The Impact of Post-COVID-19 Condition on Frontline Healthcare Workers: A Scoping Review
Elsie Duff, Em Pijl, Cindy Fehr, Sai Krishna Gudi

TL;DR
This review explores how post-COVID-19 conditions affect healthcare workers' physical and mental health, highlighting the need for policy changes.
Contribution
The study provides a comprehensive overview of post-COVID-19 impacts on frontline healthcare workers, addressing a critical research gap.
Findings
Persistent symptoms like fatigue and anxiety significantly affect healthcare workers' quality of life.
Cross-sectional studies from countries like Italy, India, and Brazil show widespread post-COVID-19 conditions among HCWs.
Findings highlight the need for healthcare policies to support affected workers and address pandemic impacts.
Abstract
The main goal of this integrative scoping review was to address the knowledge gap and inform policy and research regarding the impact of post-COVID-19 conditions on frontline healthcare workers (HCWs). An integrative scoping review using Arksey and O'Malley's framework examined post-COVID-19 conditions in frontline HCWs. We searched CINAHL, EMBASE, APA PsycINFO, PubMed, Social Science Database, ProQuest, Social Science Journals, and Web of Science, including dissertations, conference proceedings, and government publications for gray literature. A preestablished data extraction tool was developed to capture relevant information about post-COVID-19 conditions in HCWs. Of the total 42 studies, the majority were cross-sectional in design (29) and conducted mainly in countries such as Italy (4), India (3), and Brazil (3). Study findings reveal that a substantial proportion of HCWs in various…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
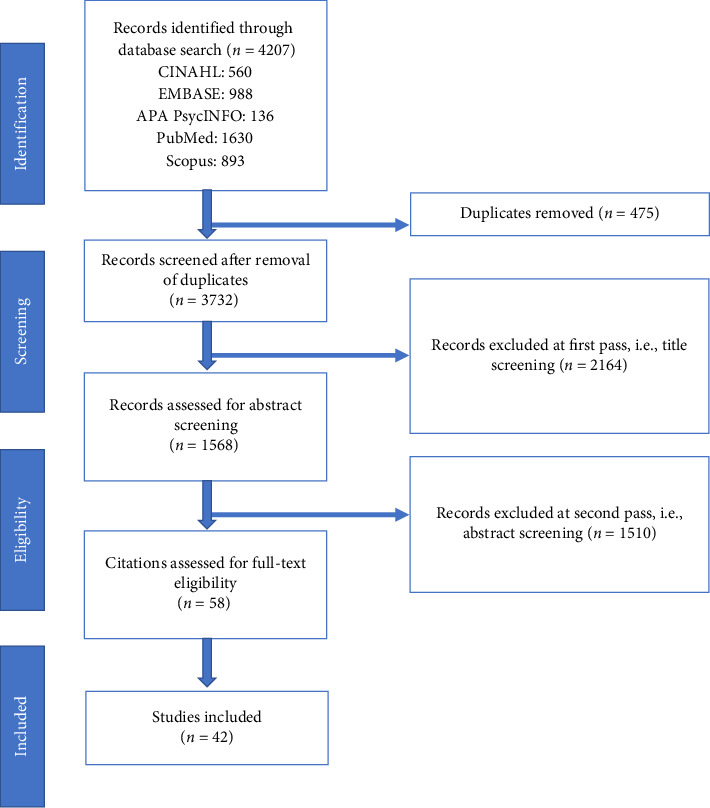 Figure 1
Figure 1- —University of Manitoba
- —Manitoba Centre for Nursing and Health Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Long-Term Effects of COVID-19 · Healthcare professionals’ stress and burnout
1. Introduction
During the coronavirus disease 2019 (COVID-19) pandemic, healthcare workers (HCWs) faced multiple physical and psychological challenges while carrying out their duties [1]. Frontline HCWs were particularly vulnerable to respiratory droplets and aerosol transmission, owing to their work to contain the disease [2]. In addition to the risk of becoming infected with COVID-19, HCWs also suffered from insomnia, loneliness, sleep disorders, and mental depression due to the workload demands and related stress [3]. HCWs also experienced anxiety and frustration due to uncertainty, lack of knowledge, environmental changes, and fear of being infected and carrying the infection to their respective family members [3]. That being said, HCWs' concerns related to maintaining physical distance from their family members to reduce the risk of infection resulted in further psychological distress [4]. Thus, exceptional attention to monitoring the psychological issues of HCWs exposed to COVID-19 becomes essential [5], where research is needed.
COVID-19 compounded the mental health of HCWs due to the high number of cases and deaths of patients and coworkers, not to mention the fear of being infected and carrying the virus to their homes [6]. Other factors of concern included precarious working conditions, long shifts, and lack of personal protective equipment (PPE) [7]. Anxiety has been a common mental health–related symptom presented by HCWs during the COVID-19 pandemic [8]. However, the nature and extent of the impact of the COVID-19 pandemic on HCWs' mental health are largely unknown.
The World Health Organization (WHO) defines post-COVID condition (PCC) symptoms as the persistence or relapse of symptoms at least 12 weeks after the onset of COVID-19 without an alternative diagnosis [9]. The symptoms reported in a recent meta-analysis concluded that HCWs encountered a range of enduring psychological stressors, including anxiety (37%), sadness (36%), and insomnia (32%) [2]. While PCC includes an extensive array of symptoms or difficulties apparent in everyday living, neurocognitive symptoms such as fatigue, memory or concentration problems, and sleep disruption are among the most frequent and debilitating [10, 11]. Large-scale epidemiological studies quantifying the memory, concentration, and executive dysfunction among HCWs with PCC are still lacking. In particular, the impact of PCC on cognitive dysfunction needs to consider the potential contributions of fatigue and psychological distress, which are known to have deleterious effects on cognitive abilities [12]. Fatigue and psychological distress are highly prevalent among HCWs in the context of the additional workload caused by the pandemic, where these symptoms are largely unexplored in research. Therefore, it is important to examine PCC in HCWs to understand the broader impact of the COVID-19 pandemic on the healthcare workforce, inform policy, and identify vulnerabilities that impact HCWs.
2. Methods
2.1. Study Design
An integrative scoping review was conducted to identify essential PCC concepts important to support the health and well-being of HCWs. The Arksey and O'Malley [13] six-stage scoping review framework was used to integrate various sources, including guidelines, editorials, and gray literature (which is a helpful strategy, especially when there is limited evidence on the topic of interest). The framework was utilized to locate, summarize, and integrate the best evidence regarding the extent and nature of the impact of PCC among HCWs.
2.2. Search Strategy
The initial search terms were determined using research questions to build a comprehensive search strategy: What effect has PCC (i.e., physical or psychological symptoms 12 weeks post COVID-19 infection, e.g., fatigue, memory problems, sleep disturbances, shortness of breath, anxiety and depression, general pain and discomfort, difficulty thinking or concentrating, and posttraumatic stress disorder) had on HCWs? Relevant keywords such as “long-COVID,” “post-COVID-19,” “post-COVID condition,” “PCC,” “PCC symptoms,” “healthcare workers,” “health personnel,” and “frontline healthcare workers” were searched with the subject headings from each database.
For instance, the detailed search strategy interpretation using PubMed was as follows: (“Post-Acute COVID-19 Syndrome”[MeSH Terms] OR “long haul covid”[Title/Abstract] OR “post covid”[All Fields] OR “Post acute covid”[Title/Abstract] OR “long COVID”[Title/Abstract] OR “PCC”[Title/Abstract] OR “pcc symptom^∗^”[Title/Abstract]) AND (“Health Personnel”[MeSH Terms] OR “frontline”[Title/Abstract] OR “healthcare personnel”[Title/Abstract] OR “health care personnel”[Title/Abstract] OR “healthcare worker^∗^”[Title/Abstract] OR “health care worker^∗^”[Title/Abstract] OR “health care provider^∗^”[Title/Abstract] OR “healthcare provider^∗^”[Title/Abstract] OR “Health Care Professional”[Title/Abstract] OR “healthcare professional^∗^”[Title/Abstract] OR “health care professional^∗^”[Title/Abstract] OR “hospital worker^∗^”[Title/Abstract] OR “hospital personnel”[Title/Abstract] OR “medical worker^∗^”[Title/Abstract] OR “medical provider^∗^”[Title/Abstract] OR “hospital employee”[Title/Abstract] OR “healthcare employee^∗^”[Title/Abstract] OR “hospital staff^∗^”[Title/Abstract] OR “healthcare staff”[Title/Abstract] OR “health care staff”[Title/Abstract]). The search strategy was reviewed by a research librarian at the authors' university. Preliminary criteria considered gray literature and English-language research studies from January 01, 2020, through April 07, 2025.
2.3. Study Selection
Electronic scientific databases such as CINAHL with full-text EBSCOhost, EMBASE-Ovid, APA PsycINFO-Ovid, PubMed, and Scopus databases were searched, including gray literature through hand searching. Initial research produced 4207 records, where 475 duplicate studies were removed using Zotero. At the second pass, i.e., title screening, 2164 studies were excluded, whereas at the third pass, i.e., abstract screening, an additional 1510 studies were excluded. After thoroughly reviewing full-text articles, 16 studies were excluded (Figure 1). A research coordinator searched, retrieved, and completed the data extraction of articles using the Zotero reference management system. In collaboration with the research coordinator, two independent investigators from the research team reviewed the abstracts, coded the articles, and decided if the inclusion criteria had been met. Ultimately, 42 studies were included in this scoping review. Articles relevant to PCC among HCWs with symptoms of physical and mental wellness (i.e., fatigue, memory problems, sleep disturbances, shortness of breath, anxiety and depression, general pain and discomfort, difficulty thinking or concentrating, or stress) were included. The characteristics and primary findings of the included studies are presented in Table 1.
The research team developed a preestablished data extraction tool to capture participant demographics, professional designation, sample size, measures/assessments, outcomes, results, and author conclusions relevant to PCC among HCWs. Once the independent reviews were completed, the investigators compared the results and discussed any differences, returning to the original study for the rationale to support their opinion. The third reviewer decided to include or exclude the study based on the criteria identified in the data extraction and review process if the team could not reach a consensus.
2.4. Data Charting
Zotero reference management software [56] was used to store the articles, note comments on inclusion and exclusion, and summarize the extracted data. The Zotero software was also used to identify articles to an “INCLUDE” folder and to remove duplicate citations. Summaries included identifying the reviewer, research question(s), study purpose, country of origin, study methodology, participants, sample size, measurements used, theories identified, results, limitations, relevance to the research questions, reviewer's recommendation, and a synopsis of the article.
3. Results
Of the 42 studies included in the review, the majority were cross-sectional studies (n = 29), followed by prospective/retrospective (n = 6), case-control (n = 3), multimethod/descriptive (n = 2), and mixed methods (n = 2) studies. Geographically, most of the included studies were conducted in Italy (n = 4), India (n = 3), Brazil (n = 3), Saudi Arabia (n = 2), United Kingdom (n = 2), China (n = 2), Egypt (n = 2), England (n = 2), Germany (n = 2), Portugal (n = 2), Switzerland (n = 2), Turkey (n = 2), and the USA (n = 2), followed by one study each in Canada, Indonesia, France, Latin America, Ireland, Jordan, Palestine, Philippines, South Africa, Sweden, Malaysia, and Tunisia. These investigations collectively aimed to analyze various aspects of HCWs' PCC experiences and outcomes.
4. Discussion
This scoping review serves as a fundamental step in informing healthcare workforce policy to address the broader impacts of the COVID-19 pandemic. Across multiple countries and study designs, HCWs who had contracted COVID-19 commonly experienced a range of persistent symptoms. Below is the list of reported PCC symptoms from the included literature based on the severity and frequency of occurrence.
4.1. Symptom Implications
4.1.1. Fatigue
Fatigue was the most common symptom reported by HCWs [14–32, 34–55, 57], which often co-occurred with other symptoms. All the included studies in this review indicated a significant prevalence of severe fatigue among HCWs. In Germany, 11% of HCWs reported experiencing severe fatigue, correlating with heightened psychological distress, diminished quality of life, and increased work incapacity [58]. Similarly, a study conducted in China found that 76% of HCWs with severe COVID-19 continued to experience symptoms of fatigue and weakness even 28 months post-discharge, with 18.7% failing to recover their functionality fully [23]. The persistence of symptoms, particularly fatigue and anxiety, has been linked to a decline in overall quality of life, decreased work ability, and impaired health-related quality of life among HCWs [24]. Notably, fatigue emerged as the most frequently reported symptom among HCWs in Italy, affecting 32.1% of individuals studied, followed by musculoskeletal pain (13.6%) and dyspnea (13.2%) [24]. Furthermore, research from Turkey highlighted the long-term impact of COVID-19 on young patients, with mild and moderate cases experiencing PCC symptoms that significantly impacted their quality of life [21]. Among German HCWs, 31.5% reported persistent impairment in their quality of life, underscoring the persistent effects of COVID-19 on HCWs [31]. A common occurrence of concentration, brain fog, or memory deficiency was reported with long COVID-19 symptoms in HCWs [15, 21, 22, 27, 29–32, 34, 37–40, 51, 52, 57]. These findings emphasize the need for targeted interventions and support mechanisms to address the complex challenges posed by post-COVID fatigue and its ramifications on individuals' well-being and occupational functioning.
4.1.2. Muscle or Joint Pain
Frontline HCWs who recovered from COVID-19 frequently reported persistent musculoskeletal symptoms, including muscle and joint pain [39, 40, 42, 44–48, 51–53]. Studies consistently indicate that these symptoms can significantly increase in intensity and frequency post-infection [25], whereas the most frequent symptom in the post-acute phase includes muscle aches. Furthermore, a significant proportion of post-COVID-19 patients met the criteria for fibromyalgia, with prevalence rates ranging from 31% to 40% [17]. In a similar study, HCWs reported the most common presenting symptoms as fatigue (73.6%) and muscle or joint pain (73.6%) [20]. The long-term impact of COVID-19 on musculoskeletal health among HCWs is particularly concerning, given the physically demanding nature of their roles. Persistent pain and reduced physical activity can significantly decline the quality of life and work capacity. Therefore, it is crucial to implement comprehensive rehabilitation programs and pain management protocols tailored to the needs of the essential workforce [23, 24]. Muscle or joint pain is vital for HCWs' safety, ergonomics, wellness, or disability management to address, preventing injury or loss of function for work productivity by employers.
4.1.3. Headache
Following fatigue and joint or muscle pain, headache was reported to be one of the most frequent symptoms among HCWs [39, 44–48, 51, 54]. In Jordan, almost three-quarters (71.4%) of HCWs who participated in the study reported headache as one of the most frequent symptoms of COVID-19 infection during the acute and follow-up phases of infection [20]. The prevalence of headache as a post-COVID symptom among HCWs in Italy was found to be more than 27% [25]. Similarly, a recent study conducted in the USA identified headache as a frequently reported symptom, even after 6 weeks of COVID-19 infection, posing a substantial disease burden among HCWs [28]. A similar German study reported that more than 70% and 41% of the HCWs experienced headaches during COVID-19 infection and post-COVID-19 syndrome, respectively [30]. Lastly, a recent study in India reported that around 35% and 15% of the HCWs experienced headaches during active illness and post-COVID-19 recovery, respectively [32]. Headache is a common reason for work absences, impacting essential HCW human resources and patient care.
4.1.4. Depression
Compared to the general public, the overall depression scores among recovered HCWs were reported to be higher (mean DASS-21 score of 25.9) [15]. A notable percentage of HCWs still experience normal to mild depression, especially HCWs under 30 years of age, who exhibit higher depression levels than their older counterparts. This study also found that longer quarantine durations were associated with increased depression levels, underscoring the psychological toll of prolonged isolation. Wang et al. [37] provided evidence that preexisting mental health conditions and preinfection psychological distress, including depression, anxiety, perceived stress, loneliness, and worry about COVID-19, significantly increased the risk of developing PCC symptoms and associated daily life impairments. In a study by Gaber et al. [18], 44% of respondents reported mood disorders, including depression, during the post-COVID-19 period. Despite acknowledging the severity of their symptoms, many HCWs were reluctant to seek medical advice or take sick leave, potentially exacerbating chronic symptoms due to maladaptive coping strategies [18]. Additionally, Mendola et al. [27] noted persistent anxiety and depression among HCWs even 10 months after recovery, significantly impacting their workability and fitness to work. That is, the post-COVID syndrome is linked with reduced work ability, with recommendations that modifications in workload and shifts to aid recovery are needed [25]. These findings collectively underscore the critical need for ongoing mental health support and monitoring for HCWs recovering from COVID-19. Addressing the psychological impacts, particularly depression, through targeted interventions and supportive workplace policies is essential to mitigate the long-term consequences of PCC symptoms in this vital workforce [39–41, 45].
4.1.5. Anxiety and Stress
The unprecedented circumstances and associated unwanted consequences of the COVID-19 pandemic triggered significant stress among both the public and frontline HCWs [39, 41, 43, 45]. Recent studies reported severe posttraumatic stress symptoms following PCC, especially among HCWs who are young [15, 36, 37]. Younger HCWs, especially those with underlying conditions like asthma, were more likely to experience anxiety, with anxiety and depression being closely linked [37]. Carascal et al. [15] found that recovered HCWs experienced higher levels of distress and anxiety compared to the general population. Factors such as age, tenure, and length of quarantine significantly influenced anxiety levels. Magnavita et al. [25] identified that workers experiencing symptoms for more than 4 weeks exhibited higher levels of anxiety, depression, and fatigue and showed reduced work ability. This group often saw a resurgence of preexisting conditions, leading to a notable decline in their overall quality of life and work performance. The long-term persistence of anxiety and depression post-COVID-19 was noted by Mendola et al. [27] who found that while physical symptoms decreased 10 months after recovery, anxiety and depression remained prevalent. Tempany et al. [34] corroborated these findings, with 22% of HCWs in their study reporting residual psychological symptoms, primarily anxiety, after recovering from COVID-19. These findings are significant as the mental health challenges among post-COVID-19 HCWs are a burden for the workforce.
4.1.6. Sleep Disturbance
HCWs recovering from COVID-19 reported significant cognitive impairments, including difficulties with concentration [43, 48–50], memory, and experiences of “brain fog.” These cognitive issues persisted long term and impacted HCWs' ability to perform tasks efficiently [21]. Moreover, studies consistently highlighted cognitive symptoms as part of the broader spectrum of post-COVID-19 conditions, emphasizing the need for ongoing support and interventions for affected individuals [15, 27, 29, 30, 32, 57]. Several studies emphasized the impact of sleep disturbances among HCWs recovering from COVID-19 [19, 25, 27, 34, 37], significantly affecting physical and mental health, workability, and overall well-being. These studies accentuate the need for interventions to improve sleep quality to support HCWs' recovery and enhance workforce sustainability [19, 25, 27, 34].
4.1.7. Chest Pain
Besides psychological symptoms, PCC also affects the cardiovascular system, where chest pain is frequently reported [17, 38, 39, 45, 57] with palpitations [17] among HCWs with PCC. In the Czech Republic, around 8% of the HCWs reported experiencing chest pain or pressure during the post-acute COVID-19 syndrome [57]. Furthermore, in a South Africa study, 24% of frontline HCWs reported experiencing chest pain during the post-acute COVID-19 syndrome [38]. A similar study in Egypt reported that around 23% and 9% of HCWs experienced chest pain during acute and acute post-COVID-19 infection, respectively [17]. Such symptoms would impact health human resources as chest pain requires a physical assessment and can result in work absence.
4.1.8. Dyspnea
A significant prevalence of dyspnea among HCWs experiencing post-COVID-19 syndrome is evident in the literature [40, 41, 44–47, 52, 53]. D'Ávila et al. [16] identified that 36.2% of 174 HCWs were diagnosed with post-COVID-19 syndrome, with dyspnea affecting 12.7% of this group. This finding is consistent with Fouad et al. [17] who noted that dyspnea was the most frequently reported symptom among 140 HCWs with chronic post-acute COVID-19. Gaber et al. [18] reported that 45% of 138 HCWs experienced persistent symptoms, with dyspnea, anxiety, and sleep disturbances being nearly universal among those still symptomatic 3–4 months after the peak of the COVID-19 wave. Kaplan et al. [21] further highlighted that dyspnea, along with fatigue, was prevalent among HCWs diagnosed with COVID-19, particularly for those whose symptoms persisted over 12 weeks. Respondents also indicated shortness of breath as a persistent symptom post-COVID, with Peters et al. [30] reporting this symptom among 73% of surveyed HCWs and Platten et al. [31] reporting 30.1%. Magnavita et al. [25] observed that dyspnea was present in 20% of their study cohort, along with other persistent symptoms such as fatigue and sensory disturbances. These symptoms, including dyspnea, were comparable to those experienced by patients with severe forms of COVID-19. However, the frequency of dyspnea was lower in cases of mild infection compared to hospitalized patients. Breathlessness was a common health issue in HCWs post-COVID-19 [32]. Moreover, Mendola et al. [27] found that 18 months post-infection, exertional dyspnea and dyspnea at rest remained significant symptoms among HCWs, with 71% reporting at least one COVID-like symptom and 76% experiencing ongoing symptoms 6 weeks after illness onset. Mohr et al. [28] observed that dyspnea was among the symptoms most strongly associated with having no prior vaccination, with 76% of participants reporting persistent symptoms 6 weeks after onset. For employers, dyspnea in the HCW workforce would be essential to consider in relation to the loss of function for work productivity.
4.1.9. Loss of Smell and Taste
Loss of smell and loss of taste during COVID-19 infection is believed to be likely due to damage to the olfactory bulb by the SARS-CoV-2 virus and is one of the most commonly reported symptoms at 12 months post-infection [22]. A study conducted in Turkey to investigate the post-COVID-19 syndrome in HCWs revealed that almost half of the study participants experienced loss of smell (49.6%) and loss of taste (47.1%) during the diagnosis of COVID-19 infection [21]. Around a quarter of the participants still exhibit loss of smell (22.3%) and loss of taste (19%) even after 3 weeks of the infection. Furthermore, loss of smell (13.2% and 11.6%) and loss of taste (9.1% and 6.4%) were persistent among participants after 12 and 24 weeks of COVID-19 infection, respectively [21, 26, 57]. Interestingly, loss of smell was reported more frequently in the acute and post-infection phases than loss of taste. Another study from India noted that the loss of smell and taste (21%) persists beyond recovery from active illness [32]. A survey that examined HCWs' consequences of COVID-19 infection, the risk factors, and the impact on quality of life over time in Germany concluded that loss of smell and taste were severe symptoms in both acute (63.5%) and post-COVID-19 (38.1%) phases [30]. Living with loss of smell or taste can affect one's quality of life beyond enjoying food or healthy nutrition, and for the HCW workforce, the sense of smell is critical to health assessment or identifying safe workplace environments [40, 44, 48].
4.1.10. Sex or Gender Implications
Considering the aspects of sex or gender, several studies observed that female HCWs often experienced PCC symptoms for a longer period compared to males [14, 20, 22]. These findings might be due to the absence of necessary resources for women HCWs. Other study findings reported menstrual changes [20, 57] and higher scores for females having persistent PCC symptoms [15, 18, 19, 25, 35, 41, 42]. Female HCWs worldwide are facing the downstream effects of their work, including mental health issues, increased physical violence, alternative arrangements for their families not to expose them to risk, and physical exhaustion [58]. These adverse differences between sex and gender in the context of PCC research are critical to examine in health workforce studies to develop policy or to support HCWs. Female HCWs who experience PCC require support, rehabilitation, and possibly financial compensation [31].
4.1.11. Older Age HCWs
Recent evidence suggests that older age is a potential risk factor for developing PCC symptoms [42]. However, long-term symptoms of COVID-19 among older adults are highly debated. A retrospective cohort study of HCWs infected with COVID-19 inferred that older age was associated with symptoms persisting over 3 and 12 months. However, in most cases, those reported symptoms were considered mild [26]. In an Italian study, older HCWs were more likely to experience PCC symptoms, especially musculoskeletal pain, dyspnea, and fatigue [24]. However, there is mixed evidence regarding older age and its association with long COVID-19 symptoms. For example, meta-analyses did not support a higher risk of long COVID-19 symptoms associated with older age (age as a continuous variable and categorizing older adults as 60 years and above) [59]. A recent cohort study that assessed psychological and physical recovery among Chinese HCWs with severe COVID-19 at 28 months after discharge concluded that older HCWs with severe COVID-19 recovered slowly compared to their younger counterparts in terms of health-related quality of life, persistent symptoms, functional fitness, and immune function at 28 months after discharge [23]. Different definitions of long-term COVID-19 infection or PCC used in various analyses might explain the differences in these inconsistent findings. Therefore, the significance of old age as a risk factor for developing PCC symptoms requires further investigation.
5. Limitations
This scoping review included articles written and published only in English. The articles examined HCWs from various countries but cannot be generalized concerning PCC and HCWs.
6. Conclusion
This integrative literature review aimed to identify the broader impacts of the COVID-19 pandemic on HCWs and healthcare employers that may be utilized to inform policy or identify vulnerabilities that impact the workforce. Beyond knowledge creation, these findings are essential for employers of frontline healthcare clinicians to understand the profound effects on the health workforce's physical and mental health, including their quality of life. The findings highlight the considerable vulnerabilities within the healthcare sector that compel unified efforts to address the enduring PCC health issues among HCWs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee J.-Y. Lee J. Lee S. H. The Experiences of Health Care Workers During the COVID-19 Pandemic in Korea: A Qualitative Study Journal of Korean Medical Science 20213623 p. e 17010.3346/jkms.2021.36.e 170PMC 820385334128598 · doi ↗ · pubmed ↗
- 2Sun P. Wang M. Song T. The Psychological Impact of Covid-19 Pandemic on Health Care Workers: A Systematic Review and Meta-Analysis Frontiers in Psychology 202112 p. 62654710.3389/fpsyg.2021.626547 PMC 829795334305703 · doi ↗ · pubmed ↗
- 3Søvold L. E. Naslund J. A. Kousoulis A. A. Prioritizing the Mental Health and Well-Being of Healthcare Workers: An Urgent Global Public Health Priority Frontiers in Public Health 20219 p. 67939710.3389/fpubh.2021.679397 PMC 813785234026720 · doi ↗ · pubmed ↗
- 4Botchway S. Fazel S. Remaining Vigilant About COVID-19 and Suicide The Lancet Psychiatry 20218755255310.1016/s 2215-0366(21)00117-633862017 PMC 9764398 · doi ↗ · pubmed ↗
- 5Razu S. R. Yasmin T. Arif T. B. Challenges Faced by Healthcare Professionals During the COVID-19 Pandemic: A Qualitative Inquiry From Bangladesh Frontiers in Public Health 20219 p. 64731510.3389/fpubh.2021.647315 PMC 838331534447734 · doi ↗ · pubmed ↗
- 6Rajkumar R. P. Mental Health Considerations in Children and Adolescents during the COVID-19 Pandemic: A Literature Review
- 7Lai J. Ma S. Wang Y. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019 JAMA Network Open 202033 p. e 20397610.1001/jamanetworkopen.2020.397632202646 PMC 7090843 · doi ↗ · pubmed ↗
- 8Pappa S. Ntella V. Giannakas T. Giannakoulis V. G. Papoutsi E. Katsaounou P. Prevalence of Depression, Anxiety, and Insomnia Among Healthcare Workers During the COVID-19 Pandemic: A Systematic Review and Meta-Analysis SSRN Electronic Journal 202010.2139/ssrn.3594632 PMC 720643132437915 · doi ↗ · pubmed ↗