Simultaneous submucosal tunneling endoscopic septum division and submucosal tunneling endoscopic resection for epiphrenic diverticulum combined with an esophageal submucosal tumor
Shao-Bin Luo, Zu-Qiang Liu, Li Wang, Quan-Lin Li, Ping-Hong Zhou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
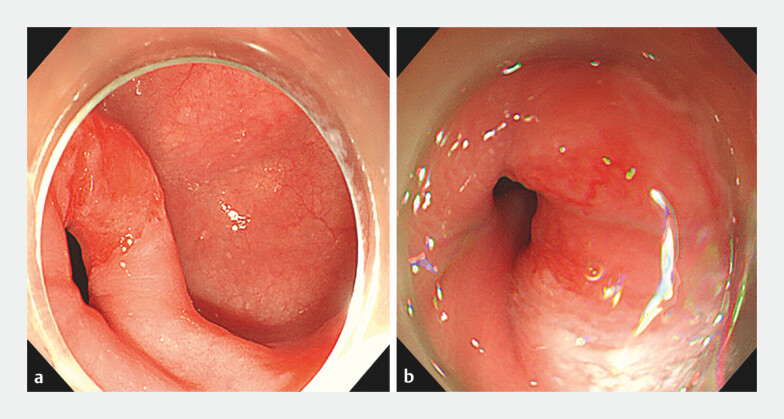 Fig. 1
Fig. 1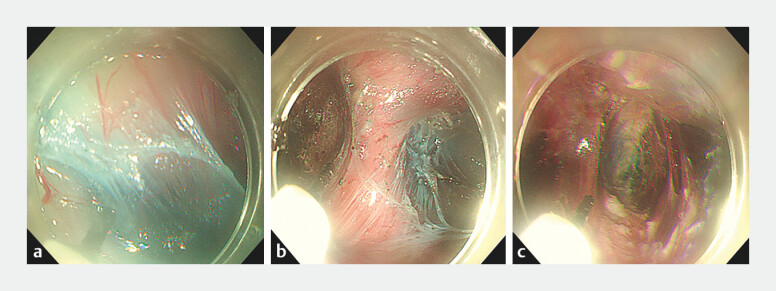 Fig. 2
Fig. 2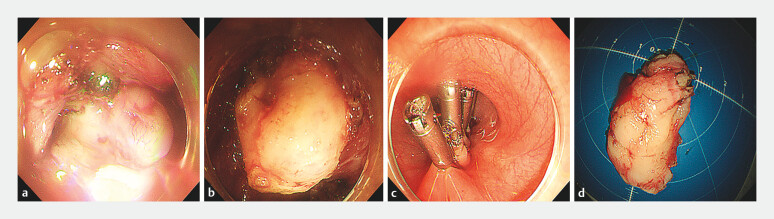 Fig. 3
Fig. 3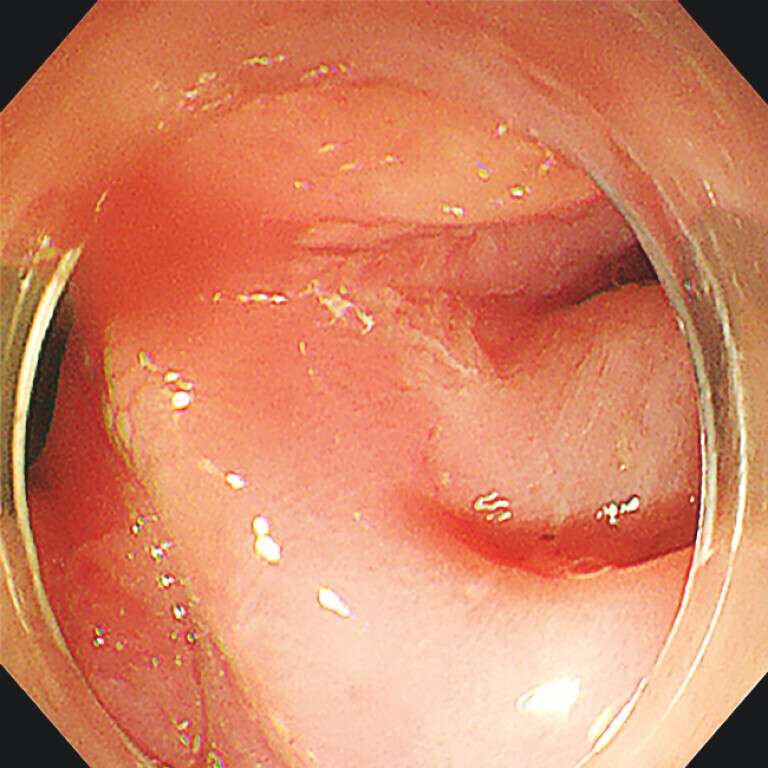 Fig. 4
Fig. 4- —The National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Dysphagia Assessment and Management · Gastrointestinal disorders and treatments
A 43-year-old woman was admitted with a history of dysphagia for 2 years. Endoscopy showed an esophageal submucosal tumor and an epiphrenic diverticulum located above the esophagogastric junction (EGJ) ( Fig. 1 ). Submucosal tunneling endoscopic septum division (STESD) combined with submucosal tunneling endoscopic resection (STER) with was performed ( Video 1 ).
Endoscopic images showing: a an epiphrenic diverticulum; b a submucosal tumor in the cardia.
Simultaneous STESD and STER in one tunnel for an epiphrenic diverticulum combined with an esophageal submucosal tumor.Video 1
After the submucosal tunnel had been established, the annular muscle bundle and diverticular ridge were completely transected, and the whole layer of the esophageal muscle bundle was completely severed 2 cm above and below the EGJ ( Fig. 2 ). In addition, the esophageal muscularis propria above the cardia showed obvious thickening in the tunnel. A 4.0-cm submucosal tumor with unclear boundaries was found, and full-thickness resection was performed ( Fig. 3 ). The postoperative pathological diagnosis was leiomyoma. The patient was discharged on postoperative day 3 without complications. Follow-up endoscopy 1 year after the procedure confirmed the base of diverticulum was flattened ( Fig. 4 ), and the patient’s symptoms of dysphagia had disappeared.
Endoscopic images showing : a the creation of a submucosal tunnel; b, c complete transection of the muscle of the diverticulum septum.
Endoscopic images showing: a a submucosal tumor with unclear boundaries b full-thickness resection being performed; c closure of the tunnel entrance with metal clips. d The resected specimen, which was 4 × 2 cm in size.
Endoscopic image at follow-up 1 year later showing the flattened base of diverticulum.
This case is the first report of simultaneous STESD and STER in one tunnel for an epiphrenic diverticulum with an esophageal submucosal tumor. Incision of the diverticular ridge and the spastic muscle layer within the same tunnel aimed avoid mucosal injury and esophageal perforation, which can greatly increase the difficulty of such procedures. The traditional treatment for an epiphrenic diverticulum with an esophageal submucosal tumor would be laparoscopic epiphrenic diverticulectomy, myotomy, and fundoplication, which is associated with high postoperative morbidity 1 . The advantage of STER is preservation of the overlying mucosal flap, which ensures the relative integrity of the esophageal wall, thereby reducing the risk of infection and pneumomediastinum.
This case suggests that the application of simultaneous STESD and STER in one tunnel may be a safe and effective technique for an epiphrenic diverticulum combined with an esophageal submucosal tumor.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.