Removal of lollipop-shaped stent-stone complex using direct-vision laser lithotripsy
Shuping Wang, Xinying Tang, Bing Hu, Kunke Wang, Lijun Xu, Daojian Gao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
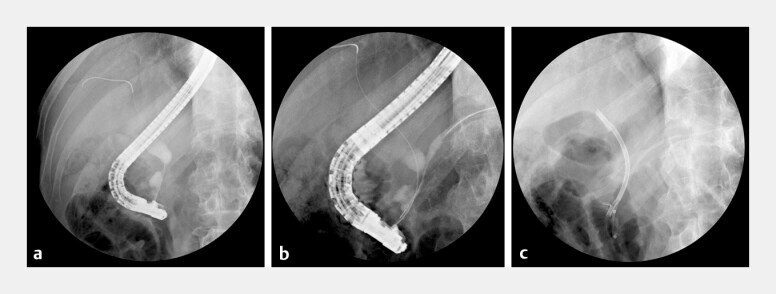 Fig. 1
Fig. 1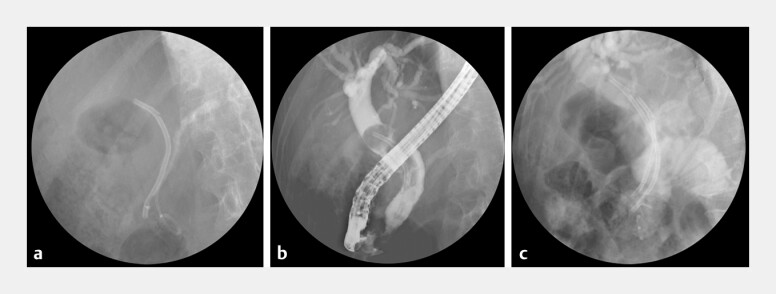 Fig. 2
Fig. 2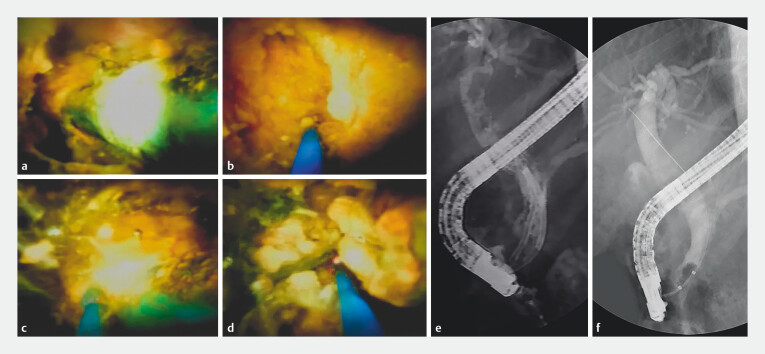 Fig. 3
Fig. 3- —Science and Technology Innovation Plan of Science and Technology Commission of Shanghai Municipality, China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Kidney Stones and Urolithiasis Treatments
Long-term retention of biliary plastic stents (PS) can lead to a rare complication: the formation of a lollipop-shaped stent-stone complex (LSSC) 1 , where stones encase the proximal end of the stent, making endoscopic removal technically difficult. We report a case of successful LSSC removal using peroral cholangioscopy (POCS)-guided frequency-doubled dual pulse Nd:YAG (FREDDY) laser lithotripsy.
A 72-year-old man, previously diagnosed with IgG4-related sclerosing cholangitis, underwent biliary and pancreatic PS placement three years prior to alleviate obstructive jaundice ( Fig. 1 ), followed by corticosteroid therapy. He was lost to follow-up. One month before admission, he presented with jaundice and fever. Emergency ERCP showed resolution of the biliary stricture but revealed a retained LSSC in the common bile duct (CBD). Removal attempts using standard tools failed, fracturing the stent at the duodenal lumen. A supplementary PS was placed to ensure drainage ( Fig. 2 ). Following stabilization, repeat ERCP was performed using POCS-guided laser lithotripsy. The PS was fully encased in yellow stones, forming an LSSC. FREDDY laser lithotripsy (U-100 Plus; World of Medicine, Berlin, Germany) was applied at the stent-stone interface under direct visualization to fragment the stones and gradually release the stent. The stent was successfully removed, and residual stones were cleared ( Fig. 3 , Video 1 ). The patient recovered well and was discharged three days later.
Initial ERCP findings (3 y prior). a Cholangiography showed a smooth, symmetrical stricture in the pancreatic segment of the common bile duct with upstream dilation. b Pancreatography revealed a slender, smooth stricture in the pancreatic head region of the main pancreatic duct, with mild dilation in the body and tail. c Plastic stents were placed in both the bile and pancreatic ducts.
Emergency ERCP findings (1 mo prior). a Biliary and pancreatic plastic stents were seen in situ, with cast-like pancreatic duct stones along the pancreatic stent. b Cholangiography revealed a round filling defect encasing the stent, forming a lollipop-shaped stent-stone complex. c A second biliary stent was placed alongside the original.
POCS-guided laser lithotripsy for LSSC removal. a POCS visualized a blue plastic stent encased in yellow stones, forming an LSSC. b, c A laser fiber was applied to the stent-stone interface and large stone. d Lithotripsy successfully fragmented the stone. e Cholangiography confirmed LSSC resolution and stone fragmentation. f Both stent and stone fragments were removed; balloon-occluded cholangiography showed no residual filling defects.
LSSC formation is associated with long-term stent retention (≥301 days) and CBD dilation 2 . The potential for LSSC formation should be considered in patients with long-term PS indwelling and dilated CBD. Endoscopic LSSC removal is technically challenging: standard endoscopic tools may fail, and forcible extraction risks ductal injury and perforation. Extracorporeal shock wave lithotripsy is technically complex 3 , while surgical intervention is traumatic. FREDDY laser lithotripsy is safer than Ho:YAG laser and electrohydraulic lithotripsy 4 5 . POCS-guided FREDDY laser lithotripsy offers a safe, minimally invasive, and effective approach for LSSC management.
Removal of lollipop-shaped stent-stone complex using direct-vision laser lithotripsy.Video 1
Endoscopy_UCTN_Code_CPL_1AK_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tang SJ Armstrong L Lara LF De novo stent-stone complex after long-term biliary stent placement: pathogenesis, diagnosis, and endotherapy Gastrointest Endosc 20076619320010.1016/j.gie.2006.12.02617521649 · doi ↗ · pubmed ↗
- 2Kaneko J Kawata K Watanabe S Clinical characteristics and risk factors for stent-stone complex formation following biliary plastic stent placement in patients with common bile duct stones J Hepatobiliary Pancreat Sci 20182544845410.1002/jhbp.58430289200 · doi ↗ · pubmed ↗
- 3Manes G Paspatis G Aabakken L Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline Endoscopy 20195147249110.1055/a-0862-034630943551 · doi ↗ · pubmed ↗
- 4Veld J Vvan Huijgevoort NCM Boermeester MAA systematic review of advanced endoscopy-assisted lithotripsy for retained biliary tract stones: laser, electrohydraulic or extracorporeal shock wave Endoscopy 20185089690910.1055/a-0637-880629991072 · doi ↗ · pubmed ↗
- 5Ni ZK Jin HM Li XW Combination of Electronic Choledochoscopy and Holmium Laser Lithotripsy for Complicated Biliary Calculus Treatment: A New Exploration Surg Laparosc Endosc Percutan Tech 201828 e 68e 7310.1097/sle.000000000000053129668665 · doi ↗ · pubmed ↗