When One Stomach Bug Is Not Enough: A Five-Pathogen Gastroenteritis Case Study
Erick A Boldt, Emma Newquist, Lily D Rundquist, Daniel Pacciulli, Victoria Echevarria, Tianna Nelson, Azjaah Rogers, Tye Barber

TL;DR
A 23-year-old man developed severe gastroenteritis from five different pathogens after a trip to Peru, highlighting the need for thorough testing in similar cases.
Contribution
This case study reports a rare polymicrobial gastroenteritis involving five pathogens from a single travel-related exposure.
Findings
Stool PCR testing identified five pathogens: Plesiomonas shigelloides, EAEC, EPEC, EIEC, and norovirus.
The patient's symptoms resolved with intravenous fluids and antibiotics after two days of care.
The case underscores the importance of comprehensive diagnostic testing for travelers with severe gastroenteritis.
Abstract
Foodborne infections are a common cause of gastroenteritis, but cases involving multiple enteric pathogens from a single exposure are rarely reported. We present the case of a healthy 23-year-old male with no significant chronic medical history who developed febrile gastroenteritis after returning from a four-day solo trip to Peru. His symptoms began one day after returning and included fever, fatigue, nausea, vomiting, watery diarrhea, frontal headaches, and severe neck pain. His history was notable for a herniated disc from a motor vehicle collision (MVC) four months prior, for which he was undergoing physical therapy, raising initial concerns for a non-infectious cause of his neck pain. Initial workup revealed leukocytosis, tachycardia, acute kidney injury (AKI), and imaging concerning for a possible small bowel obstruction. Stool polymerase chain reaction (PCR) testing detected…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
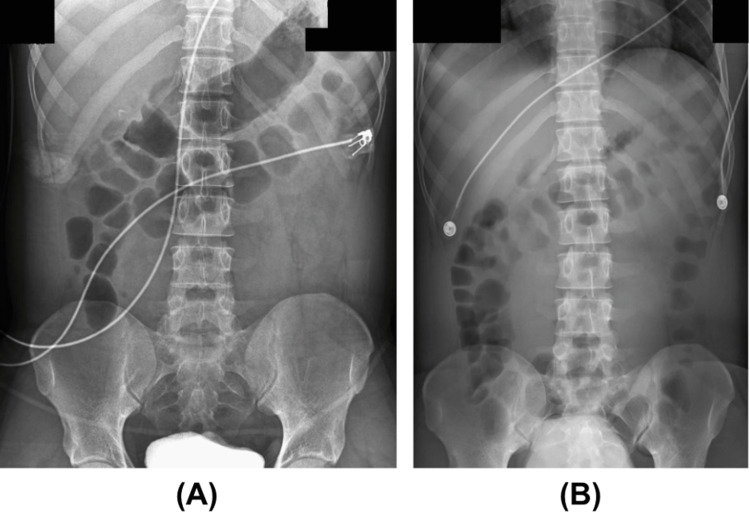 Figure 1
Figure 1| Gastrointestinal Panel | Results |
| Plesiomonas shigelloides | Detected |
| Salmonella | Not detected |
| Vibrio PCR, Vibrio cholerae | Not detected |
| Campylobacter PCR | Not detected |
| Yersinia eneterocolitica | Not detected |
| EAEC | Detected |
| EPEC | Detected |
| ETEC | Not detected |
| Shiga-like-toxin producing E. coli (STEC) | Not detected |
| E. coli O157 | Not detected |
| Shigella/EIEC | Detected |
| Cryptosporidium, Giardia Lamblia, Cyclospora Cayetanensis, Entamoeba histolytica | Not detected |
| Adenovirus F 40/41, Astrovirus, Rotavirus, Sapovirus PCR | Not detected |
| Norovirus | Detected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Clostridium difficile and Clostridium perfringens research · Escherichia coli research studies
Introduction
Acute gastroenteritis (AGE) is a significant global health concern and contributes to an estimated 1.3 million deaths globally per year. In the United States alone, AGE accounts for approximately 179 million cases and one million hospitalizations each year [1]. It typically presents with diarrhea, vomiting, fever, and abdominal pain that lasts for less than a week. While viral pathogens, particularly norovirus, are the most common culprits of epidemic diarrheal disease, bacterial and parasitic co-infections also play a considerable role, especially in foodborne outbreaks and travel-related illnesses [2,3].
A study by Mannstadt et al. examined the prevalence of single versus multiple pathogen infections in gastroenteritis and their association with immunosuppression. They found that approximately 73% of cases involved a single pathogen, while 27% had multiple pathogens, making diagnosis and management more complex [4]. It is hypothesized that multiple pathogen gastroenteritis may occur due to various factors, including impaired host immunity that reduces the body's ability to clear infections, as well as high-risk settings where diverse pathogens circulate, such as international travel or hospitalization [4].
Among the bacterial pathogens mentioned in our patient’s case presentation, enteroaggregative *E. coli *(EAEC) is increasingly recognized as a cause of both acute and chronic watery diarrhea in diverse regions [5]. Enteropathogenic *E. coli *(EPEC) remains a leading cause of diarrheal illness in infants and young children, particularly in resource-limited settings [5]. Plesiomonas shigelloides, with antigenic similarities to Shigella sonnei, is most often reported in Southeast Asia and Africa, with limited reports from other continents [6,7]. Additionally, enteroinvasive E. coli (EIEC) is relatively uncommon due to the requirement of a large inoculum to cause infection [5].
Given the high burden of AGE and its foodborne transmission pathways, understanding the impact of multi-pathogen infections is critical for improving diagnostic accuracy and treatment strategies. This case study explores a complex presentation of AGE in a patient with five enteric pathogens, highlighting the clinical course and management challenges associated with multi-pathogen diarrheal illness and encouraging the necessity for practicing proper food and water safety precautions when traveling.
Case presentation
In March 2025, a 23-year-old previously healthy male presented to the emergency department with fever, fatigue, and gastrointestinal symptoms. His symptoms began one day after returning from a four-day solo trip to Peru, during which he consumed ceviche, raw shellfish, and unfiltered sink water. He initially developed chills, generalized weakness, and nausea, followed by a single episode of green, large-volume emesis and three episodes of watery, non‑bloody, non‑foul‑smelling diarrhea. He also reported intermittent frontal headaches and worsening severe neck pain, which he described as worse than his usual discomfort from a motor vehicle collision (MVC) four months prior, for which he was undergoing physical therapy. He denied any visual disturbances, photophobia, dysuria, or upper respiratory symptoms.
His medical history was also notable for mild, intermittent asthma. There was no previous history of chronic gastrointestinal disease. He did not take daily medications aside from occasional acetaminophen. There were no reports of tobacco or illicit drug use; however, he did admit to drinking alcohol occasionally. He denied any new sexual partners or history of sexually transmitted infections. Family history was unremarkable for gastrointestinal or infectious diseases.
On arrival, he was febrile (39.5 °C/103.1 °F), tachycardic (HR 121 bpm), and tachypneic (RR 27 bpm), with an elevated blood pressure (158/77 mmHg). He appeared mildly distressed but was alert and oriented. His physical examination revealed dry mucous membranes, no overt abdominal tenderness, and no hepatosplenomegaly. His lung and cardiac exams were unremarkable. Given his fever, headache, and neck pain, a neurological exam was performed, which showed full strength, no focal deficits, and negative Kernig and Brudzinski signs, making meningitis less likely.
Initial laboratory workup showed a leukocytosis of 12,140 cells per µL of blood (normal rage: 4,000-11,000 cells per µL of blood), lactate of 4.8 mmol/L (normal range: 0.5-2.2 mmol/L), acute kidney injury (AKI) with a creatinine level of 1.4 mg/dL (normal range: 0.8-1.2 mg/dL), and an abdominal radiograph suggested possible small bowel obstruction (SBO) with recommendations to repeat the following morning (Figure 1A). A stool polymerase chain reaction (PCR) panel (Table 1) later revealed multiple enteric pathogens, including Plesiomonas shigelloides, EAEC, EPEC, EIEC, and norovirus.
Abdominal X-rays demonstrating evolution of suspected small bowel obstruction (SBO).(A) An abdominal X-ray on the day of admission was significant for a possible SBO due to the presence of dilated small bowel. (B) A repeat abdominal X-ray on hospital day two without significant small bowel dilation signified that the patient did not have an SBO during this admission.
Given his septic presentation, empiric broad‑spectrum coverage with intravenous ceftriaxone (1 g in sodium chloride 0.9% 50 mL, every 24 hours) and metronidazole (500 mg, every 12 hours) was initiated within the first hour in accordance with our emergency department sepsis protocol and the Infectious Diseases Society of America (IDSA) guidelines for presumed community‑acquired intra‑abdominal infection; therapy was discontinued once stool PCR and blood cultures excluded invasive bacterial pathogens. Since the patient was immunocompetent and without comorbidities that could negatively impact his recovery, the patient’s symptoms were treated with fluid resuscitation and conservative management. Additionally, all positively identified microbes were self-limiting, rendering further medical management unnecessary. A repeat abdominal x-ray on day two was negative for SBO (Figure 1B). On hospital day three, he remained afebrile, tolerated oral intake, and had resolution of nausea and headache, though he continued to have mild non-bloody diarrhea. He was discharged home in stable condition with instructions for continued hydration and monitoring for worsening symptoms.
Discussion
Though travel-related gastroenteritis is usually attributed to a single pathogen, this case highlights the risk for a polymicrobial enteric infection while traveling to endemic regions. The labs and cultures obtained from our patient were significant for P. shigelloides, EAEC, EPEC, EIEC, and norovirus, indicating that there was extensive pathogen exposure that originated from contaminated food or water.
During his four-day trip to Peru, our patient said to have consumed ceviche, raw shellfish, and unfiltered sink water. P. shigelloides is a waterborne pathogen associated with consumption of raw seafood and untreated water, both of which were part of the patient’s dietary history [6]. The pathogens EAEC and EPEC are both well-documented causes of traveler’s diarrhea. The co-detection of these further supports a foodborne etiology, and both may have been acquired from contaminated water. Moreover, EIEC is a relatively uncommon cause of enteric infection and requires higher infectious doses to be symptomatic, suggesting the patient was exposed to a substantial microbial load [8]. Finally, norovirus is a highly contagious viral pathogen. Its detection adds to the complexity of his clinical presentation as it can exacerbate symptoms and may contribute to prolonged illness [9]. Overall, the identification of these five distinct pathogens emphasizes the severe and unintended repercussions of consuming unfiltered water and ingesting raw or undercooked foods while traveling abroad, particularly outside the United States.
Retrospective studies support the rarity of this finding. For example, Mannstadt et al. analyzed gastrointestinal PCR panels and found that while 27% of patients had multiple pathogens, fewer than 3% had more than three, and most of those patients were immunocompromised [4]. In contrast, our patient was young and healthy and had no history of chronic illness or immunodeficiency. His exposure history likely contributed to a high inoculum of enteric pathogens, resulting in a rare, compounded infection.
In addition, this case further points out the necessity of a comprehensive workup for travel-related enteric infections. As demonstrated in our patient, a thorough diagnostic approach, including PCR testing, was essential to accurately identify pathogens to guide appropriate management. Healthcare practitioners should maintain a high index of suspicion for polymicrobial infections in patients with a history of recent travel with severe or prolonged gastroenteritis, as having multiple infections can potentially complicate diagnosis and treatment.
Furthermore, our patient’s presentation is particularly apparent given that the patient was a young and healthy individual with no underlying medical conditions or immunocompromising factors. Despite his competent immune system, he still contracted multiple enteric infections on a short four-day trip. It is important to recognize that anyone, regardless of their overall health status, can be susceptible to contracting enteric infections when exposed to contaminated food or water. Though immunocompromised individuals may face more severe outcomes, even those with fully functioning immune systems are still at risk for foodborne illnesses and severe polymicrobial infections. Fortunately, in this case, the patient required only supportive care, highlighting the resilience of a healthy immune system in overcoming such infections.
Conclusions
This case demonstrates the high possibility for severe polymicrobial gastroenteritis following short-term international travel despite immunocompetency. It also highlights the need for heightened caution in food selection and hygiene practices. Given the patient’s history and clinical presentation, the presence of five distinct enteric pathogens was most likely contracted from consumption of raw seafood and unfiltered water despite his young age and healthy immune status. Healthcare providers should ensure that travelers are well informed about preventive measures, including avoiding raw or undercooked foods, drinking only safe water sources, and practicing good hand hygiene. Our patient’s clinical presentation is a reminder that, while travel can offer enriching experiences, it also comes with inherent risks. Maintaining appropriate pre-travel education and post-travel workup can help reduce the risk of severe polymicrobial gastrointestinal infections, ultimately leading to improved outcomes for individuals experiencing travel-related illnesses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence, etiology, and severity of acute gastroenteritis among prospectively enrolled patients in 4 veterans affairs hospitals and outpatient centers, 2016-2018 Clin Infect Dis Cardemil CV Balachandran N Kambhampati A 03873202110.1093/cid/ciaa 806PMC 919549632584956 · doi ↗ · pubmed ↗
- 2Acute bacterial gastroenteritis Gastroenterol Clin North Am Fleckenstein JM Matthew Kuhlmann F Sheikh A 2833045020213402444210.1016/j.gtc.2021.02.002PMC 8793005 · doi ↗ · pubmed ↗
- 3Viral gastroenteritis Stat Pearls Stuempfig ND Tobin EH Seroy J Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 518995/30085537 · pubmed ↗
- 4Risk factors and clinical outcomes associated with multiple as opposed to single pathogens detected on the gastrointestinal disease polymerase chain reaction assay Gut Pathog Mannstadt I Choy AM Li J Green DA Freedberg DE 451620243921537310.1186/s 13099-024-00638-4PMC 11365154 · doi ↗ · pubmed ↗
- 5Escherichia coli infection Stat Pearls Mueller M Tainter CR Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 564298/33231968 · pubmed ↗
- 6Plesiomonas shigelloides infections Up To Date 3 2025 Morris JG Horneman A Waltham, MA Up To Date 2023 https://www.uptodate.com/contents/plesiomonas-shigelloides-infections
- 7Plesiomonas shigelloides revisited Clin Microbiol Rev Janda JM Abbott SL Mc Iver CJ 3493742920162696093910.1128/CMR.00103-15PMC 4786884 · doi ↗ · pubmed ↗
- 8Differentiation between Shigella, enteroinvasive Escherichia coli (EIEC) and noninvasive Escherichia coli Eur J Clin Microbiol Infect Dis van den Beld MJ Reubsaet FA 8999043120122190163610.1007/s 10096-011-1395-7 · doi ↗ · pubmed ↗