A management of a patient with chronic thromboembolic pulmonary hypertension prior to surgical resection for lung cancer
Satoshi Isomatsu, Kenichiro Takeda, Yu Shionoya, Toshihiko Sugiura, Shizu Miyata, Shun Imai, Jun Nagata, Yu Taniguchi, Akira Naito, Rika Suda, Ayako Shigeta, Nobuhiro Tanabe, Takuji Suzuki

TL;DR
A 55-year-old woman with both CTEPH and lung cancer was successfully treated by prioritizing CTEPH management before lung cancer surgery.
Contribution
This case report presents a management strategy for coexisting CTEPH and lung cancer.
Findings
CTEPH treatment with riociguat and BPA reduced mean pulmonary artery pressure from 39 to 27 mmHg.
Lung cancer surgery was performed without significant worsening of right heart failure.
No recurrence of lung cancer was observed post-surgery.
Abstract
The basic treatment for chronic thromboembolic pulmonary hypertension (CTEPH) includes lifelong anticoagulant therapy and pulmonary endarterectomy; moreover, balloon pulmonary angioplasty (BPA) and vasodilators are also known to be effective. Surgery is the standard treatment for localized lung cancer. However, no established treatment guidelines exist for cases of coexisting CTEPH and lung cancer. The patient was a 55-year-old woman who experienced dyspnea on exertion. She was diagnosed with non-small cell lung cancer, and surgery was scheduled; however, she was also diagnosed with CTEPH during preoperative examinations. She was referred to our hospital, where right heart catheterization revealed a mean pulmonary artery pressure (mPAP) of 39 mmHg. We prioritized the treatment of CTEPH, starting oral riociguat followed by BPA three times. The mPAP decreased to 27 mmHg. Then, right…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
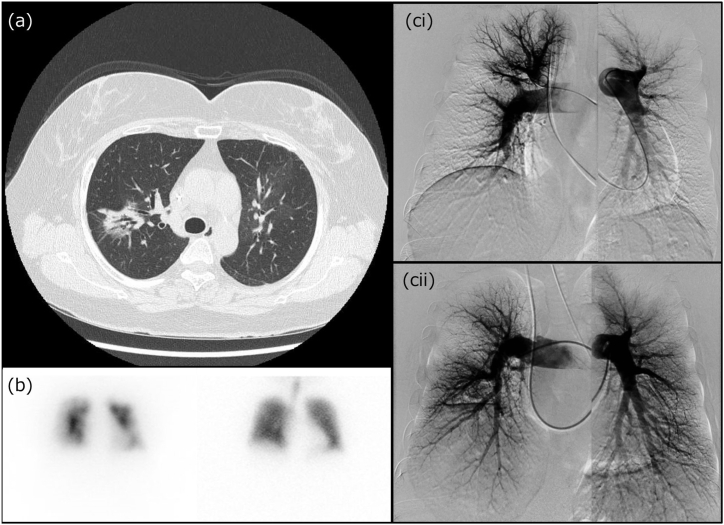 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Heart Failure Treatment and Management · Cardiovascular Function and Risk Factors
Introduction
1
Patients with pulmonary hypertension (PH) are at high risk of perioperative complications and death [1]. Although several pulmonary circulatory markers are used for risk assessment [2,3], definitive protocol are not established.
The cornerstone of treatment for chronic thromboembolic pulmonary hypertension (CTEPH) is lifelong anticoagulation followed by pulmonary thromboendarterectomy (PEA) when feasible [2]. However, performing PEA is sometimes difficult when pulmonary artery thrombus are predominantly distributed in the peripheral regions [4]. Pulmonary vasodilators and ballon pulmonary angioplasty (BPA) have recently been recognized as important treatment options [2]. BPA has been reported to produce the same therapeutic outcomes as PEA [5]. In particular, additional treatment with BPA after oral administration of riociguat was shown to contribute to further improvements in exercise capacity, and pulmonary hemodynamics [6].
Here, we report a patient simultaneously diagnosed with CTEPH and operable lung cancer.
Case presentation
2
A 55-year-old woman, with a smoking history of 7.5 pack-years, had a medical history of hypertension, asthma, and left breast cancer, which was treated with surgery and postoperative chemotherapy. A central venous port was implanted in her chest. The patient had experienced exertional dyspnea for several years. During a health checkup, a tumor shadow was detected in the right middle lung field on chest radiography, leading to a referral to a nearby hospital. Chest computed tomography (CT) revealed a part-solid ground-glass opacity with a long diameter of 3 cm in the upper lobe of the right lung (Fig. 1a). No malignant findings were observed during bronchoscopy; however, the tumor did not shrink after six months of follow-up. The patient was referred for thoracic surgery for diagnostic treatment of the lung tumor, which was suspected to be primary lung cancer. However, preoperative electrocardiography showed increased p-waves and right-axis deviation, suggesting right heart overload. Echocardiography revealed right ventricular enlargement and the maximum velocity of tricuspid regurgitation (TRVmax) was approximately 3.9 m/s, suggesting pulmonary hypertension (PH). Additionally, pulmonary perfusion scintigraphy revealed multiple bilateral defects, whereas ventilation scintigraphy showed no defects (Fig. 1b). These results suggested chronic thromboembolic pulmonary hypertension (CTEPH), and treatment with edoxaban was initiated.Fig. 1. Radiological images(a) Chest computed tomography showing a part-solid ground-glass opacity with a long diameter of 3 cm in the upper lobe of the right lung (arrow), which turned out to be papillary adenocarcinoma.(b) Pulmonary perfusion scintigraphy presenting multiple defects bilaterally, whereas ventilation scintigraphy shows no defects.(ci) Pulmonary angiography performed at the time of diagnosis, showing weak distal perfusion on both sides.(cii) Pulmonary angiography performed after the third BPA session and lobectomy of the right upper lobe, showing an improvement in blood flow.Fig. 1
The patient was referred to our institution for further investigation. The values from right heart catheterization were as follows: pulmonary artery pressure (PAP; systolic/diastolic/mean), 69/18/39 mmHg; pulmonary artery wedge pressure (PAWP), 5 mmHg; right atrial pressure (RAP), 3 mmHg; pulmonary vascular resistance (PVR), 9.1 Wood units; cardiac output (CO), 3.72 L/min; cardiac index (CI), 2.24 L/min/m^2^ (Table 1). Blood test showed elevated level of brain natriuretic peptide (BNP); 216.1 pg/mL. Pulmonary arteriography revealed a peripherally predominant blood-flow defect, which led to a definitive diagnosis of CTEPH (Fig. 1ci). We considered that her pulmonary hemodynamics put her at high risk for requiring surgery for lung cancer. Therefore, the initial approach was to focus on the treatment of PH. After discussions with physicians, surgeons, and radiologists, a combination therapy with pulmonary vasodilators and balloon pulmonary angioplasty (BPA) was planned. After the introduction of riociguat, the patient underwent BPA three times. After the third BPA, mean PAP (mPAP) decreased to 27 mmHg and PVR decreased to 5.0 Wood units (Table 1). Pulmonary arteriography revealed improvement in peripheral blood flow, and BNP was reduced to 28.3 pg/mL.Table 1. Findings of right heart catheter.Table 1. ParametersAt diagnosisAfter the 3rd BPAAfter the lobectomyAfter 1 year of lobectomysPAP, mmHg69466437dPAP, mmHg18161813mPAP, mmHg39273622PAWP, mmHg58710RAP, mmHg3NA43PVR, Wood unit9.15.03.42.5CO, L/min3.723.808.575.84CI, L/min/m^2^2.242.225.043.33PaO_2_, mmHg65.4NA58.072.8PvO_2_, mmHg38.741.042.038.4BPA, ballon pulmonary angioplasty; CI, cardiac index; CO, cardiac output; dPAP, diastolic pulmonary artery pressure; mPAP, mean pulmonary artery pressure; sPAP, systolic pulmonary artery pressure; PAWP, pulmonary artery wedge pressure; PaO_2_, partial pressure of arterial oxygen; PvO_2_, partial pressure of mixed venous oxygen; PVR, pulmonary vascular resistance; RAP, right atrial pressure.
Right upper lobectomy with lymph node dissection was performed in the thoracic surgery department. The pathological diagnosis after surgery was papillary adenocarcinoma T1cN1M0, pStage IIB (8th edition staging by the Union for International Cancer Control). Two weeks after surgery, the TRVmax surveyed by echocardiography was approximately 4.1 m/s, which was nearly equivalent to the value before BPA. However, the results of right heart catheterization performed at almost the same time indicated no exacerbation of PVR: PAP (systolic/diastolic/mean), 64/18/36 mmHg; PAWP, 7 mmHg; RAP, 4 mmHg; PVR, 3.4 Wood units; CO, 8.57 L/min; CI, 5.04 L/min/m^2^. Hypoxia due to lung resection was presumed to be the main cause of the increased cardiac output. Additionally, selexipag introduced postoperatively may have contributed to the increased cardiac output. The patient was discharged on long-term oxygen therapy because of persistent hypoxemia, which required 2 L/min oxygen inhalation. Since then, PH has stabilized, and the lung cancer has progressed without recurrence.
Discussion
3
This is the first report of successful management of a case of concomitant CTEPH and primary lung cancer. Although no study has suggested a direct relationship between CTEPH and lung cancer, it is generally recognized that a cancerous state increases coagulability and the risk of venous thromboembolism [7]. Additionally, in this case, the patient had a central venous port, which may have contributed to the development of CTEPH [8].
A recent study on perioperative outcomes in patients with PH found that 11.3 % had serious postoperative complications and 4.7 % died within 30 days after undergoing noncardiac surgery [9]. Bleeding is the serious perioperative complication in thoracic surgery. To the best of our knowledge, no reports have been made of pulmonary hypertension as a risk factor for intraoperative bleeding. However, anticoagulants and prostacyclin receptor agonists used to treat CTEPH will increase the risk of bleeding. Additionally, preoperative heparin administration was reported as the risk factor of bleeding requiring reoperation [10]. Fragility of pulmonary vessel walls due to pulmonary hypertension may also affect susceptibility to perioperative bleeding.
There are no firm indicators for evaluating postoperative risk [9]. Modifying some values, such as CI, RAP and BNP, which can be used for risk classification in PH, to low-risk range may help avoid perioperative adverse events [2,3].
However, in the management ahead of pulmonary resection for CTEPH patients, it is also necessary to thoroughly evaluate blood flow in each segment. In this case, the right heart catheterization performed after referral to our hospital showed high mPAP, PVR, and BNP, while CI was 2.2 L/min and RAP was 4 mmHg, both of which were not particularly unfavorable. However, pulmonary angiography and lung perfusion scintigraphy suggested that the blood flow around the tumor was well preserved; therefore, lobectomy for lung cancer was highly likely to exacerbate oxygenation and pulmonary hemodynamics. Therefore, it was important to improve perfusion in the remaining lung by implementing additional treatment preoperatively.
Adjuvant chemotherapy with cisplatin and vinorelbine is effective for completely resected stage II–III non-small cell lung cancer [11]. However, in this case, adjuvant chemotherapy was not administered because hydration from the cisplatin-based chemotherapy could worsen her pulmonary hemodynamics.
Conclusion
4
It was essential to administer appropriate medical therapy and BPA to make the patient tolerable for lung cancer surgery. But the treatment for cases of coexisting CTEPH and lung cancer remains unclear and further research is needed.
CRediT authorship contribution statement
Satoshi Isomatsu: Writing – original draft, Investigation, Data curation. Kenichiro Takeda: Writing – review & editing, Project administration, Investigation, Data curation, Conceptualization. Yu Shionoya: Validation, Data curation. Toshihiko Sugiura: Validation, Supervision, Data curation. Shizu Miyata: Validation, Data curation. Shun Imai: Validation, Data curation. Jun Nagata: Validation, Data curation. Yu Taniguchi: Validation, Data curation. Akira Naito: Validation, Data curation. Rika Suda: Validation, Data curation. Ayako Shigeta: Validation, Data curation. Nobuhiro Tanabe: Validation, Data curation. Takuji Suzuki: Validation, Supervision.
Patient consent
The patient provided written informed consent.
Funding
None.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pilkington S.A.Taboada D.Martinez G.Pulmonary hypertension and its management in patients undergoing non-cardiac surgery Anaesthesia 7012015 Jan 56702526749310.1111/anae.12831 · doi ↗ · pubmed ↗
- 2Humbert M.Kovacs G.Hoeper M.M.ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension Eur. Respir. J.611202222008792023 Jan 10.1183/13993003.00879-202236028254 · doi ↗ · pubmed ↗
- 3Price L.C.Martinez G.Brame A.Perioperative management of patients with pulmonary hypertension undergoing non-cardiothoracic, non-obstetric surgery: a systematic review and expert consensus statement Br. J. Anaesth.12642021 Apr 7747903361224910.1016/j.bja.2021.01.005 · doi ↗ · pubmed ↗
- 4Madani M.M.Pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension: state-of-the-art 2020 Pulm. Circ.11220212045894021100737210.1177/20458940211007372 PMC 815048634104418 · doi ↗ · pubmed ↗
- 5Masaki K.Hosokawa K.Funakoshi K.Outcomes of chronic thromboembolic pulmonary hypertension after balloon pulmonary angioplasty and pulmonary endarterectomy JACC Asia 482024 Aug 5775893915650910.1016/j.jacasi.2024.05.007PMC 11328766 · doi ↗ · pubmed ↗
- 6Wang W.Wang J.Yang S.Better efficacy of sequential combination with balloon pulmonary angioplasty after long-term riociguat for patients with inoperable chronic thromboembolic pulmonary hypertension Pulm. Circ.1432024 Jule 1242910.1002/pul 2.12429 PMC 1134520439188536 · doi ↗ · pubmed ↗
- 7Nasser N.J.Fox J.Agbarya A.Potential mechanisms of cancer-related hypercoagulability Cancers 1232020 Feb 5663212138710.3390/cancers 12030566 PMC 7139427 · doi ↗ · pubmed ↗
- 8Machat S.Eisenhuber E.Pfarl G.Complications of central venous port systems: a pictorial review Insights Imaging 1012019 Aug 863146364310.1186/s 13244-019-0770-2PMC 6713776 · doi ↗ · pubmed ↗