Patient lumbar discectomy journey (DiscJourn) in the UK: a qualitative study
Louise White, Nicola R Heneghan, Navin Furtado, Karl Baraks, Zeeshan Parvez, Annabel Masson, Alison B Rushton

TL;DR
This study explores the experiences of UK patients after lumbar discectomy surgery, highlighting their emotional and physical recovery journeys.
Contribution
The study provides new qualitative insights into patient experiences and expectations following lumbar discectomy in the UK.
Findings
Patients expressed high satisfaction and optimism after surgery, with readiness to pursue personal goals.
Post-operative fear and uncertainty were common, driven by concerns about recurrence and long-term impacts.
Personalized rehabilitation and improved communication are needed to address diverse patient needs.
Abstract
To gain insight into patients’ views, perceptions, experiences and expectations postlumbar discectomy. A qualitative study using interpretative phenomenological analysis (IPA) purposively recruited patients undergoing lumbar discectomy at one UK spinal centre. Purposive criteria included age, sex, ethnicity, symptom duration, work/sick leave, education level and co-existing psychological issues. Semi-structured interviews were conducted using a patient co-constructed topic guide. Interview transcriptions were analysed in accordance with IPA. Strategies enhancing trustworthiness included suspension of judgements and presuppositions, reflexivity, iterative coding process and critique from co-investigators. Data from 14 participants (eight elective, 6 emergency surgery) informed four themes. The theme ready to move forwards was characterised by high satisfaction with post-operative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
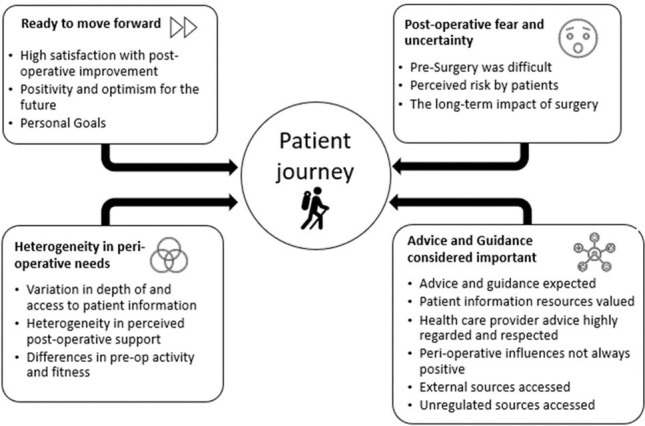 Figure 1
Figure 1| N (%) | ||
|---|---|---|
| Age (years) | 20–35 | 4 (28.6) |
| 36–50 | 6 (42.8) | |
| 50–70 | 3 (21.4) | |
| >70 | 1 (7.1) | |
| Sex | Female | 6 (42.8) |
| Male | 8 (57.2) | |
| Ethnicity | White British | 12 (85.7) |
| British Asian | 2 (14.2) | |
| Level of surgery | L4/5 | 6 (42.8) |
| L5/S1 | 8 (57.2) | |
| Elective or emergency | Elective | 8 (57.2) |
| Emergency | 6 (42.8) | |
| Symptom duration | 0–1 year | 6 (42.8) |
| 1–2 years | 5 (35.7) | |
| >2 years | 3 (21.4) | |
| Employment status | Employed/self-employed | 10 (71.4) |
| Unemployed | 2 (14.2) | |
| Retired | 2 (14.2) | |
| Co-existing past medical history | Depression | 2 (14.2) |
| Panic attacks | 1 (7.1) | |
| Cardiac | 1 (7.1) | |
| Nil | 10 (71.4) |
| Subtheme | Description | Illustrative quotations |
|---|---|---|
| High satisfaction with postoperative improvement | Participants described reduced leg pain, numbness, paraesthesia and/or weakness following surgery. | P1 (Elsurg) |
| Positivity and optimism for the future | Participants reported psychological positivity and optimism for the future; they could see hope to return to “normal life” including activities valued and enjoyed. There was perceived opportunity to improve quality of life with associated motivation and enthusiasm for the future. | P4 (Elsurg) |
| Personal goals | Participants all described how their lives had been restricted because of their symptoms. Returning to meaningful and enjoyable activities was very important and fuelled their drive to achieve personal goals. | P5 (Emsurg) |
| Subtheme | Description | Illustrative quotations |
|---|---|---|
| Pre-surgery was difficult | Participants reflected on presurgery difficulties: | P8 (Elsurg) |
| Perceived risk by patients | Participants voiced fear and uncertainty that their actions could cause regression thus decreasing confidence to self-manage. | P16 (Emsurg) |
| The long-term impact of surgery | Participants described their beliefs and concerns about the impact of surgery and the associated influence on future behaviours aiming to mitigate recurrence or regression. | P15 (Emsurg) |
| Subtheme | Description | Illustrative quotations |
|---|---|---|
| Advice and guidance expected | Participants looked to the Healthcare Team (HCT) to provide the right advice and guidance to support recovery. | P6 (Elsurg) |
| Patient information resources valued | Participants described patient information resources as useful to reinforce the verbal advice provided in face-to-face consultations. | P12 (Emsurg) |
| Healthcare provider advice highly regarded and respected | When unexpected symptom increases were experienced, anxiety of triggering a self-induced setback led to seeking advice and guidance. | P6 (Elsurg) |
| Peri-operative influences not always positive | Participants also described inadvertent advice potentially amplifying negative beliefs and behaviours (eg, restricting and avoidant behaviours). | P4 (Elsurg) |
| External sources accessed | When information and guidance was insufficient to meet needs, external sources were sought (including websites and chat forums). | P15 (Emsurg) |
| Subtheme | Description | Illustrative quotations |
|---|---|---|
| Variation in depth of and access to patient information | Although peri-operative advice and guidance was valued by all there was significant variation in preferred depth and type of delivery of guidance. Some looked for very detailed guidance. | P12 (Emsurg) |
| Heterogeneity in perceived post-operative support | Some participants described satisfaction with only post-operative advice and guidance. | P3 (Emsurg) |
| Differences in pre-op activity and fitness | Participants described wide-ranging pre-surgery activity levels suggesting inevitable differences in fitness. Illustrating the “active pre-op” end of the spectrum, two Emsurg participants experienced sudden deterioration with no major pre-existing symptoms with three Emsurg participants at work on day of admission (P5, P12 and P15). | P15 (Emsurg) |
- —Birmingham Health Partnership
- —National Institute for Health Research (NIHR)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Musculoskeletal pain and rehabilitation · Clinical practice guidelines implementation
Background
Lumbar discectomy is an internationally recognised surgical procedure for discogenic neural compression causing concordant severe or progressive neurological deficits, especially when conservative treatments have been exhausted.1 Discectomy is the most frequent spinal surgical procedure2 with moderate-level evidence of postdiscectomy improved leg pain and disability as well as associated reduced back pain.3 Furthermore, analysis of world-wide patient-rated outcomes revealed 79% excellent-to-good results postdiscectomy,2 consistent with earlier studies where 69%–79% reported ‘good recovery’ 1 year postdiscectomy4 and 78%–95% success at 1–2 years post-op.5 Despite these favourable results, not all patients experience full symptom resolution and functional recovery. A recent study reported 26.3% and 30.6% of participants describing poor improvement in leg and back pain, respectively, postdiscectomy,6 with persistent mild-to-moderate disability after 2–8 years3 and 5 years.7 A systematic review8 revealed widely varying work rates (3%–100%) within 24 months of surgery for radiculopathy and sick leave variation of 0.8–20 weeks. Collectively, findings illustrate significant variation in recovery, which is currently not well understood.
Evidence guiding perioperative management is limited. Systematic reviews identify low/very low-quality evidence demonstrating potential to improve pain and disability,5 movement and physical impairment9 in the short-term with high-intensity rehabilitation exercise programmes commencing 4–6 weeks postsurgery. Also, there is ongoing debate about support that clinicians think patients need and postsurgery activity restrictions.10 Additionally, reports suggest poor quality discectomy patient information with lack of perioperative information contributing to depression and anxiety both before and after surgery11 and such emotions associated with poor surgical results. This is concordant with the wider evidence base, with reports of negative emotions increasing the risk of chronicity and disability12 and psychological processes potentially catalysing the transition from acute to chronic pain. Therefore, exploring the patients’ perspective, in terms of perioperative rehabilitation needs (including exercise, advice, guidance and information expectations) as well as the effect of perioperative support on recovery, requires deeper understanding.
Within the existing evidence base, qualitative studies are rare yet offer in-depth understanding of patients’ experiences and have been associated with the development of high quality, safe and clinically effective care.13 One interview study explored acceptability of outpatient discectomy surgery, finding positive patient experiences including satisfaction with level and quality of perioperative information, but rehabilitation experiences were not included.14 Another semistructured interview study15 reported postoperative movement restrictions due to participants’ high anxiety and fear of re-injury with lack of physiotherapy support to explore optimal activity and functional recovery. However, this study included eight elective patients excluding15 those undergoing emergency surgery, with postoperative focus on physiotherapy rather than considering wider influences on patients’ beliefs and behaviours. Also, a focus group study found differences in management preferences within and between patient and physiotherapist groups,with some patients indicating that ‘advice and guidance only’ was acceptable for them.16 Previous studies5 9 have assumed that all patients need and want intensive postdiscectomy rehabilitation, but there may be some heterogeneity within perioperative needs. Building on existing evidence, the aim of this study was to understand patients’ perspectives and lived experiences of lumbar discectomy surgery.
Objectives
To explore the patient discectomy journey and understand experiences relating to symptomatology and function.
To capture the patients’ perceptions of the need for, value of and adherence to perioperative care and guidance.
To understand the patient journey through return to functional activities and gain insight into barriers and facilitators affecting recovery, similarities and differences between patients/ patient groups (eg, elective vs emergency) and perceptions relating to post-op rehabilitation and recovery.
Methods
Design
A qualitative study employing an Interpretive Phenomenological Analysis (IPA) approach enabled rich exploration of the patient’s experience (phenomenology) combined with making sense of the experience (hermeneutics).17 Study design and data analyses were conducted in partnership with two patient co-investigators according to a published protocol18 reported in line with Standards for Reporting Qualitative Research19 and Consolidated Criteria for Reporting Qualitative Studies.20 A Study Management Group (SMG) including clinical physiotherapists (LW, KB), academic researchers (ABR, NRH), Patient and public involvement (PPI) representative and post-graduate physiotherapy student (ZP) met regularly to oversee study quality.
Participants
A purposive sample of 14 patients (≥16 years) undergoing primary lumbar discectomy surgery (emergency or elective) and able to communicate in English was recruited in one UK secondary care spinal surgery setting. Sampling ensured a range of participant characteristics, such as age, sex, ethnicity, symptom duration, work satisfaction, sick leave duration from work, educational level, co-existing psychological issues and coping strategies. Exclusion criteria included infection, malignancy or previous surgery. Potentially eligible participants were identified (n=22) by neurosurgery team members including hospital Principal Investigator (PI) (LW), surgeons, ward physiotherapists and waiting list coordinators prior to or during admission.
Data collection
Semistructured interviews were arranged and undertaken by the PI (LW), a specialist physiotherapist, between May 2018 and March 2019. Participants were aware of the interviewer’s background with interviews completed at participants’ home or hospital within 3 weeks of surgery. The topic guide (box 1 and online supplemental file 1) was co-constructed drawing on evidence and insights from patient co-investigators. Pilot interviews (n=2) were undertaken to ensure quality of the topic guide and practice, with no changes made. Interviews were audio-recorded and professionally transcribed verbatim.
Box 1Topic Guide sectionsTopic guide sectionsPre- and postoperative experiencesParticipant’s expectations from surgeryUnderlying attitudes and beliefs towards the surgical interventionFacilitators and barriers to recoveryAdherence to advice and physiotherapy; experiences of rehabilitationReturn to previous function, activity and/ or work
Data storage and management
Adherence to the Research Governance and Data Protection Act 2018 included electronic records storage on password-protected computers, preserved and accessible to the research team for 10 years poststudy completion. To maintain participant pseudoanonymity, numbers were used to depersonalise data. Transcribed texts were checked with audio recordings and file notes prior to analysis.
Data analysis
Analysis was undertaken in accordance with IPA.
Stage 1: Interviews transcribed verbatim were combined with interviewer’s observations, reflections and notes.
Stage 2: In accordance with IPA, two investigators (LW and ZP) initially independently immersed themselves in data reading and re-reading transcriptions combined with listening to recordings. Noting included descriptive, linguistic and conceptual comments which were then organised to develop emergent themes.
Stages 3 and 4: The PI (LW) and blind reviewer (ZP) independently grouped emergent themes as clusters and tabulated them in a summary table, illustrated by verbatim extracts. Themes were then presented and discussed with the SMG and checked for consistency and accuracy. The SMG provided critique with discussion to consider a priori concepts throughout the process.
Patient and public involvement
This project involved two patient and public representatives from inception. Both PPI representatives had undergone lumbar discectomy surgery and one contributed to previous lumbar discectomy projects undertaken by the research group. As co-investigators, patient representatives contributed to the interview topic guide, participant information sheets and consent forms. They were integral members of the SMG and therefore in data analysis.
Trustworthiness
Strategies to ensure trustworthiness17 included researchers discussing their preconceived beliefs, knowledge and clinical experience openly and acknowledging potential impact on data. Other strategies included rigorously checking/rechecking data to the level of minor themes with blind coding from two researchers (LW, ZP), regular discussions with SMG and code–recode audits. Coding was an iterative process including collaborative analysis with triangulation of analysis and interpretation through regular discussions with fellow researchers, enabling greater transparency of data discussed within the SMG. This ensured peer and patient critique and review, thus providing professional and PPI perspectives enhancing researcher reflexivity and quality of analysis.
Ethical considerations
Informed consent was sought during admission for surgery. Recruiters had current Good Clinical Practice (GCP) training. Ethical approval was granted by the London-Bloomsbury Research Ethics Committee (18/LO/0459; IRAS 241345). Hospital Research and Development approval was granted.
Findings
Participants
Twenty-two patients were introduced, with six declining participation. Two were excluded as they underwent more extensive surgery. Participants (n=14) included n=8 females, aged 26–76 years (median 51 years). Eight underwent elective surgery (Elsurg) and six emergency surgery (Emsurg) (table 1). Further details of participants are available in online supplemental file 2.
Themes
Four key themes emerged from participants’ experiences during early post-op recovery: ready to move forward, postoperative fear and uncertainty, advice and guidance considered important and heterogeneity in perioperative needs (figure 1).
Themes and subthemes.
Ready to move forward theme
Participants described confidence that surgery had been necessary and the right decision. Physical and psychological improvements were identified and, with surgery behind them, participants were motivated to engage with recovery and ready to move forward with their lives. Three subthemes characterised this theme (table 2).
Post-operative fear and uncertainty theme
Participants described fear and uncertainty experienced concurrently with postoperative positivity. Three subthemes characterise this theme. The difficulties associated with preoperative life fuelled dread of recurrence or relapse with acknowledgement of the holistic negative impact and approximately half the participants reflected that they were not coping presurgery. Subthemes also characterise the implications for how associated beliefs influenced immediate and longer-term future. Furthermore, reflection on presurgical difficulties underpinned concerns that participants could cause setbacks or recurrencies if the ‘right rules’ and restrictions were not followed as well as thoughts and beliefs affecting future behaviours (table 3).
Advice and Guidance considered important theme
This theme was characterised by participants’ descriptions of perioperative advice and guidance expectations and experiences to navigate recovery and optimise outcomes. Overall advice and guidance were considered important with six subthemes characterising this theme (table 4).
Heterogeneity in perioperative needs theme
Although all participants underwent the same surgical procedure, heterogeneity evolved as a theme in relation to participants’ perioperative needs characterised by three subthemes (table 5).
Discussion
This is the first study to explore transition from presurgery through to early post-operative recovery from the patients’ perspective following elective and emergency discectomy. The IPA approach offers new insight into symptoms experienced and effects on all aspects of life, gaining valuable reflections on the surgical journey including barriers, facilitators and perceived support requirements. Findings are concordant with positive outcomes from previous studies identifying physical improvements after discectomy, including reduced leg symptoms and disability,3 and also offers a wider and more holistic perspective.
The ‘ready to move forwards’ theme describes combined postoperative symptomatic and physical improvements with high satisfaction, positive emotions and optimism fuelling motivation towards achieving individual goals. These factors offer a strong platform for rehabilitation and recovery. However, the second theme describes concurrent ‘post-operative fear and uncertainty.’ Fear is an unpleasant emotion in response to perceived or recognised danger or threat; for participants, this is related to the threat of recurrent symptoms, return to difficult presurgery state and uncertainty for the future. These findings are similar to an Italian interview study21 which specifically investigated thoughts and concerns of 28 participants undergoing a range of lumbar surgical procedures (discectomy, decompression and arthrodesis fixation) at point of discharge. Our study focused on discectomy patients with interviews exploring a wider perspective of what was important to patients. However, similar outcomes included reports of unacceptable presurgery disability and lack of normal life as well as postoperative fear of pain recurrences. Our findings were also concordant with a previous interview study15 which described significant fear of pain generation and ‘undoing’ the effects of surgery with associated avoidant behaviours. It is recognised in the wider evidence base that pain-related fear and uncertainty can lead to safety-seeking behaviours potentially adversely affecting normal movement and activity, thus limiting progress with negative emotions and behaviours also associated with increased risk of chronicity and disability.12 Conversely, it has been shown that people who are not threatened by pain will follow recovery-orientated goals, facilitating faster recovery.22
Our third theme, ‘advice and guidance considered important’ describes the opportunity for healthcare providers to address such fears and uncertainties posing potential barriers to progress. Participants reported keenness for advice and guidance to help successfully navigate recovery and gain advice and reassurance when unexpected events and potential setbacks were experienced. These findings align with the Italian interview study,21 which included participants undergoing a range of lumbar operative procedures; although only verbal advice and guidance was provided, participants sought this perisurgical information, and support was valued. Furthermore, in concordance with a previous discectomy study,15 patient information resources were considered useful to enhance and reinforce verbal advice; strong compliance with provided advice and guidance was also reported. These findings highlight how Health Care Professionals (HCPs) are potentially powerful influencers on beliefs and behaviours postsurgery. It is therefore important that HCPs offer high-quality evidence-based perioperative advice, guidance and comprehensive patient information resources to positively influence recovery and challenge unhelpful beliefs and behaviours, thus empowering recovery. Within the non-surgical back pain literature, Darlow found that clinicians could provide reassurance which increased confidence with advice positively influencing the approach to movement and activity23. However, in Theme 3, participants reported incidences of repeated advice potentially fostering unhelpful beliefs and therefore behaviours, thus increasing the risk of developing persistent pain, maladaptive behaviours and limiting recovery. Similar findings were reported in a previous interview study15 focussing on physiotherapy post-operative experience; fear-avoidance behaviours were not challenged with resultant levels of post-operative anxiety described relating to movement and activity restrictions. It is beyond the scope of this study to explore if patient understanding diverged from the HCP intended message and highlights an area for future investigation.
In Theme 3, participants also described value in perioperative patient information resources, with instances of participants searching the internet for additional information and guidance when resources and advice provided did not fully meet their needs. However, Brooks24 analysed Lumbar Discectomy YouTube content against British Association of Spinal Surgeons (BASS) criteria with approximately 50% of content graded poor/inadequate quality. In another study,25 lumbar discectomy patient information available on NHS Trust websites was examined; 47% of identified leaflets contained poor/fair information, with 44% considered good quality and only 3% excellent. The limited evidence base underpinning patient information is a likely contributing factor to the confusing postoperative rehabilitation guidance for clinicians and patients. For example, a previous survey26 reported wide-ranging activity limitations postdiscectomy within UK practice with ongoing debate regarding postdiscectomy restrictions.10 Clearer evidence with international consensus guiding best peridiscectomy practice would facilitate more confident and positive influences on recovery.
While our results support advice and guidance for all, the final theme described ‘heterogeneity in peri-operative needs’. The first subtheme characterises variation in depth of and access to patient information. Two participants described reliance only on verbal guidance from preoperative consultations, but our findings indicate consequent limited understanding of expected progress reducing self-efficacy. There were also differences between emergency and elective surgery patient needs with the former ‘missing’ preoperative preparation. Therefore, ensuring access to comprehensive patient information, especially during and after emergency admission, is recommended, as well as encouragement for patient engagement with resources.
There was also variability in perceived postoperative support; while patient information with minimal postoperative HCP input was adequate for some, others wanted more detailed rehabilitation and guidance. Furthermore, findings demonstrated a spectrum of preoperative activity and functional levels (eg, ranging from asymptomatic and able to work until surgery to others describing prolonged presurgery very sedentary behaviours—see table 1 and Table of Participants online supplemental file). This heterogeneity has not been considered within clinical trials5 9 where discectomy patients have been treated as a homogenous group and potential benefits of post-op rehabilitation explored for all patients. It is therefore postulated that within previous studies, inclusion of those with higher preoperative functioning and postoperative symptom resolution may mask benefits for those who would benefit most. There were indications of transferable skills influencing self-efficacy (eg, one patient with previous history of depression described use of previously acquired cognitive behavioural therapy skills). However, it is beyond the scope of this study to identify subgroups requiring more detailed rehabilitation, but our findings support personalised perioperative management based on identified physical and psychosocial needs.
Strengths and limitations
The use of IPA was a key strength of this study, providing detailed insight from participants. The main author was immersed in the study through data collection and subsequent analysis, although analysis was a collaborative process including researchers, clinicians and patient representatives; this triangulation was a strength. However, there may have been bias as all interviews were completed by the same individual; involving clinicians with different professional backgrounds may have reduced this potential bias. Effort was made to include a representative sample of discectomy patients including those undergoing emergency and elective procedures and wide-ranging backgrounds although none of our participants described dissatisfaction or specifically experienced perioperative complications. Participants were encouraged to freely describe their experiences providing depth of data. All participants underwent surgery within one secondary care NHS Trust, although external validity is a recognised limitation of IPA. The study indicates heterogeneity within patient rehabilitation needs, but it was beyond the scope of this study to identify criteria for those with low versus more intensive rehabilitation need, highlighting an area requiring future research.
Conclusions
The findings highlight the transition from a difficult preoperative state to postsurgery improvement. There was postoperative high satisfaction, positivity and optimism for resuming previously enjoyed activities and improved quality of life. Clinicians have an opportunity to harness patients’ motivation towards achieving personalised goals and to address fears and uncertainties that could inhibit progress or even limit eventual outcomes; our findings demonstrate healthcare professionals’ powerful influence, with participants describing value in HCP input. However, results also suggest scope to improve quality of verbal communication to minimise iatrogenic negative healthcare messages as well as ensuring access to appropriate comprehensive information to support recovery. The final theme indicates that advice and guidance is adequate for some, empowering self-management. However, others require more intensive peri-operative input with results supporting personalised care based on individual biopsychosocial needs. This qualitative study identifies what is important from the patients’ perspective and areas to improve support for those undergoing discectomy towards improving the patient journey as well as optimising outcomes.
Supplementary material
10.1136/bmjopen-2025-101259online supplemental file 1
10.1136/bmjopen-2025-101259online supplemental file 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Greenhough C National back and radicular pain pathway Trauma programme of care: NHS England 2017
- 2Dohrmann GJ Mansour N Long-Term Results of Various Operations for Lumbar Disc Herniation: Analysis of over 39,000 Patients Med Princ Pract 2015242859010.1159/00037549925832729 PMC 5588202 · doi ↗ · pubmed ↗
- 3Rushton A Heneghan NR Heymans MW et al Clinical course of pain and disability following primary lumbar discectomy: systematic review and meta-analysis Eur Spine J 20202916607010.1007/s 00586-019-06272-y 31916000 · doi ↗ · pubmed ↗
- 4Arts MP Brand R van den Akker ME et al Tubular diskectomy vs conventional microdiskectomy for sciatica: a randomized controlled trial JAMA 20093021495810.1001/jama.2009.97219584344 · doi ↗ · pubmed ↗
- 5Oosterhuis T Costa LOP Maher CG et al Rehabilitation after lumbar disc surgery Cochrane Database Syst Rev 20142014 CD 00300710.1002/14651858.CD 003007.pub 324627325 PMC 7138272 · doi ↗ · pubmed ↗
- 6Wang S Hebert JJ Abraham E et al Postoperative recovery patterns following discectomy surgery in patients with lumbar radiculopathy Sci Rep 2022121910.1038/s 41598-022-15169-835778472 PMC 9249755 · doi ↗ · pubmed ↗
- 7Machado GC Witzleb AJ Fritsch C et al Patients with sciatica still experience pain and disability 5 years after surgery: A systematic review with meta-analysis of cohort studies Eur J Pain 2016201700910.1002/ejp.89327172245 · doi ↗ · pubmed ↗
- 8Huysmans E Goudman L Van Belleghem G et al Return to work following surgery for lumbar radiculopathy: a systematic review Spine J 201818169471410.1016/j.spinee.2018.05.03029800705 · doi ↗ · pubmed ↗