Venous Blood Gas (VBG) Analysis Is as Safe and Equally Reliable as Arterial Blood Gas (ABG) Analysis in the Determination of Prognosis in Chronic Liver Disease Patients: A Study Conducted in a Tertiary Care Hospital in Uttar Pradesh, India
Manish K Bansal, Veenavadinee Mishra, Raghav Singhal, Mayank Sharma, Chandra Prakash, Sapna Rawat

TL;DR
This study shows that venous blood gas analysis is as effective as arterial blood gas analysis in predicting outcomes for patients with chronic liver disease, offering a safer alternative.
Contribution
The study demonstrates that venous blood gas parameters, especially lactate levels, are reliable predictors of prognosis in chronic liver disease patients.
Findings
Elevated lactate levels strongly correlate with disease severity and mortality in CLD patients.
Venous blood gas parameters like pH and bicarbonate differ significantly across disease severity classes.
Kaplan-Meier analysis confirmed that higher lactate levels are linked to reduced 30-day survival rates.
Abstract
Introduction Chronic liver disease (CLD) frequently causes systemic complications, including acid-base disturbances, significantly influencing patient prognosis. Arterial blood gas (ABG) analysis is traditionally utilized to monitor these disturbances, but presents procedural risks, especially in patients with coagulopathies, which is a well-known complication of chronic liver disease (CLD). Venous blood gas (VBG) analysis has emerged as a safer alternative, yet its prognostic significance in CLD requires further investigation. Aim & objective This study aimed to evaluate the prognostic significance of venous blood gas parameters in chronic liver disease patients. The objectives included assessing VBG parameters in CLD patients, correlating these parameters with disease severity using the Child-Turcotte-Pugh (CTP) score, and determining their predictive role in patient outcomes and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
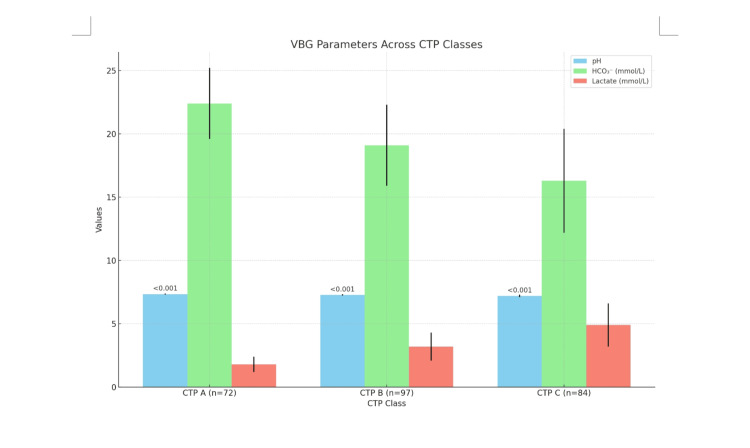 Figure 1
Figure 1| Variable | Frequency (n) | Percentage (%) |
| Gender | ||
| Male | 160 | 63.25 |
| Female | 93 | 36.75 |
| Education | ||
| Primary | 103 | 41.67 |
| Illiterate | 87 | 34.87 |
| Secondary | 63 | 25.00 |
| Socioeconomic Status (BG Prasad) | ||
| Lower Middle | 81 | 32.40 |
| Middle | 73 | 29.20 |
| Lower | 44 | 17.60 |
| Upper Middle | 42 | 16.80 |
| Upper | 13 | 5.20 |
| Etiology | Frequency (n) | Percentage (%) |
| Alcohol-related | 121 | 47.8% |
| Hepatitis B | 63 | 24.9% |
| Hepatitis C | 34 | 13.4% |
| NAFLD | 22 | 8.7% |
| Others (autoimmune, genetic, drug induced, etc.) | 13 | 5.1% |
| VBG Parameter | CTP A (n=72) | CTP B (n=97) | CTP C (n=84) | p-value |
| pH | 7.35 ± 0.04 | 7.28 ± 0.06 | 7.21 ± 0.09 | <0.001 |
| HCO₃⁻ (mmol/L) | 22.4 ± 2.8 | 19.1 ± 3.2 | 16.3 ± 4.1 | |
| Lactate (mmol/L) | 1.8 ± 0.6 | 3.2 ± 1.1 | 4.9 ± 1.7 |
| Parameter | Pearson’s R | P-value |
| pH | - 0.76 | <0.001 |
| HCO₃⁻ | 0.71 | |
| Lactate | 0.82 |
| Parameter | With HE (n=89) | Without HE (n=164) | P-value |
| pH | 7.24 ± 0.08 | 7.33 ± 0.05 | <0.001 |
| Lactate (mmol/L) | 4.3 ± 1.5 | 2.1 ± 0.9 | <0.001 |
| Ascites Severity | pH | Lactate (mmol/L) | p-value |
| None (n=92) | 7.34 ± 0.05 | 2.0 ± 0.8 | <0.001 |
| Mild (n=77) | 7.29 ± 0.06 | 3.1 ± 1.0 | <0.001 |
| Moderate/Severe (n=84) | 7.20 ± 0.08 | 4.6 ± 1.5 | <0.001 |
| Parameter | Odds Ratio | 95% CI | p-value |
| pH <7.25 | 4.8 | 2.6–8.9 | <0.001 |
| Lactate >4.5 mmol/L | 6.2 | 3.4–11.3 | <0.001 |
| HCO₃⁻ <18 mmol/L | 3.1 | 1.7–5.6 | 0.002 |
| Parameter | AUC (95% CI) | Cutoff Value | Sensitivity | Specificity | p-value |
| Lactate (mmol/L) | 0.89 (0.84–0.94) | >4.5 | 82.1% | 88.2% | <0.001 |
| pH | 0.85 (0.79–0.91) | <7.25 | 75.5% | 83.3% | <0.001 |
| HCO₃⁻ (mmol/L) | 0.78 (0.71–0.85) | <18 | 69.4% | 74.5% | <0.001 |
| pCO₂ (mmHg) | 0.67 (0.59–0.75) | >45 | 58.2% | 65.1% | 0.002 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal function and acid-base balance · Liver Disease Diagnosis and Treatment · Liver Disease and Transplantation
Introduction
Arterial blood gases (ABG) testing is commonly used to determine oxygenation and acid-base status, but is associated with rare but serious complications such as infections, bleeding, nerve injury, vascular injury, and limb loss. Multiple studies have looked at the venous blood gas (VBG) as a less invasive alternative for routine monitoring of acid-base status, especially in the coagulopathy scenario like chronic liver disease [1, 2]. Portal and splanchnic complications to chronic liver disease, along with complications relating to the systemic and pulmonary circulation, affect the prognosis of the patient as part of a multi-organ syndrome. Splanchnic vasodilatation in relation to portal hypertension is responsible for the hyperdynamic circulation and abnormal distribution of blood volume. Due to splanchnic pooling of blood, there is a reduced “effective arterial blood volume” and activation of baroreceptor and volume-receptor reflexes as the outcome. The enhanced vasodilatation and counterregulatory overactivity of vasoconstrictor systems play major roles in the development of the multi-organ failure in cirrhosis with impaired function and perfusion of kidneys, lungs, brain, skin, and muscles. Blood gas analysis is considered essential to reach the final diagnosis, decide the adequate treatment, and monitor its effectiveness in the management of the patients. It is beneficial to study the hepatic role in the maintenance of acid-base homeostasis and also the effects of acute or chronic hepatic disease on the acid-base disturbances. In clinical application and practice, physicians managing patients with acute or chronic hepatic cell failure should suspect the possibility of the existence of lung-kidney-liver cross-talk. Accurate interpretation of acid-base balance is not possible without thorough assessment and detection of respiratory gas exchange. The interrelationship between pulmonary and hepatic disease is, actually, well known. Ventilation perfusion mismatching, alveolar capillary oxygen disequilibrium, or intrapulmonary or extrapulmonary shunting, or a combination of all of these, is found [3]. As chronic liver diseases and cirrhosis progress gradually, blood oxygenation may also decline over time. The occurrence of ABG alterations and hypoxemia in patients with chronic liver disease significantly influences clinical decision-making and management strategies [4].
Materials and methods
A hospital-based observational, cross-sectional study was conducted in the Department of General Medicine at Sarojini Naidu Medical College, a tertiary care hospital in Agra (Uttar Pradesh), India, from March 2023 to January 2025. A total of 253 patients over 18 years of age who have chronic liver disease have been enrolled after obtaining informed consent. The risk, benefit, and purpose of the study were explained to all of them in their language. Participants were given the opportunity to ask questions and withdraw from the study at any time.
Ethical approval was received from the institutional ethics committee (SNMC/IEC/DHR/2025/103) of Sarojini Naidu Medical College. Confidentiality of the patients was maintained. Patients having evidence of sepsis, respiratory disease, or chronic kidney disease or those with a denial for consent were excluded from the study.
Patients were assessed through detailed history, examination, and investigations like liver function tests, coagulation profiles, viral markers (hepatitis B and C, HIV), and imaging when necessary.
Venous blood samples were collected using a heparinized 1 ml syringe under all aseptic precautions. Analysis was done using the ABL 800 FLEX blood gas analyzer and a specific calibration solution immediately after sample collection. The VBG (venous blood gases) parameters included pH, partial pressure of carbon dioxide (pCO2), partial pressure of oxygen (pO2), bicarbonates (HCO3-), base excess, and serum lactates.
Disease severity was evaluated with the Child-Turcotte-Pugh scoring system, classifying the patients into CTP Class A, B, and C. Outcomes, including complications, hospital stay, and mortality, were analyzed.
Data were entered in Microsoft Excel and analyzed using SPSS software version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics (mean, SD, frequency, and percentage) were used for baseline characteristics. Correlation analysis (Pearson/Spearman) assessed relationships between VBG values and CTP scores. Comparative analysis (t-test, ANOVA, Mann-Whitney U test) compared VBG values across CTP classes. Multivariate logistic regression identified independent predictors of poor outcome and mortality. A p-value <0.05 was considered statistically significant (at 95% confidence interval).
Table 1 and Table 2 show the distribution of study subjects according to demography and etiology, respectively.
Out of the total study participants (N=253), 36.75% were female (93) and 63.25% were male (160). In terms of education, 41.67% of participants had primary education (103), 34.87% were illiterate (87), and 25% had secondary education (63). Regarding socioeconomic status, 32.40% of participants belonged to the lower middle class (81), 29.20% to the middle class (73), 17.60% to the lower class (44), 16.80% to the upper middle class (42), and 5.20% to the upper class (13).
Out of the total study participants (N=253), 47.8% had alcohol-related chronic liver disease, 24.9% had hepatitis B, 13.4% had hepatitis C, 8.7% had nonalcoholic fatty liver disease (NAFLD), and 5.1% had other etiologies like autoimmune, genetic causes, etc.
Results
Table 3 and Figure 1 illustrate the VBG parameters across the various CTP classes, showing that out of the total study participants, 72 were classified as CTP A, 97 as CTP B, and 84 as CTP C. The pH levels were significantly different across the groups, with CTP A having a pH of 7.35 ± 0.04, CTP B 7.28 ± 0.06, and CTP C 7.21 ± 0.09, with a p-value of <0.001. HCO₃⁻ levels were highest in CTP A at 22.4 ± 2.8 mmol/L, followed by 19.1 ± 3.2 mmol/L in CTP B, and lowest in CTP C with 16.3 ± 4.1 mmol/L. Lactate levels also increased across the groups, from 1.8 ± 0.6 mmol/L in CTP A to 3.2 ± 1.1 mmol/L in CTP B and 4.9 ± 1.7 mmol/L in CTP C.
VBG Parameters Across CTP Classes (N= 253)VBG: Venous blood gases; CTP: Child-Turcotte-Pugh score
Table 4 shows the correlation between VBG parameters and the CTP score. pH had a Pearson’s r value of 0.76 with a p-value of <0.001, indicating a strong positive correlation. HCO₃⁻ and lactate also demonstrated positive correlations with the CTP score, with Pearson’s r values of 0.76, 0.71, and 0.82, respectively.
Table 5 shows VBG parameters in patients with vs. without hepatic encephalopathy. Among the study participants, 89 had hepatic encephalopathy (HE) and 164 did not. The pH level in patients with HE was 7.24 ± 0.08, while in those without HE, it was 7.33 ± 0.05, with a significant difference (p < 0.001). The lactate level in patients with HE was 4.3 ± 1.5 mmol/L, compared to 2.1 ± 0.9 mmol/L in patients without HE, also showing a significant difference (p < 0.001).
Table 6 shows the impact of ascites on VBG parameters among the study participants. Out of the total study participants, 92 had no ascites, 77 had mild ascites, and 84 had moderate/severe ascites. It shows that participants with no ascites had a pH of 7.34 ± 0.05 and lactate levels of 2.0 ± 0.8, while those with mild ascites had a pH of 7.29 ± 0.06 and lactate levels of 3.1 ± 1.0. Participants with moderate/severe ascites had a pH of 7.20 ± 0.08 and lactate levels of 4.6 ± 1.5. The p-value indicates a significant difference in the parameters across the groups.
Table 7 shows the VBG parameters as predictors of mortality (logistic regression). Among the study participants, a pH level below 7.25 was linked to a 4.8 times higher chance of death (95% CI: 2.6-8.9, p < 0.001), a lactate level above 4.5 mmol/L was linked to a 6.2 times higher chance of death (95% CI: 3.4-11.3, p < 0.001), and a bicarbonate level below 18 mmol/L was linked to a 3.1 times higher chance of death (95% CI: 1.7-5.6, p = 0.002), all of which were important indicators of mortality.
Table 8 shows the prognostic performance of VBG parameters (ROC analysis). Out of the total study participants, the lactate parameter demonstrated the highest prognostic performance with an AUC of 0.89 (95% CI: 0.84-0.94), a sensitivity of 82.1%, and a specificity of 88.2%. The cutoff value for lactate was >4.5, and the p-value was less than 0.001. The pH parameter followed with an AUC of 0.85 (95% CI: 0.79-0.91), a sensitivity of 75.5%, and specificity of 83.3%, with a cutoff value of <7.25 and a p-value of less than 0.001. HCO₃⁻ showed an AUC of 0.78 (95% CI: 0.71-0.85), with a sensitivity of 69.4%, specificity of 74.5%, and a cutoff value of <18, with a p-value also less than 0.001. Lastly, the pCO₂ parameter had the lowest AUC at 0.67 (95% CI: 0.59-0.75), with a sensitivity of 58.2%, specificity of 65.1%, and a cutoff value of >45, with a p-value of 0.002.
Discussion
Regarding the venous blood gas (VBG) parameters across CTP classes, our study revealed that the pH decreased progressively from CTP A (7.35 ± 0.04) to CTP B (7.28 ± 0.06) and CTP C (7.21 ± 0.09), with a highly significant p-value (<0.001). HCO₃⁻ declined from 22.4 ± 2.8 mmol/L (CTP A) to 19.1 ± 3.2 mmol/L (CTP B) and further to 16.3 ± 4.1 mmol/L (CTP C). Similarly, lactate levels increased from 1.8 ± 0.6 mmol/L in CTP A to 3.2 ± 1.1 mmol/L in CTP B and 4.9 ± 1.7 mmol/L in CTP C. However, no significant correlation was observed for pCO₂ levels in ABG due to chronic lung disease (CLD), suggesting that pCO₂ may not be a reliable indicator for assessing CLD in these patients [5-7]. In terms of correlation between VBG parameters and CTP score, our findings revealed a strong correlation with pH showing r = 0.76 (p < 0.001), pCO₂ r = 0.68, HCO₃ r = 0.71, and lactate r = 0.82 [8].
In the present study, the venous blood gas (VBG) parameters between patients with and without hepatic encephalopathy showed marked differences. Patients with HE had a significantly lower pH (7.24 ± 0.08) and higher lactate levels (4.3 ± 1.5 mmol/L) compared to non-HE patients, who had a pH of 7.33 ± 0.05 and lactate of 2.1 ± 0.9 mmol/L with p-values <0.001 [5]. The present study showed that as ascites severity increased, pH declined and lactate rose [8]. The present study highlights the logistic regression where pH <7.25 (OR = 4.8), lactate >4.5 mmol/L (OR = 6.2), and HCO₃ < 18 mmol/L (OR = 3.1) were significant predictors of mortality, all with p <0.01 [8].
In the present study, comparison of VBG in survivors vs. non-survivors: Among the study participants in our study, the mean pH value in survivors was 7.31 ± 0.06, while in non-survivors, it was significantly lower at 7.18 ± 0.09 (p < 0.001) [8]. Lactate levels in survivors were 2.4 ± 1.1 mmol/L, whereas non-survivors showed elevated levels of 4.8 ± 1.6 mmol/L (p < 0.001) [7].
Length of hospital stay by lactate levels among the study participants in our study: participants with lactate levels <2.5 mmol/L (n=112) had an average hospital stay of 6.2 ± 2.1 days; those with lactate between 2.5-4.5 mmol/L (n=95) stayed for 9.5 ± 3.3 days; and individuals with lactate >4.5 mmol/L (n=46) stayed the longest at 14.8 ± 5.6 days. The p-value was <0.001, indicating strong statistical significance [6, 8].
The present study illustrates ROC analysis where lactate had the highest AUC of 0.89, sensitivity of 82.1%, specificity of 88.2%, and a cutoff of >4.5. pH had AUC of 0.85, sensitivity of 75.5%, and specificity of 83.3% with a cutoff <7.25. HCO3 and pCO2 had lower prognostic value [8]. The present study reveals that in multivariate analysis, CTP class C had an adjusted HR of 5.3 (p<0.001), lactate >4.5 mmol/L had HR 7.1 (p<0.001), pH <7.25 had HR 3.9 (p=0.001), and lower socioeconomic status had HR 2.5 (p=0.008). These values reflect significant independent associations with mortality [8].
This study highlights the prognostic value of venous blood gas (VBG) analysis in chronic liver disease (CLD) but has several limitations. Its cross-sectional design limits causal inference, and the lack of long-term follow-up may underestimate outcomes. Reliance on the static Child-Turcotte-Pugh (CTP) score and exclusion of arterial blood gas (ABG) analysis or metabolic markers may reduce accuracy. The single-center setting and exclusion of patients with common comorbidities limit generalizability. Technical variability in VBG measurements and a modest sample size further constrain findings. Future multicenter, longitudinal studies with broader inclusion and ABG comparison are recommended for validation.
Conclusions
Based on the findings of this study, venous blood gas (VBG) analysis should be integrated into the routine assessment of patients with chronic liver disease (CLD), particularly those classified as Child-Turcotte-Pugh (CTP) B or C, given its strong prognostic value. Parameters such as pH, lactate, and HCO₃⁻ demonstrated significant correlations with disease severity and mortality, with lactate >4.5 mmol/L and pH <7.25 emerging as critical thresholds for poor outcomes. However, the value of venous blood pCO2 was not found to be significant in this study, showing its shortcoming with respect to ABG (arterial blood gases). These markers should be used for early risk stratification, enabling timely interventions in high-risk patients, such as those with hepatic encephalopathy (HE) or severe ascites, where metabolic acidosis and hyperlactatemia were pronounced. Overall, the study highlights the utility of VBG as a simple, cost-effective tool and equally useful as ABG for prognostication and clinical decision-making in chronic liver disease, with the potential to enhance patient outcomes through early risk identification and tailored management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The accuracy of the central venous blood gas for acid-base monitoring J Intensive Care Med Walkey AJ Farber HW O'Donnell C Cabral H Eagan JS Philippides GJ 1041102520102001860710.1177/0885066609356164 · doi ↗ · pubmed ↗
- 2International Liver Transplant Society practice guidelines: diagnosis and management of hepatopulmonary syndrome and portopulmonary hypertension Transplantation Krowka MJ Fallon MB Kawut SM 1440145210020162732681010.1097/TP.0000000000001229 · doi ↗ · pubmed ↗
- 3Lung injury and its prognostic significance in acute liver failure Crit Care Med Audimoolam VK Mc Phail MJ Wendon JA Willars C Bernal W Desai SR Auzinger G 5926004220142415258910.1097/01.ccm.0000435666.15070.d 5 · doi ↗ · pubmed ↗
- 4Study of arterial blood gases in different stages of chronic liver diseases J Med Scientific Res Elfaizy MW Ghatas TS 2352022
- 5Correlation and agreement between arterial and venous blood gas analysis in patients with hypotension-an emergency department-based cross-sectional study Int J Emerg Med Prasad H Vempalli N Agrawal N 181620233689929710.1186/s 12245-023-00486-0PMC 9999648 · doi ↗ · pubmed ↗
- 6Clinical characteristics, etiology, and prognostic scores in patients with acute decompensated liver cirrhosis J Clin Med Al Kaabi H Al Alawi AM Al Falahi Z Al-Naamani Z Al Busafi SA 57561220233768582210.3390/jcm 12175756 PMC 10488876 · doi ↗ · pubmed ↗
- 7Oxidative stress as one of the pathogenetic mechanisms of hepatopulmonary syndrome in patients with liver cirrhosis Gastroenterology Faiura OP Tolopko SY Abrahamovych MY Ferko MR Bilous ZO Guta SI Abrahamovych OO 3943582024
- 8Pulmonary dysfunction in patients with cirrhosis of the liver: a study of pulmonary function tests and arterial blood gases Int J Appl Basic Med Res Vaishnav B Barla DR Ruchitha P Wadivkar AN Tonde T Mondkar S 48531420243850484210.4103/ijabmr.ijabmr_367_23PMC 10947758 · doi ↗ · pubmed ↗