity analyses were performed including only patients who did not switch to another antibiotic class during hospitalization. Kaplan-Meier curves stratified by disease severity were constructed to visually describe time to discharge for different classes of antibiotics. The log-rank test was used to evaluate the equality of the survivor function across groups.
A P value <.05 was considered significant. Statistical analyses were performed using STATA-SE version 18.0 software (StataCorp LLC, College Station, Texas, USA).
Patient Consent Statement
The Regional Ethical Review Board in Stockholm, Sweden, approved of the study (registration number 2018/797-31). Informed consent was waived due to the retrospective nature of the study.
RESULTS
Baseline Characteristics
A total of 747 patients were included in the cohort (Figure 1), with 62% (460/747) classified as having severe disease (estimated PaO_2_/FiO_2_ ≤300) at admission. Included patients had a positive M pneumoniae PCR from nasopharyngeal (46% [343/747]), oropharyngeal (31% [232/747]), sputum (21% [158/747]), and bronchoalveolar lavage sampling (1% [10/747]). Four patients (0.5%) had unknown localization of sampling. Serology was infrequently used and only 8 patients (1%) had a significant titer increase in paired sera, all of whom were also PCR positive. Baseline characteristics are summarized in Table 1 and Supplementary Table 1. The median age of the cohort was 42 years (interquartile range [IQR], 33–55 years), spanning from 18 to 90 years, and 52% (285/747) were male. A majority (56% [420/747]) of the patients had no comorbidities. Patients presenting with severe disease were significantly older (median age, 44 years [IQR, 35–57 years] vs 40 years [IQR, 29–51 years]; P < .001), more likely to be male (57% [261/460] vs 43% [124/287]; P < .001), and had a higher median body mass index (26 kg/m^2^ [IQR, 24–30 kg/m^2^] vs 25 kg/m^2^ [IQR, 22–28 kg/m^2^]; P < .001) compared to those with mild disease.
Flowchart of study population. Abbreviation: PCR, polymerase chain reaction.
Forty-three patients (6%) were found to have an alternative airway pathogen. The most common pathogens were Haemophilus influenzae (10 cases), Streptococcus pneumoniae (8 cases), and Moraxella catarrhalis (8 cases). Additionally, 11 patients had a viral coinfection including rhinovirus (5 cases), coronavirus (3 cases), and 1 patient each with respiratory syncytial virus, adenovirus, and influenza A virus.
Incidence
In Stockholm County, Sweden, the registered adult population increased from 1 697 119 inhabitants in 2013, to 1 802 149 inhabitants in 2017. During this period, the incidence rate of M pneumoniae pneumonia in adults needing hospitalization was 8.5 cases (95% CI, 7.9–9.2) per 100 000 PY. The incidence rate was 8.9 cases (95% CI, 8.1–9.9) per 100 000 PY for men and 8.2 cases (95% CI, 7.4–9.1) per 100 000 PY for women (P = .23). The incidence rates by sex and age are presented in Figure 2. The annual incidence rate varied (P < .001) from 2.3 cases (95% CI, 1.6–3.1) per 100 000 PY in 2013 to 14.1 cases (95% CI, 12.4–16.0) per 100 000 PY in 2016 (Figure 3A), with the highest cumulative monthly incidences occurring from October to December (Figure 3B).
Incidence rate (cases per 100 000 person-years) of Mycoplasma pneumoniae pneumonia requiring hospitalization in adults by age and sex in Stockholm County, Sweden, 2013–2017.
A, Incidence rate (cases per 100 000 person-years) of Mycoplasma pneumoniae pneumonia requiring hospitalization in adults per month in Stockholm County, Sweden, 2013–2017. B, Cumulative number of adults with M pneumoniae pneumonia needing hospitalization per calendar month in Stockholm County, Sweden, 2013–2017.
When comparing cases of M pneumoniae pneumonia to the total number of patients hospitalized with a diagnosis of bacterial pneumonia in Stockholm County from 2013 to 2017, the proportion was 2.2% (747/33 908). This proportion ranged from 0.6% (39/6075) in 2013 to 3.4% (250/7322) in 2016.
Clinical Presentation at Admission
Symptoms, clinical findings at examination, laboratory and radiological data, and risk scoring at admission are presented in Table 2 and Supplementary Table 2. The most commonly reported symptoms were cough (95%), fever (92%), and dyspnea (54%). Patients with severe disease had a significantly longer median symptom duration (8 days [IQR, 6–10 days]) compared to those with mild disease (6 days [IQR, 4–10 days]) (P < .001). In line with this, there was a significant but weak correlation (Spearman ρ = −0.23, P < .001) between estimated PaO_2_/FiO_2_ and symptom duration (Supplementary Figure 1), indicating that patients with longer symptom duration had lower estimated PaO_2_/FiO_2_ at admission. There was no significant difference in median estimated PaO_2_/FiO_2_ between patients admitted to different study hospitals.
Antibiotic treatments prior to admission were prescribed to 59% (442/747) of patients, and 8% (60/747) received multiple courses of antibiotics. Ineffective antibiotics were prescribed to 93% (411/442) of patients receiving treatment prior to admission, of which β-lactam antibiotics constituted 407 cases. A significantly higher proportion of patients with severe disease had received ineffective antibiotic treatment prior to admission (62% [286/460]) compared to those with mild disease (44% [125/287]) (P = .02). Median symptom duration was significantly longer (P < .001) in patients receiving antibiotics prior to admission (9 days [IQR, 7–11 days]) compared to those not receiving antibiotics prior to admission (5 days [IQR, 3–7 days]).
Extrapulmonary symptoms were reported in 30 patients (4%). Twelve patients (2%) had a skin rash, including 3 with erythema multiforme and 1 with vasculitis. Six patients (1%) had hemolytic anemia, and 5 (1%) had myocarditis/pericarditis. There was 1 patient each with iritis, conjunctivitis, Guillain–Barré syndrome, myocardial infarction, meningitis/myelitis, polyarthritis, and Stevens–Johnson syndrome. All patients with extrapulmonary infection received effective antibiotic treatment during hospitalization, and 11 of 30 (37%) received adjunctive corticosteroid treatment.
Hypoxemia (SpO_2_ <93% or receiving oxygen treatment) occurred in 71% (522/740) of patients at admission and the median respiratory rate was 24 (IQR, 20–28) breaths per minute. Bilateral infiltrates on X-ray or computed tomography scan of the thorax were reported in 49% (362/744) of patients, and 21% (153/744) had a pleural effusion. Signs of severe disease such as altered mental status (3% [19/712)], hypotension (2% [16/735]), or elevated lactate concentrations (13% [50/385]) were infrequent. In line with this, 12% (93/747) were classified as Pneumonia Severity Index (PSI) risk class IV–V.
Treatments and Outcomes
Treatments and outcomes are presented in Table 3. Twenty-eight patients (4%) did not receive any effective antibiotics either prior to or during admission. Six of these 28 patients (21%) received corticosteroid treatment. Treatment with effective antibiotics was associated with significantly longer time to fever regression (P = .003) and length of stay (P < .001), compared to those not receiving effective antibiotic treatment. There was no significant difference in estimated PaO_2_/FiO_2_ between patients receiving and not receiving effective antibiotic treatment.
Initial effective antibiotics during hospitalization were tetracyclines in 44% (313/719), macrolides in 25% (178/719), and fluoroquinolones in 32% (228/719) of patients. Patients with severe disease more often (P < .001) received treatment with macrolides and fluoroquinolones compared to those with mild disease. In line with this, median estimated PaO_2_/FiO_2_ was significantly lower in patients receiving fluoroquinolones (266 [IQR, 232–310]) as initial effective antibiotics compared to those receiving macrolides (280 [IQR, 243–310]) or tetracyclines (300 [IQR, 267–343]) (P < .001). Additionally, the choice of first-line effective treatment varied between the 7 hospitals in the region (Supplementary Table 3).
Doxycycline (313/313) was the only tetracycline used. Patients treated with macrolides received erythromycin (92% [164/178]) or azithromycin (8% [14/178]). Of those treated with fluoroquinolones, 55% (125/228) received levofloxacin, 45% (102/228) moxifloxacin, and 0.4% (1/228) ciprofloxacin.
Twenty-three percent (165/719) of patients receiving effective antibiotics switched to another antibiotic class during hospitalization. Changing to another antibiotic class was most common in patients receiving initial treatment with macrolides (39% [70/178]), followed by fluoroquinolones (31% [70/228]) and tetracyclines (8% [25/313]) (P < .001). Two-thirds (110/165) of these patients received a tetracycline as a secondary effective antibiotic. Tetracyclines were thus the most common antibiotics (57% [337/656]) for patients after discharge compared to macrolides (14% [92/656]) and fluoroquinolones (29% [187/656]).
The median length of stay was 4 days (IQR, 2–6 days) in the full cohort. Length of stay was significantly longer in patients receiving treatment with macrolides (+1.0 days [IQR, 0.9–1.2 days]; P < .001) and fluoroquinolones (+0.8 days [IQR, 0.1–1.4 days]; P = .03) as initial effective antibiotics compared to those receiving tetracyclines, in a median regression adjusted for age, sex, estimated PaO_2_/FiO_2_, symptom duration, corticosteroid treatment, and time from admission to effective antibiotics (Supplementary Table 4). Kaplan-Meier curves of length of stay in patients receiving different types of antibiotics showed a higher discharge rate in patients receiving tetracyclines with similar results both in patients with mild disease and those with severe disease at admission (Figure 4). Moreover, patients with lower estimated PaO_2_/FiO_2_, higher age, longer time from admission to effective antibiotics, and corticosteroid treatment had significantly longer median length of stay in the multivariable regression (Supplementary Table 4). Results were consistent in a sensitivity analysis including only patients who did not switch to another antibiotic class during hospitalization (data not shown).
Kaplan-Meier curves of length of stay for patients with mild (estimated partial pressure of oxygen in arterial blood [PaO2]/fraction of inspired oxygen [FiO2] >300) (A) and severe (estimated PaO2/FiO2 ≤300) (B) disease at admission receiving different types of initial effective antibiotics during hospitalization. The log-rank test evaluates the equality of the survivor function across groups.
The median duration of fever was 2 days (IQR, 1–3 days) in patients with fever at admission (n = 567). Fever duration was significantly longer (+0.3 days [IQR, 0.1–0.6 days]; P = .02) in patients receiving fluoroquinolones compared to those receiving tetracyclines, in a median regression adjusted for age, sex, estimated PaO_2_/FiO_2_, symptom duration, corticosteroid treatment, and time from admission to effective antibiotics (Supplementary Table 5). Fever duration did not differ significantly between patients receiving macrolides and tetracyclines. Patients with higher age and longer time from admission to effective antibiotics had longer fever duration, and patients with longer symptom duration had shorter median fever duration in the multivariable regression (Supplementary Table 5). Results were mostly consistent in a sensitivity analysis including only patients who did not switch to another antibiotic class during hospitalization (data not shown).
In-hospital mortality was 0.4% (3/747), and 6% (42/747) of patients were admitted to an intensive care unit (ICU). The 3 patients who died during hospitalization had significant comorbidities, including neoplasia, Down syndrome, and prior cerebrovascular lesions. Two were elderly (>80 years old) and only 1 was admitted to an ICU. All were classified as having severe disease at admission. Among patients with mild disease at admission, 2% (5/287) deteriorated during hospitalization and required ICU care.
DISCUSSION
This retrospective cohort study (N = 747) provides a comprehensive analysis of the incidence, patient characteristics, treatments, and outcomes of adults hospitalized with M pneumoniae pneumonia in a Swedish region over a 5-year period after the introduction of NAAT-based diagnostic testing. The findings highlight several aspects of M pneumoniae pneumonia, contributing to the broader understanding of its epidemiology and clinical management.
Incidence
The incidence rate of M pneumoniae pneumonia in this study was 8.5 cases per 100 000 PY, representing 2.2% of all adult patients hospitalized with pneumonia. The incidence rate and prevalence are consistent with previous reported findings where M pneumoniae contributed to 2% (43/2272) of adults hospitalized with CAP, representing an incidence rate of 5 cases (95% CI, 4–7) per 100 000 PY [4]. The notable annual variation, with a peak incidence in 2016, is in line with the known cyclical epidemic pattern of M pneumoniae infections, which typically exhibit peaks every 4 years [2]. This pattern is also consistent with previous data indicating an epidemic in Europe during the winter seasons of 2014–2015 and 2015–2016 [8]. These results underscore the importance of heightened clinical and diagnostic vigilance during epidemic periods.
Patient Characteristics and Clinical Presentation
The cohort predominantly comprised younger adults with a median age of 42 years, and a significant proportion had no comorbidities. This demographic profile is consistent with earlier studies indicating that M pneumoniae pneumonia often affects younger, healthier individuals compared to CAP of other etiologies [6, 16]. However, a relatively high proportion of older patients were included, with 14% (106/747) being 65 years or older. This age distribution is similar to previous Swedish data but differs from most other European countries, where M pneumoniae infections are infrequently diagnosed in older individuals [8]. This finding suggests that M pneumoniae infections occur in older patients and may be underdiagnosed.
A high proportion of patients had severe respiratory illness, but few had signs of systemic infection such as hypotension or elevated lactate concentrations. Patients with severe disease were older, had higher body mass index, and were more often male, suggesting that these factors may contribute to disease severity. Additionally, patients with severe disease more often received ineffective antibiotic treatment prior to admission and had longer symptom durations. This highlights the risk of delayed diagnosis and a need for improved diagnostic protocols to ensure timely and appropriate treatment.
Treatments and Outcomes
Unexpectedly, patients receiving no effective treatment during hospitalization had better outcomes. This group likely represent patients where the microbiological results were received after discharge. However, follow-up data were not available from after discharge.
Hospital discharge occurred approximately 1 day faster in patients treated with tetracyclines compared to those treated with macrolides or fluoroquinolones even after adjusting for confounders such as disease severity. The choice of first-line antibiotic treatment varied due to local traditions rather than patient disease severity across different hospitals in the region. This strengthens the findings, although residual confounding such as disease severity may still be present. These results differ from previous retrospective studies that reported no significant differences in length of stay or fever duration between these antibiotic classes [11, 17]. The prevalence of macrolide-resistant M pneumoniae in Sweden 2016–2017 was reported to be 2% (1/61), and no clinical isolates with fluoroquinolone resistance have been identified, indicating that antibiotic resistance did not affect outcomes [9, 18]. These results suggest that doxycycline is an effective first-line treatment option for adults hospitalized with M pneumoniae pneumonia.
The low in-hospital mortality rate (0.4%) and ICU admission rate (6%) reflect the generally favorable outcomes for M pneumoniae pneumonia. However, the significant morbidity associated with severe disease underscores the need for early and effective treatment.
Strengths and Limitations
The strengths of this study include the comprehensive inclusion of all diagnosed patients from a well-defined source population, detailed clinical data, and the use of reliable population denominator data from Swedish statistics databases. The retrospective design may introduce selection bias, and the reliance on medical records for data extraction could result in misclassification or incomplete data. Additionally, the study was conducted in a single geographic region, which may limit the generalizability of the findings to other settings. Despite using multivariable models to analyze the correlation of antibiotic class to outcomes, there remains a risk of residual confounding by indication, as patients treated with tetracyclines more often had mild disease. Moreover, there is a possibility of information bias in time to regression of fever as different hospitals may have had varying precision of temperature data. Future prospective studies are needed to validate these results and explore the long-term outcomes of M pneumoniae pneumonia.
CONCLUSIONS
This study of 747 adults hospitalized with M pneumoniae pneumonia provides valuable insights into the epidemiology, clinical characteristics, and management of this disease. The findings highlight the importance of timely and accurate treatment and potential benefits of doxycycline as a first-line treatment. These insights can inform clinical practice and guide future research to improve the care of patients with M pneumoniae pneumonia.
Supplementary Material
ofaf380_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meyer Sauteur PM, Beeton ML, Pereyre S, et al Mycoplasma pneumoniae: delayed re-emergence after COVID-19 pandemic restrictions. Lancet Microbe 2024; 5:e 100–1.38008103 10.1016/S 2666-5247(23)00344-0 · doi ↗ · pubmed ↗
- 2Brown RJ, Nguipdop-Djomo P, Zhao H, Stanford E, Spiller OB, Chalker VJ. Mycoplasma pneumoniae epidemiology in England and Wales: a national perspective. Front Microbiol 2016; 7:157.26909073 10.3389/fmicb.2016.00157 PMC 4754400 · doi ↗ · pubmed ↗
- 3Marchello C, Dale AP, Thai TN, Han DS, Ebell MH. Prevalence of atypical pathogens in patients with cough and community-acquired pneumonia: a meta-analysis. Ann Fam Med 2016; 14:552–66.28376442 10.1370/afm.1993 PMC 5389400 · doi ↗ · pubmed ↗
- 4Jain S, Self WH, Wunderink RG, et al Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 2015; 373:415–27.26172429 10.1056/NEJ Moa 1500245 PMC 4728150 · doi ↗ · pubmed ↗
- 5Kutty PK, Jain S, Taylor TH, et al Mycoplasma pneumoniae among children hospitalized with community-acquired pneumonia. Clin Infect Dis 2019; 68:5–12.29788037 10.1093/cid/ciy 419PMC 6552676 · doi ↗ · pubmed ↗
- 6von Baum H, Welte T, Marre R, Suttorp N, Lück C, Ewig S. Mycoplasma pneumoniae pneumonia revisited within the German Competence Network for Community-Acquired Pneumonia (CAPNETZ). BMC Infect Dis 2009; 9:62.19439072 10.1186/1471-2334-9-62PMC 2689234 · doi ↗ · pubmed ↗
- 7Nilsson AC, Björkman P, Persson K. Polymerase chain reaction is superior to serology for the diagnosis of acute Mycoplasma pneumoniae infection and reveals a high rate of persistent infection. BMC Microbiol 2008; 8:93.18547431 10.1186/1471-2180-8-93PMC 2446399 · doi ↗ · pubmed ↗
- 8Beeton ML, Zhang XS, Uldum SA, et al Mycoplasma pneumoniae infections, 11 countries in Europe and Israel, 2011 to 2016. Euro Surveill 2020; 25:1900112.31964459 10.2807/1560-7917.ES.2020.25.2.1900112 PMC 6976882 · doi ↗ · pubmed ↗