Intraoperative Bowel Decompression Using an Endo GIA-to-Ultrasound Sleeve Anastomosis: A Novel Approach for Managing Unprepped Sigmoid Volvulus
Brandt Gruizinga, Jonathan Santos, Kevin Szafran, Daniel De Oliveira

TL;DR
This paper introduces a new surgical method to safely decompress the colon during unprepped sigmoid volvulus without contaminating the surgical area.
Contribution
A novel intraoperative technique using a GIA stapler and ultrasound sleeve for bowel decompression is proposed.
Findings
The technique allows fecal evacuation without contaminating the operative field.
A case report demonstrates the feasibility of the method.
Future animal studies are suggested to validate the technique.
Abstract
Acute large bowel obstruction from sigmoid volvulus in unprepped patients presents a significant intraoperative challenge due to the high risk of contamination when decompressing or resecting a distended, feces-filled colon. This paper describes a novel technique for safe and effective decompression of the colon using a linear GIA stapler to create an anastomosis between the descending colon and a sterile ultrasound (US) probe sleeve, enabling fecal evacuation without contamination of the operative field. A case report is presented, and the potential for this technique to be validated through future animal studies is discussed.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
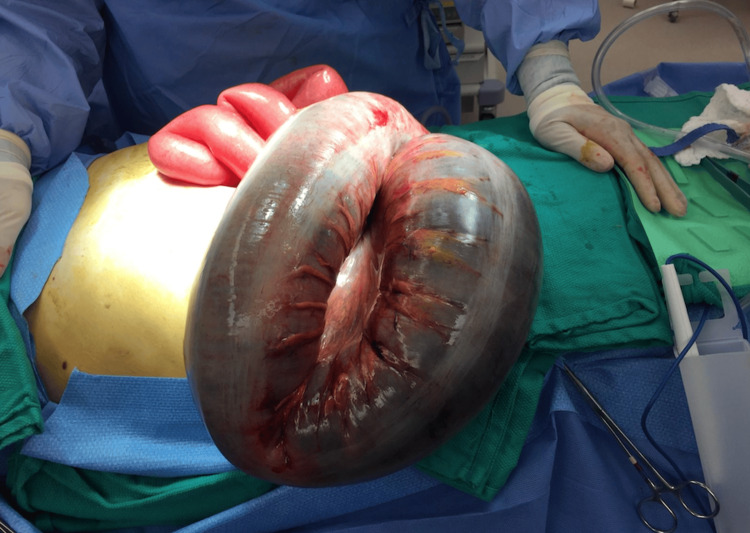 Figure 1
Figure 1 Figure 2
Figure 2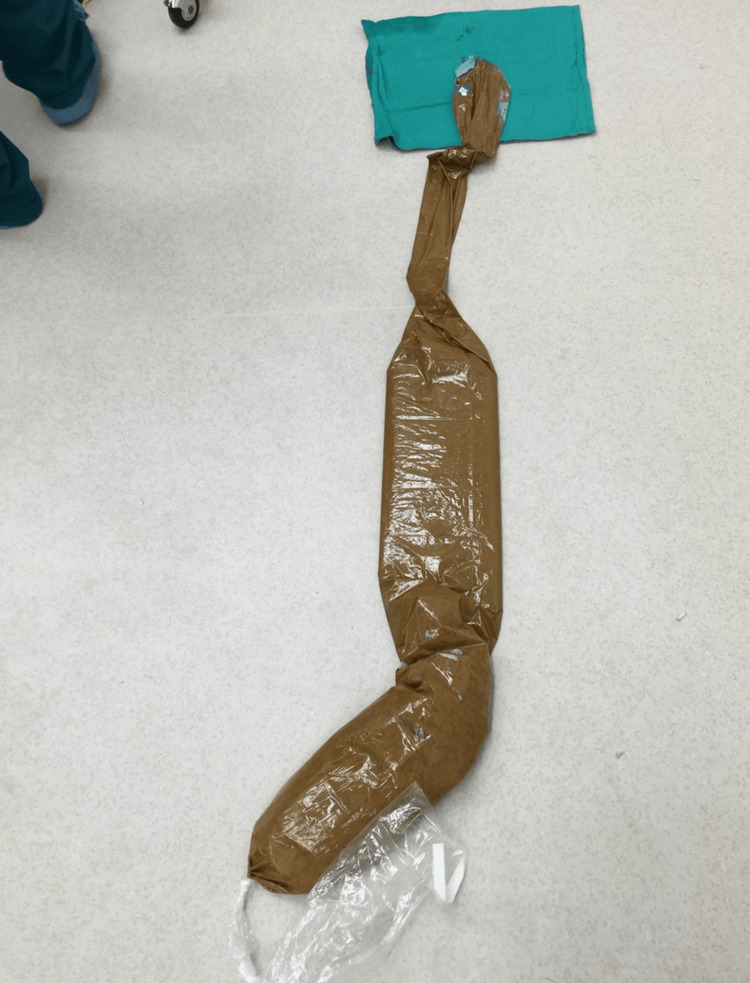 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Intestinal Malrotation and Obstruction Disorders · Esophageal and GI Pathology
Introduction
Sigmoid volvulus is a common cause of large bowel obstruction in elderly populations. In the United States and Western Europe, it accounts for approximately 10-15% of large bowel obstructions. In resource-limited regions, such as parts of Africa, South America, and Asia, it can represent up to 42% of cases [1]. Sigmoid volvulus frequently requires emergency surgical intervention when nonoperative decompression fails or when ischemia or perforation is suspected [2]. In unprepped patients, intraoperative management presents a particular challenge due to the increased risk of fecal contamination during decompression or resection.
Traditional decompression techniques such as manual evacuation, on-table lavage, or enterotomy with suction carry substantial risks of intraoperative spillage and postoperative infectious complications. Surgical site infection (SSI) rates following colorectal surgery range from 5% to 30%, with rates as high as 80% in cases involving perforation [3]. Beyond infection, fecal contamination contributes to significant peritoneal inflammation, which can lead to the development of intra-abdominal adhesions.
Adhesions form in more than 50% of patients following intra-abdominal surgery and are driven by peritoneal trauma and inflammation [4]. Notably, fecal spillage is a major aggravating factor in adhesion formation, as shown by increased rates of adhesion-related readmissions following colorectal procedures [5]. These adhesions can lead to chronic pain, infertility, and recurrent bowel obstructions, creating a self-perpetuating cycle of inflammation, reoperation, and further adhesion formation. Avoiding the initial inflammatory insult of fecal contamination therefore offers the potential for unquantifiable cost savings and improved long-term patient outcomes.
Preserving a sterile operative field is thus essential but technically difficult in the setting of a massively distended colon. In this report, we describe a novel approach using an Endo GIA stapler to create a sealed, side-to-side anastomosis between the descending colon and a sterile ultrasound (US) probe sleeve. This configuration allows for controlled fecal evacuation into a closed system, reducing intraoperative contamination and preserving sterility.
By repurposing familiar surgical tools in an innovative manner, this technique may serve as a safer, reproducible alternative for decompression in emergent colorectal procedures. Further validation through animal models and clinical studies is warranted to assess safety, feasibility, and broader applicability.
Case presentation
Patient information
A male patient in his mid-60s with baseline cognitive impairment and residing in an assisted living facility presented to the emergency department with nausea and vomiting. While his symptoms were initially nonspecific, physical examination revealed a distended, tympanic abdomen with mild diffuse tenderness and no signs of peritonitis. He was hemodynamically stable. A contrast-enhanced CT scan demonstrated a markedly dilated sigmoid colon with mesenteric twisting, consistent with sigmoid volvulus.
Following fluid resuscitation, electrolyte correction, and nasogastric decompression, the decision was made to proceed with an exploratory laparotomy due to concern for complete colonic obstruction. Intraoperatively, a massively distended sigmoid colon with volvulus was confirmed. Given the absence of preoperative bowel preparation, controlled decompression was prioritized to minimize contamination and allow safe resection.
Intraoperative findings
A midline laparotomy revealed a grossly distended sigmoid colon. There was no evidence of ischemia or perforation. The bowel was severely dilated (up to 12 cm in diameter) with thin bowel walls, and the descending colon proximal to the twist was moderately dilated (Figure 1).
Intraoperative image following a midline laparotomy, showing a grossly distended sigmoid colon with severe dilation. No evidence of ischemia or perforation is observed.
Decompression technique
Given the lack of preoperative bowel preparation and the high risk of fecal spillage, decompression in a controlled manner to minimize spillage was paramount. The sigmoid colon was transected distal to the point of torsion using a linear 60 mm Endo GIA purple-load stapler. A second linear stapled side-to-side anastomosis was created between the proximal descending colon and a sterile US probe sleeve, which had been modified and clamped distally to act as a closed fecal conduit (Figure 2).
Intraoperative image showing a side-to-side anastomosis made between the descending colon and a sterile US probe sleeveUS: Ultrasound
Once the stapler fired, immediate decompression was achieved as fecal content flowed into the contained sleeve. Approximately 2 liters of semisolid fecal material was evacuated without contamination of the surgical field. The sleeve was clamped proximally and removed from the field in one motion, preserving sterility (Figure 3).
The sterile US sleeve filled with approximately 2 liters of fecal matter after being removed from the operative fieldUS: Ultrasound
Definitive surgery and colostomy
After complete decompression, the remaining redundant sigmoid colon was resected. A formal end colostomy was constructed in the left lower quadrant. The rectal stump was oversewn and placed in the pelvis. The colostomy was matured with attention to creating a tension-free stoma and securing the mesentery. No intraoperative complications occurred.
Postoperative course and follow-up
The patient had an uneventful postoperative course. He was advanced from clear liquids to a soft diet by postoperative day (POD) 3, with return of bowel function by POD 4. Pain was well controlled with oral analgesics, and he was ambulating independently by POD 2. Laboratory markers remained within normal limits, and no signs of infection or anastomotic complications were observed.
The patient was discharged in stable condition on POD 6 with colostomy education and outpatient follow-up arranged. At his two-week postoperative visit, he reported no complications, and his surgical wounds were healing well.
Discussion
Intraoperative decompression of a distended, unprepped colon remains a major challenge in emergency colorectal surgery. Conventional methods such as manual decompression, suction via enterotomy, or on-table lavage have been associated with increased rates of fecal contamination, which can elevate the risk of postoperative infectious complications, including wound infections and intra-abdominal abscesses, and lead to prolonged recovery and hospital stay [2].
The technique described here offers a novel, controlled approach by creating a side-to-side stapled anastomosis between the colon and a sterile US sleeve. This closed conduit allows for safe evacuation of fecal contents without contaminating the operative field. It uses standard surgical tools in an unconventional but practical way, making it easily adoptable across a range of surgical settings.
The implications of fecal spillage extend beyond infection alone. Contamination can also contribute to the formation of intra-abdominal adhesions, which have been linked to chronic pain, infertility, and future bowel obstructions. A systematic review by ten Broek et al. identified postoperative contamination as a contributing factor to adhesion-related morbidity [6]. More recently, Krielen et al. showed that contamination significantly increases the risk of adhesion-related readmissions following colorectal surgery, reinforcing the long-term burden of even a single intraoperative contamination event [5].
Maintaining sterility is critical, especially in unprepped patients, to reduce complications such as wound infections, intra-abdominal abscesses, and adhesions. This method may also be particularly valuable in resource-limited or high-risk environments, where bowel preparation is not feasible and contamination control is essential. Further studies, including animal models, are warranted to evaluate reproducibility, safety, and broader applications in emergency colorectal care.
Conclusions
Intraoperative bowel decompression using an Endo GIA-to-US sleeve anastomosis offers a safe, sterile, and effective solution for managing unprepped sigmoid volvulus. By minimizing contamination and simplifying fecal evacuation, this technique addresses a critical challenge in emergency colorectal surgery. Its ease of adoption and potential to reduce postoperative complications position it as a promising alternative in high-risk and resource-limited settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WSES consensus guidelines on sigmoid volvulus management World J Emerg Surg Tian BW Vigutto G Tan E 341820233718913410.1186/s 13017-023-00502-x PMC 10186802 · doi ↗ · pubmed ↗
- 2Clinical practice guidelines for colon volvulus and acute colonic pseudo-obstruction Dis Colon Rectum Vogel JD Feingold DL Stewart DB Turner JS Boutros M Chun J Steele SR 5896005920162727051010.1097/DCR.0000000000000602 · doi ↗ · pubmed ↗
- 3Risk factors for surgical site infection in emergency colorectal surgery: a retrospective analysis Surg Infect (Larchmt) Watanabe M Suzuki H Nomura S 2562611520142481080410.1089/sur.2012.154 · doi ↗ · pubmed ↗
- 4Intra-abdominal adhesions: definition, origin, significance in surgical practice, and treatment options Dtsch Arztebl Int Brüggmann D Tchartchian G Wallwiener M Münstedt K Tinneberg HR Hackethal A 7697751072010 https://doi.org/10.3238/arztebl.2010.07692111639610.3238/arztebl.2010.0769 PMC 2992017 · doi ↗ · pubmed ↗
- 5Adhesion-related readmissions after open and laparoscopic colorectal surgery in 16 524 patients Colorectal Dis Krielen P ten Broek RP van Dongen KW Parker MC Griffiths EA van Goor H Stommel MW 5205292420223491976510.1111/codi.16024 · doi ↗ · pubmed ↗
- 6Burden of adhesions in abdominal and pelvic surgery: systematic review and met-analysis BMJ ten Broek RP Issa Y van Santbrink EJ 0347201310.1136/bmj.f 5588 PMC 378958424092941 · doi ↗ · pubmed ↗