Kidney function improvement after urinary diversion for cisplatin eligibility in bladder cancer patients
Fernando Korkes, José Henrique DallAcqua Santiago, André Marantes Masciarelli Pinto, Artur da Silva Farias, Frederico Timóteo, Suelen Patricia dos Santos Martins, Sidney Glina

TL;DR
This study shows that urinary diversion can improve kidney function in bladder cancer patients, making them eligible for cisplatin chemotherapy.
Contribution
The study demonstrates that urinary diversion reverses renal impairment in bladder cancer patients, enabling cisplatin eligibility.
Findings
Mean GFR improved from 44.1 to 59.1 mL/min after urinary diversion.
75% of patients with initial GFR <50 mL/min achieved GFR >50 mL/min post-diversion.
Initial GFR was a significant predictor of GFR recovery.
Abstract
Muscle-invasive bladder cancer (MIBC) is an aggressive disease typically treated with radical cystectomy following neoadjuvant chemotherapy (NAC). However, the presence of hydronephrosis – a significant marker of advanced disease – can impair renal function, potentially precluding patients from receiving cisplatin-based NAC. The present study aimed to assess the role of urinary diversion in patients with MIBC, specifically in reversing renal function impairment and enabling eligibility for cisplatin-based therapy. A retrospective study was performed by evaluating a database of patients treated for urothelial MIBC from 2018 to 2021. Case notes were reviewed to identify patients with hydronephrosis who underwent urinary diversion. The types of urinary diversion recorded included percutaneous nephrostomy, ureteral stenting, or surgical obstruction release. Renal function was assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
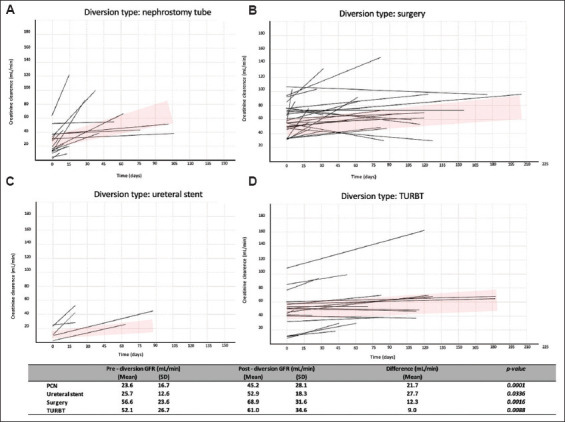 Figure 1
Figure 1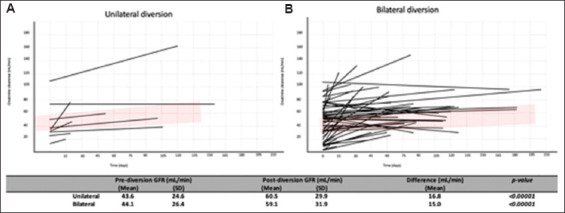 Figure 2
Figure 2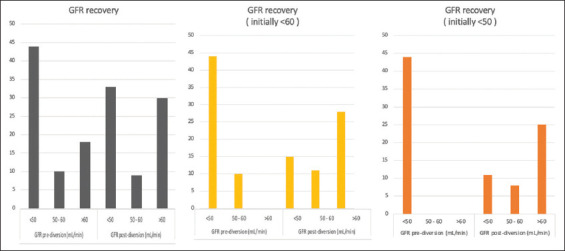 Figure 3
Figure 3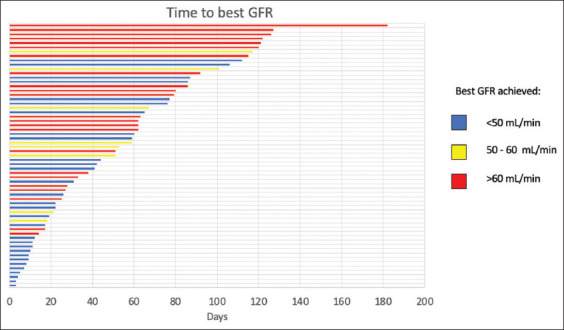 Figure 4
Figure 4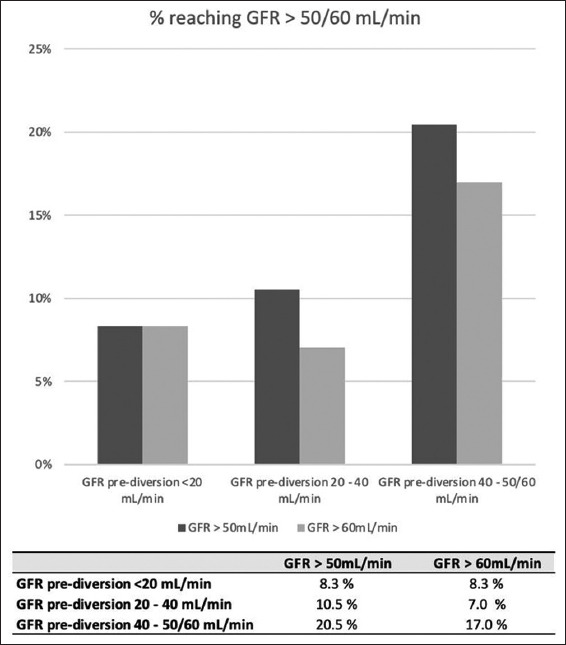 Figure 5
Figure 5| Parameter | %/range | |
|---|---|---|
| Gender | ||
| Male | 51 | 71.0 |
| Female | 21 | 29.0 |
| Ethnicity | ||
| White | 52 | 72.2 |
| Black | 13 | 18.1 |
| Brown | 7 | 9.7 |
| Hydronephrosis | ||
| Unilateral | 41 | 56.9 |
| Bilateral | 29 | 40.3 |
| Hydronephrosis right | ||
| Absent | 25 | 34.7 |
| Mild | 13 | 18.1 |
| Moderate | 17 | 23.6 |
| Severe | 17 | 23.6 |
| Hydronephrosis left | ||
| Absent | 19 | 26.4 |
| Mild | 9 | 12.5 |
| Moderate | 30 | 41.7 |
| Severe | 14 | 19.4 |
| Pre-creatinine | 2.4 | (0.5 – 12.6) |
| Pre-creatinine clearance | 44.1 | (5.1 – 113.0) |
| Post-creatinine | 1.4 | (0.5 – 4.2) |
| Post-creatinine clearance | 59.1 | (9.5 – 165.3) |
| Urinary diversion | ||
| Unilateral | 11 | 15.3 |
| Bilateral | 61 | 84.7 |
| Right kidney diversion | ||
| Ureteral stent | 5 | 6.9 |
| Nephrostomy tube | 4 | 5.6 |
| Surgical diversion | 18 | 25.0 |
| TURBT | 25 | 34.7 |
| Left kidney diversion | ||
| Ureteral stent | 4 | 5.6 |
| Nephrostomy tube | 5 | 6.9 |
| Surgical diversion | 15 | 20.8 |
| TURBT | 27 | 37.5 |
| Parameter | Multivariate regression | |
|---|---|---|
|
| ||
| Odds ratio (95% confidence interval) | ||
| Hydronephrosis | ||
| Unilateral | Reference | - |
| Bilateral | 1.22 (0.22 – 6.89) | 0.822 |
| Hydronephrosis grade | ||
| Mild | Reference | - |
| Moderate | 8.75 (0.46 – 168.02) | 0.150 |
| Severe | 9.56 (0.45 – 202.69) | 0.147 |
| GFR pre | 1.11 (1.02 – 1.21) | 0.012 |
| GFR cluster | ||
| <50 mL/min | Reference | - |
| 50 – 60 mL/min | 4.42 (0.20 – 97.66) | 0.346 |
| >60 mL/min | 2.10 (0.03 – 133.08) | 0.726 |
| Urinary diversion | ||
| Unilateral | Reference | - |
| Bilateral | 3.42 (0.22 – 52.92) | 0.379 |
| Diversion type | ||
| Ureteral stent | Reference | - |
| PCN | 0.42 (0.03 – 5.56) | 0.511 |
| Surgery | 0.06 (0.01 – 2.04) | 0.119 |
| TURBT | 0.05 (0.01 – 1.33) | 0.073 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urological Disorders and Treatments · Renal cell carcinoma treatment
1. Introduction
Muscle-invasive bladder cancer (MIBC) is an aggressive disease associated with elevated mortality rates. Radical cystectomy (RC) remains the cornerstone of treatment for these patients. There is now substantial evidence supporting the use of cisplatin-based systemic therapy before surgery for all eligible patients.1 In this context, neoadjuvant chemotherapy (NAC) has been shown to reduce the risk of mortality by up to 16% and may improve 5-year survival by up to 8%.2-4
Despite the body of evidence supporting NAC, these data have not been widely translated into the routine implementation of multimodal strategies for treating MIBC. Factors, such as increasing age, comorbidities, lower patient income, and treatment at non-academic centers have been identified as barriers to the acceptance of NAC.5 Concerns regarding the toxicity of chemotherapy, delays in the time to cystectomy, and the potential overtreatment of patients with organ-confined disease further contribute to its underuse. In addition, frail patients with MIBC may have clinical characteristics that contraindicate the use of cisplatin-based chemotherapy regimens.6
Contraindications to cisplatin-based chemotherapy include hearing loss/dysfunction, cardiac dysfunction, poor performance status, and renal insufficiency.7,8 A significant proportion of MIBC patients have impaired renal function, and when taking a creatinine clearance (CrCl) below 60 mL/min as the threshold, studies have demonstrated that approximately 40% of MIBC patients over the age of 70 may be ineligible for cisplatin-based chemotherapy.9 Multiple factors contribute to renal function impairment in this patient population, including comorbidities, age-related declines in glomerular filtration rate (GFR), and ureteral obstruction. It is important to note that one major limitation of CrCl testing is its decreasing accuracy as GFR declines, due to the increasing tubular secretion of creatinine. As a result, GFR may be overestimated in patients with renal impairment.
The incidence of ureteral obstruction and hydronephrosis in MIBC ranges from 7.2% to 54.1%.10-12 This condition typically arises from intramural or extravesical tumoral extension, tumor involvement of the ureteral orifice, or simultaneous ureteral tumors.13 The negative impact of ureteral obstruction in this cohort is multifaceted. Hydronephrosis serves as a significant marker for advanced disease and is an independent prognostic marker for adverse oncological outcomes, such as recurrence-free survival and cancer-specific survival.10 Moreover, urethral obstruction can result in renal function impairment, which may prevent patients from benefiting fully from cisplatin-based NAC.
Accurately predicting the potential for kidney function recovery after the release of urinary obstruction is crucial for both urologists and oncologists. Functional recovery can occur as early as 7 – 10 days, though it may take longer, depending on factors, such as the completeness and duration of the obstruction, as well as the function of the contralateral kidney.14,15
There is a lack of studies evaluating the impact of urinary obstruction release on kidney function, specifically in the MIBC context. The present study aimed to assess the role of urinary diversion in patients with urothelial MIBC, particularly its effect on reversing renal function impairment, and to discuss the various factors that may influence the recovery of GFR to levels meeting cisplatin eligibility.
2. Methods
2.1. Patients
A retrospective study was conducted to examine the patients treated for urothelial MIBC at our institution from 2018 to 2021. All case notes were reviewed, and patients with hydronephrosis who had undergone urinary diversion were included for further analysis. The types of urinary diversion recorded included placement of a percutaneous nephrostomy (PCN), insertion of a ureteral stent, transurethral resection of the bladder tumor (TURBT) over the ureteral orifice, or surgical obstruction release (including cutaneous ureterostomy alone or incontinent urinary diversion). The decision regarding the method of diversion was made at the discretion of the surgeon.
Data collected for analysis included demographic information, serum creatinine levels, and post-operative complications. Patients in the surgical group who underwent orthotopic diversions were excluded from further analysis. Serum creatinine was measured using kinetic colorimetric assays. GFR was determined based on CrCl, calculated from serum creatinine using the Cockcroft-Gault (CG) formula.16 We selected the CG formula as the primary tool for estimating CrCl, as it has similar efficiency to the Chronic Kidney Disease Epidemiology Collaboration equation.17
2.2. Statistical analysis
Statistical analysis was performed using STATA 14.0 (StataCorp LP, USA). Groups were compared using Pearson’s Chi-square or Fisher’s exact test. The Student’s t-test was applied for continuous variables with a normal distribution, while the Mann–Whitney U test was used for variables with a non-normal distribution. Analysis of variance was performed for multiple comparisons. A generalized linear regression model was utilized to investigate the effect of covariates on the GFR recovery. Statistical significance was defined as a p < 0.05.
2.3. Ethical approval and patient consent
All participants voluntarily provided informed consent and were aware that they could withdraw consent at any time. The study was approved by the Institutional Review Board (IRB), with approval numbers of 40836920.0.0000.0071 and 26817719.2.0000.0082.
3. Results
A total of 72 patients satisfied the criteria for having hydronephrosis secondary to MIBC that was subsequently relieved. Of these patients, 51 were male and 21 were female. The mean age of the study population was 67.5 years (range, 33 – 92 years). Demographic data are presented in Table 1.
The mean GFR before urinary diversion was 44.1 ± 26.4 mL/min (range, 5.1 – 113 mL/min), while the mean GFR after urinary diversion was 59.1 ± 31.9 mL/min (range, 9.5 – 165.3 mL/min). After urinary diversion, the mean GFR recovery was 15.0 ± 20.0 mL/min (range, 0 – 73.6 mL/min). The mean GFR recovery for different types of urinary diversion was as follows: PCN, 22 mL/min (range, 0 – 74 mL/min); ureteral stent, 27 mL/min (range, 0 – 42 mL/min); surgery, 12 mL/min (range, 0 – 58 mL/min); and TURBT, 9 mL/min (range, 0 – 52 mL/min). GFR was significantly higher after all types of diversion (Figure 1), as well as after unilateral and bilateral diversion (Figure 2).
Of the 72 patients, 44 had an initial GFR below 50 mL/min. 75% of these patients (n = 33) demonstrated an improvement in GFR to above 50 mL/min following urinary diversion. More than half of these patients (n = 25, 56%) experienced an increase in their GFR to above 60 mL/min (Figure 3). In addition, 54 patients had an initial GFR below 60 mL/min, and 51.8% (n = 28) of these patients experienced an improvement in GFR (Figure 3).
The time to achieve the best GFR varied widely. The median ± standard deviation (SD) time to reach the optimal GFR was 59 ± 33 days (range, 9 – 165 days). Thirteen patients with a baseline GFR below 50 mL/min (mean GFR ± SD = 36.8 ± 12.7 mL/min) achieved a GFR above 50 mL/min after a mean period of 61 ± 39 days (mean GFR ± SD = 70.0 ± 15.4 mL/min). When using a cutoff of GFR below 60 mL/min, 16 patients showed a significant recovery. These patients initially had a mean GFR of 46.8 ± 15.9 mL/min, and after a mean period of 78.3 ± 42 days, their GFR increased to 76.6 ± 15.7 mL/min (Figure 4).
Eleven patients could be classified as “super-recoverers.” These patients had a very low initial GFR (mean GFR ± SD = 38.5 ± 20.2 mL/min), and after a relatively short period (29 ± 18 days), their GFR increased to 82 ± 25 mL/min. Most of these patients had mild- to high-grade hydronephrosis in their renal units (13/12 units, 60%), and nearly all underwent bilateral urinary diversion (10/11, 91.1%).
Logistic regression indicated that the initial GFR was significantly associated with GFR recovery (odds ratio = 1.11, 95% confidence interval = 1.02 – 1.21, p = 0.012). For each unit increase in pre-diversion GFR, the odds of a patient becoming cisplatin-eligible increased by 11.32 (Table 2). Figure 5 summarizes the percentage of patients achieving a ClCr >50 mL/min and >60 mL/min based on initial GFR categories.
4. Discussion
MIBC is a challenging disease. NAC with cisplatin-based combination regimens lowers the risk of recurrence following RC.18 As mentioned earlier, several factors can determine cisplatin ineligibility, with a ClCr <60 mL/min being one of the primary conditions that preclude MIBC patients from benefiting from NAC. Virtually, half of the patients with MIBC are ineligible for NAC, and hydronephrosis is a significant factor associated with reduced GFR.8
Despite concerns about NAC for MIBC, such as therapeutic toxicity and potential delays to RC, robust scientific evidence indicates that the benefits of NAC outweigh the risks for eligible patients.1-4 It is essential to emphasize that urothelial carcinoma of the bladder is highly chemosensitive and generally responds well to cisplatin-based regimens.1,19 Occult metastasis at the time of diagnosis is a key reason for the poor prognosis of MIBC, with recurrence rates reaching as high as 50% after RC.18,20 The rationale for administering NAC is to increase survival by targeting micrometastatic disease at the time of diagnosis when the tumor burden is at its lowest.21
A common dilemma in the management of MIBC is whether to perform upfront RC or a urinary diversion followed by NAC. RC is a cornerstone of curative treatment for MIBC and should not be delayed for more than 12 weeks, as postponing the procedure increases mortality risk.22 Thus, it is crucial to ensure that NAC does not interfere with the patient’s ability to undergo surgery. While RC is a complex procedure with a high 90-day complication rate, it can lead to the inability to administer adequate post-operative chemotherapy in over 30% of patients.23 This scenario highlights the complexity of decision-making, where urologists and clinical oncologists must carefully consider whether performing a urinary diversion to improve renal function may enable cisplatin-ineligible patients to benefit from NAC. Therefore, appropriate patient selection for urinary diversion is of utmost importance.
Since hydronephrosis is a marker of both advanced disease and poor prognosis, it is reasonable to assume that MIBC patients with renal obstruction may benefit from the advantages of NAC. Ureteral obstruction elevates ipsilateral ureteral pressure and reduces renal blood supply, leading to a decrease in GFR and cellular and molecular abnormalities in the obstructed kidney, ultimately progressing to fibrosis.24 Upon relief of the obstruction, the renal response depends on several factors, including the patient’s age, ureteral compliance, duration of the obstruction, contralateral kidney function during the obstruction, and the degree of fibrosis.24 Notably, the duration of ureteral obstruction plays a critical role in the kidney’s regenerative potential.
The recovery period following the release of an obstruction has been widely studied in animal models.25 In rats, functional and structural recovery of a kidney obstructed for 3 – 7 days typically takes 4 – 6 weeks.25,26 In dogs, after 4 days of obstruction, there is a practically complete recovery of the GFR. However, as the obstruction persists, the recovery potential progressively declines, such that after 21 days, only 13% of the original GFR is restored.27 In humans, the exact recovery timeline is less defined. While the literature generally agrees that complete GFR recovery is possible when diversion is implemented promptly, controversy remains regarding the recovery potential for kidneys obstructed for longer periods.15,28-32 This uncertainty may stem from the difficulty in accurately assessing the degree of obstruction in humans, as well as challenges in estimating the duration of obstruction in patients diagnosed with bladder cancer.
In our own observations, there was considerable variability in recovery time among patients (Figure 4). While some patients demonstrated GFR recovery within a few days, others required several weeks for full recovery. Given that MIBC treatment is time-sensitive, the time required for GFR recovery is vital, as adequate GFR is necessary for administering NAC and proceeding with surgery. The overall median time to achieve the best GFR was 59 days, which can be considered a relatively long period in the context of this time-sensitive disease. However, we identified 11 patients with very low initial GFR (mean ± SD = 38.5 ± 20.2 mL/min) who attained a GFR of 82 ± 25 mL/min after a relatively short period following the release of obstruction. Approximately 60% of these “super-recoverers” had moderate to severe hydronephrosis, and 91.1% had undergone bilateral diversion.
To identify patients more likely to achieve GFR recovery, we performed a multivariate analysis, which revealed that the only statistically significant predictor of GFR recovery was the initial GFR (Table 2). A previous prospective study of non-oncological patients with ureteral obstruction found that several factors, such as pre-operative renographic GFR, renal perfusion, parenchymal thickness, parenchymal echogenicity, corticomedullary differentiation, reduction of the renal resistive index, and compensatory hypertrophy of the contralateral normal kidney, were associated with renal function recovery after the relief of obstruction. However, on multivariate analysis, only pre-operative GFR and renal perfusion remained statistically significant as independent factors affecting kidney functional recovery.14 Our data corroborate these findings, demonstrating that pre-operative GFR was the sole independent factor influencing renal function recovery in patients with bladder cancer and hydronephrosis. Patients with a GFR between 40 and 50 mL/min had the highest likelihood of becoming eligible for cisplatin. In contrast, kidneys with a GFR of around 10 mL/min were likely irreversibly damaged, as shown in Figure 5. Therefore, patients with such low GFR should not be considered for diversion as a strategy to improve their chances of receiving cisplatin (Figure 5).
Although we could not identify significant predictors for the time to GFR recovery, we have demonstrated that some patients can become eligible for cisplatin, and this can occur within a reasonable timeframe. Future studies that evaluate imaging techniques and attempt to establish GFR recovery nomograms may provide valuable insights. In the meantime, it is essential to note that 75% of patients who were initially ineligible for cisplatin became eligible after upper tract deobstruction, with up to 25% of these patients showing significant kidney function improvement in a relatively short period, thereby potentially benefiting from NAC. Furthermore, GFR recovery has additional positive clinical implications.
Our study has several limitations. First, its retrospective nature introduces inherent constraints. We could not estimate the duration of the obstruction, and the timing of examinations post-ureteral deobstruction was not pre-established, relying instead on clinician requests. We also lacked data on urine output and were unable to evaluate imaging examinations for all patients, as many did not have initial scans available for analysis. Nevertheless, previous studies have shown that certain imaging parameters, such as parenchymal echogenicity, corticomedullary differentiation, renal perfusion, and parenchymal thickness, do not consistently predict GFR recovery.14
This study focused on a specific population of bladder cancer patients and their demographic characteristics, with a particular emphasis on the feasibility of performing urinary diversion to improve GFR recovery and cisplatin eligibility for NAC. By highlighting this issue, we encourage the scientific community to develop tools that can predict when urinary diversion should precede RC to optimize treatment outcomes.
5. Conclusion
Some patients with upper tract obstruction secondary to MIBC can benefit from pre-operative urinary diversion, with a mean GFR recovery of 15 mg/mL following deobstruction. Patients with mildly reduced GFR are more likely to become eligible for cisplatin. The time to GFR recovery varies, typically ranging from 1 to 8 weeks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Witjes JA Bruins HM Cathomas R European association of urology guidelines on muscle-invasive and metastatic bladder cancer:Summary of the 2020 guidelines. Eur Urol. 2021;79(1):82–104. doi:10.1016/j.eururo.2020.03.05532360052 10.1016/j.eururo.2020.03.055 · doi ↗ · pubmed ↗
- 2International Collaboration of Trialists, Medical Research Council Advanced Bladder Cancer Working Party (now the National Cancer Research Institute Bladder Cancer Clinical Studies Group). European Organisation for Research and Treatment of Cancer Genito-Urinary Tract Cancer Group International phase III trial assessing neoadjuvant cisplatin, methotrexate, and vinblastine chemotherapy for muscle-invasive bladder cancer:Long-term results of the BA 06 30894 trial. J Clin Oncol. 2011;29(16):2171–2177 · doi ↗ · pubmed ↗
- 3Grossman HB Natale RB Tangen CM Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer [published correction appears in N Engl J Med 2003;349 191880]. N Engl J Med. 2003;349(9):859–866. doi:10.1056/NEJ Moa 02214812944571 10.1056/NEJ Moa 022148 · doi ↗ · pubmed ↗
- 4Hamid ARA Ridwan FR Parikesit D Widia F Mochtar CA Umbas R Meta-analysis of neoadjuvant chemotherapy compared to radical cystectomy alone in improving overall survival of muscle-invasive bladder cancer patients. BMC Urol. 2020;20(1):158. doi:10.1186/s 12894-020-00733-z 33054762 10.1186/s 12894-020-00733-z PMC 7557048 · doi ↗ · pubmed ↗
- 5Zaid HB Patel SG Stimson CJ Trends in the utilization of neoadjuvant chemotherapy in muscle-invasive bladder cancer:Results from the National Cancer Database. Urology. 2014;83(1):75–80. doi:10.1016/j.urology.2013.07.07224231210 10.1016/j.urology.2013.07.072 · doi ↗ · pubmed ↗
- 6Korkes F Editorial Comment:Factors associated with utilization of neoadjuvant chemotherapy in charlson comorbidity zero non-metastatic muscle-invasive bladder cancer patients. Int Braz J Urol. 2021;47(4):819–820. doi:10.1590/S 1677-5538. IBJU.2020.0594.133848074 10.1590/S 1677-5538.IBJU.2020.0594.1PMC 8321471 · doi ↗ · pubmed ↗
- 7Apolo AB Grossman HB Bajorin D Steinberg G Kamat AM Practical use of perioperative chemotherapy for muscle-invasive bladder cancer:Summary of session at the Society of Urologic Oncology annual meeting. Urol Oncol. 2012;30(6):772–780. doi:10.1016/j.urolonc.2012.01.01223218068 10.1016/j.urolonc.2012.01.012PMC 3524835 · doi ↗ · pubmed ↗
- 8Thompson RH Boorjian SA Kim SP Eligibility for neoadjuvant/adjuvant cisplatin-based chemotherapy among radical cystectomy patients. BJU Int. 2014;113(5b):E 17–E 21. doi:10.1111/bju.1227424006893 10.1111/bju.12274 · doi ↗ · pubmed ↗