Is rotavirus aetiology in young children with acute diarrhoea associated with sociodemographic and clinical factors, including rotavirus vaccination status? A secondary cross-sectional analysis of the ABCD trial
Sarah Somji, Christopher R Sudfeld, Christopher Duggan, Karim Manji, Tahmeed Ahmed, Mohammod Jobayer Chisti, Usha Dhingra, Sunil Sazawal, Benson Singa, Judd L Walson, Patricia B Pavlinac, Naor Bar-Zeev, Eric Houpt, Queen Dube, Karen L Kotloff, Samba O Sow

TL;DR
This study explores whether rotavirus infection in young children with diarrhea is linked to vaccination status, education, and other factors, finding limited associations.
Contribution
The study provides new insights into the limited predictive value of rotavirus vaccination status and socioeconomic factors for rotavirus aetiology in diarrheal disease.
Findings
Rotavirus prevalence was 21.1% among children with diarrhea.
Shorter diarrhea duration was associated with rotavirus aetiology.
Parental secondary education was linked to increased rotavirus prevalence.
Abstract
One of the leading causes of global child mortality continues to be diarrhoea where rotavirus contributed to about 24% of deaths among all diarrhoeal deaths, mostly in low-income and middle-income countries. Rotavirus vaccination programmes have contributed to the reduction of mortality from 24% to 19% in rotavirus infections among hospitalised children, but the burden of rotaviral diarrhoea remains high, especially in settings with undernutrition. We aimed to determine the association of rotaviral diarrhoea aetiology with prior vaccination, socioeconomic status and clinical factors in children to see their utility in clinical settings. We analysed secondary data from a multicentre clinical trial on antibiotic impact in children with diarrhoea and increased risk of mortality. We used stored stool samples of 6697 children aged 2–23 months old, presenting to a health facility with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
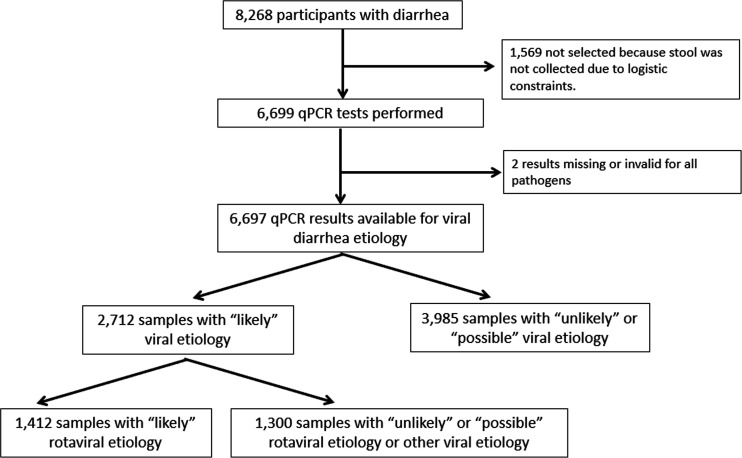 Figure 1
Figure 1| Baseline characteristics | Total | Bangladesh | India | Kenya | Malawi | Mali | Pakistan | Tanzania |
|---|---|---|---|---|---|---|---|---|
| Infant age, months | 11.6 (5.3) | 11.2 (5.0) | 11.9 (5.6) | 11.0 (5.7) | 12.0 (4.8) | 12.0 (4.6) | 12.5 (5.5) | 11.0 (5.2) |
| Male sex | 53.8% | 57.8% | 52.9% | 52.7% | 56.9% | 53.9% | 50.6% | 53.2% |
| Rotavirus vaccination status (any dose >1) | 59.9% | 1.0% | 2.7% | 99.6% | 99.6% | 97.6% | 7.3% | 99.9% |
| Length for age Z score | −1.5 (1.4) | −1.8 (1.2) | −2.1 (1.3) | −0.8 (1.3) | −1.6 (1.5) | −1.2 (1.1) | −2.2 (1.3) | −0.8 (1.1) |
| Weight for length Z score | −1.1 (1.2) | −1.7 (0.9) | −1.4 (1.0) | −0.3 (1.2) | −0.6 (1.2) | −2.0 (0.7) | −1.5 (1.0) | −0.4 (1.3) |
| Exclusive breastfeeding at time of enrolment | 8.7% | 1.7% | 6.9% | 17.9% | 4.1% | 5.4% | 9.2% | 14.4% |
| Maternal education, completed school years | 6 (4) | 5 (3) | 4 (4) | 8 (2) | 8 (2) | 4 (4) | 2 (4) | 7 (2) |
| No maternal education | 26.0% | 18.8% | 38.7% | 0.9% | 0.7% | 51.6% | 59.1% | 4.8% |
| Maternal age, years | 26.0 (5.6) | 24.4 (5.2) | 26.1 (4.4) | 26.0 (5.6) | 25.1 (6.0) | 26.4 (6.2) | 26.8 (5.5) | 27.1 (5.8) |
| Maternal Body Mass Index, kg/m2 | 23.3 (4.7) | 22.3 (4.3) | 22.6 (4.3) | 23.3 (3.8) | 23.1 (5.3) | 24.0 (4.9) | 23.2 (5.0) | 24.5 (5.0) |
| Paternal education, completed school years | 6 (4) | 6 (4) | 5 (4) | 10 (2) | 10 (2) | 4 (5) | 3 (4) | 8 (2) |
| No paternal education | 24.4% | 20.4% | 30.9% | 0.4% | 0.6% | 55.1% | 52.7% | 0.6% |
| Household wealth above median (wealth quintile) | 54.7% | 0.1% | 71.6% | 47.1% | 56.6% | 92.0% | 18.1% | 98.4% |
| Number of children <5 years in the household | 1.7 (1.1) | 1.2 (0.4) | 1.9 (0.9) | 1.7 (0.8) | 1.4 (0.6) | 2.4 (1.8) | 2.0 (1.0) | 1.3 (0.5) |
| Proportion of viral aetiology | 40.5% | 67.2% | 35.0% | 26.4% | 50.7% | 41.0% | 23.3% | 43.2% |
| Proportion of rotavirus aetiology | 21.1% | 47.3% | 15.9% | 11.0% | 28.7% | 24.4% | 11.6% | 11.1% |
| Variable | Rotaviral diarrhoea aetiology | ||||
|---|---|---|---|---|---|
| Prevalence n/N (%) | Unadjusted prevalence ratio (95% CI) | P value | Adjusted | P value | |
| Any dose of rotavirus vaccination | |||||
| No | 647/2491 (25.9%) | Ref. | – | Ref. | – |
| Yes | 656/3724 (17.6%) | 0.61 (0.54, 0.69) | <0.001 | 0.71 (0.49, 1.03) | 0.07 |
| Variable | Rotaviral diarrhoea aetiology | ||
|---|---|---|---|
| Prevalence n/N (%) | Adjusted | P value | |
| Age (in months) | |||
| 2–<6 | 180/967 (18.6%) | Ref. | – |
| 6–<12 | 660/2797 (23.6%) | 1.00 (0.82, 1.24) | 0.93 |
| 12–<18 | 415/1871 (22.2%) | 1.00 (0.80, 1.26) | 0.96 |
| 18–<24 | 157/1057 (14.9%) | 0.84 (0.64, 1.10) | 0.21 |
| Risk-defining criterion | |||
| Severe stunting only | 144/414 (34.8%) | Ref. | – |
| Some/severe dehydration only | 1099/2835 (38.8%) | 1.24 (0.87, 1.77) | 0.24 |
| MAM only | 962/2225 (35.5%) | 1.03 (0.72, 1.48) | 0.88 |
| MAM and some/severe dehydration | 298/626 (47.6%) | 1.44 (0.98, 2.11) | 0.06 |
| MAM and severe stunting | 141/409 (34.5%) | 0.93 (0.57, 1.52) | 0.78 |
| Some/severe dehydration and severe stunting | 31/95 (32.6%) | 1.58 (0.91, 2.73) | 0.10 |
| MAM, some/severe dehydration and severe stunting | 32/84 (38.1%) | 1.24 (0.57, 2.70) | 0.59 |
| Duration of diarrhoea (excluding day of enrolment) | |||
| 7–13 days of diarrhoea | 23/3633 (6.3%) | Ref. | – |
| 0–6 days of diarrhoea | 1389/6329 (21.9%) | 2.65 (1.29, 5.45) | 0.008 |
| Frequency of loose stools (24 hours before enrolment) | |||
| 3–6 stools (low frequency) | 599/3536 (16.9%) | Ref. | – |
| >6 stools (high frequency) | 813/3156 (25.8%) | 1.13 (0.97, 1.32) | 0.13 |
| Low birth weight | |||
| No | 516/2816 (18.3%) | Ref. | – |
| Yes | 93/363 (25.6%) | 1.09 (0.90, 1.32) | 0.37 |
| Exclusive breastfeeding at time of enrolment | |||
| No | 506/5280 (9.6%) | Ref | – |
| Yes | 79/1412 (5.6%) | 0.74 (0.53, 1.03) | 0.08 |
| Variable | Rotavirus aetiology | ||
|---|---|---|---|
| Prevalence n/N (%) | Adjusted | P value | |
| Maternal education | |||
| No formal education | 22.0% (381/1732) | Ref | – |
| Primary | 21.7% (640/2950) | 0.92 (0.82, 1.04) | 0.20 |
| Secondary | 19.3% (331/1719) | 0.86 (0.74, 1.00) | 0.04 |
| Higher education | 20.9% (53/254) | 0.88 (0.66, 1.18) | 0.39 |
| Paternal education | |||
| No formal education | 23.1% (366/1583) | Ref | – |
| Primary | 21.9% (511/2330) | 0.94 (0.83, 1.07) | 0.33 |
| Secondary | 19.6% (411/2094) | 0.87 (0.75, 1.00) | 0.05 |
| Higher education | 20.1% (95/473) | 0.90 (0.72, 1.13) | 0.38 |
| Wealth quintile | |||
| Q1-poorest | 35.5% (307/864) | Ref | – |
| Q2 | 27.7% (303/1094) | 1.07 (0.94, 1.21) | 0.32 |
| Q3 | 14.9% (160/1071) | 0.98 (0.80, 1.20) | 0.84 |
| Q4 | 18.2% (323/1779) | 1.18 (0.97, 1.45) | 0.10 |
| Q5-richest | 16.9% (319/1884) | 1.10 (0.89, 1.38) | 0.35 |
| Number of children <5 years of age in the household | |||
| 1 | 23.5% (824/3509) | Ref | – |
| 2 | 18.9% (428/2259) | 1.04 (0.93, 1.15) | 0.50 |
| >3 | 17.3% (160/924) | 0.99 (0.84, 1.17) | 0.94 |
| Presence of animal at home | |||
| No | 25.5% (970/3803) | Ref | – |
| Yes | 15.3% (442/2889) | 1.05 (0.92, 1.21) | 0.47 |
| Presence of improved source of water | |||
| No | 12.2% (95/776) | Ref | – |
| Yes | 22.3% (1317/5916) | 1.13 (0.88, 1.44) | 0.35 |
| Improved sanitation facility | |||
| No | 20.9% (285/1365) | Ref | – |
| Yes | 21.2% (1127/5327) | 0.92 (0.79, 1.07) | 0.30 |
- —http://dx.doi.org/10.13039/100000865Bill and Melinda Gates Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Hepatitis Viruses Studies and Epidemiology
Introduction
Diarrhoea remains one of the leading causes of global child mortality and was estimated to cause about 444 000 child deaths in 2021.1 In 2013, prior to the roll-out of vaccination programmes, rotavirus infection was responsible for about 24% of diarrhoeal deaths in childhood, most of which occurred in low and middle-income countries (LMICs).2 3 Several countries in East and Southern Africa have implemented rotavirus vaccine roll-outs, with coverage increasing from 0% in 2010 to 90% in 2015. Concomitantly, there is evidence that vaccination has contributed to a reduction in rotavirus infections among children hospitalised with diarrhoea.4 Rotavirus vaccination is also associated with a reduced rate of rotavirus infection, especially in subpopulations of children such as those admitted with undernutrition.5 However, despite rotavirus vaccination programmes, the burden of rotaviral infection remains high, with rotaviral diarrhoea estimated to account for 19% of diarrhoeal deaths globally in 2019.6
Even though rotavirus vaccination reduces the incidence of rotavirus-associated diarrhoea, the numbers of cases remain high in LMICs.3 Several studies indicate that rotavirus vaccine is effective for severe rotavirus gastroenteritis.4 7 In a randomised controlled trial, 1.9% of infants in the rotavirus vaccine group vs 4.9% of infants in the placebo group developed severe gastroenteritis during the first year of life.8 Children presenting with rotaviral diarrhoea aetiology often experience a more severe form of diarrhoea in comparison to children with other diarrhoea.9 There is earlier information on the association between rotaviral aetiology and clinical as well as sociodemographic factors. Symptoms such as watery diarrhoea, fever, vomiting and dehydration associated with rotavirus infection can cause further complications that could lead to hospitalisation and other downstream effects.9 Socioeconomic factors such as age and crowded households are associated with rotavirus infection.5 Maternal illiteracy as well as stunting and wasting was associated with dehydrating rotavirus diarrhoea.10 Although there are now point-of-care tests for rotavirus infection, these are often not available in resource-constrained settings.11 Therefore, identifying risk factors of rotaviral aetiology would be a useful tool to assist in identifying rotaviral diarrhoea aetiology.
Several factors play a role in increasing the risk of any disease, including rotaviral diarrhoea aetiology. There is not much information on sociodemographic and clinical risk factors for children treated on the outpatient basis, especially in LMIC populations where rotavirus vaccination has been widely distributed. To our knowledge, this is the first analysis to correlate rotaviral aetiology with sociodemographic and clinical factors from several LMICs, especially after rotavirus vaccination. Therefore, this study aims to assess if a rotaviral diarrhoea aetiology in 2–23-month-old children is associated with the child’s earlier vaccination, socioeconomic status and clinical signs and symptoms. We hypothesised that among children presenting with diarrhoea at outpatient clinics, those with a prior receipt of rotaviral vaccine would have a lower probability of rotavirus diarrhoea than unvaccinated children. We also examined the association of rotaviral diarrhoea aetiology with clinical and socioeconomic factors using secondary data from a clinical trial of antibiotics in 2–23-month-old children with diarrhoea and increased risk of mortality carried out in 7 LMICs.
Methods
Ethical approval
Ethical approval for the main Antibiotics for Children with Diarrhoea (ABCD) trial was obtained from WHO Ethics review committee (protocol ID: ERC.0002722) as well as institutional review boards from all sites including Bangladesh, India, Kenya, Malawi, Mali, Pakistan and Tanzania.
Study design and participants
We performed a secondary analysis of a multicentre clinical trial of antibiotics for children with diarrhoea and increased risk of mortality (ABCD, ClinicalTrials.gov Identifier: NCT03130114) ages 2–23 months. ABCD was a multicountry, double-blinded, randomised, placebo-controlled clinical trial that assessed whether a 3-day long treatment with azithromycin would reduce all-cause mortality among 2–23-month-old children with diarrhoea and increased risk of mortality.12 13 The ABCD trial was conducted at seven sites including Bangladesh, India, Kenya, Malawi, Mali, Pakistan and Tanzania between June 2017 and July 2019.
The definition of children with diarrhoea and increased risk of mortality in this study was a history of acute watery diarrhoea (>3 loose/watery stool in the past 24 hours) for <14 days with one or more of the following high mortality-risk defining characteristics: moderate acute malnutrition (MAM) (defined as weight-for-length z-score (WLZ) <−2 and >−3 or mid-upper arm circumference (MUAC) >115 mm and <125 mm for children over 6 months), presence of some or severe dehydration, or severe stunting (length-for-age z-score (LAZ) <−3). Children were excluded if they had any of the following: allergy or contraindication to azithromycin; use of antibiotics in the 14 days before presentation or current use of antibiotics; clinical suspicion of Vibrio cholerae infection; or living far from the enrolment centre that would hinder direct observation on days 2 and 3; previous or current enrolment in this or any interventional trial; or sibling or another child in the same household enrolled in this trial. Written informed consent was obtained after which the participant was randomised to azithromycin or placebo arm.13
Approximately, the first 1000 participants at each site were requested to give a stool sample prior to antibiotic treatment initiation. In this secondary analysis, enteropathogen data obtained from stool samples as well as data collected at baseline were used in order to assess the likelihood of rotavirus aetiology associated with a prior receipt of rotaviral vaccine or various clinical or socioeconomic characteristics of the children.
Study Variables
The outcome variable in the current association analyses was aetiology of the diarrhoea episode, indicated as rotaviral aetiology (yes/no). The main exposure variable was earlier receipt of at least one dose of rotavirus vaccination. Additional exposure variables of interest included child clinical characteristics including age, high mortality-risk defining characteristic, prolonged duration of diarrhoea, high number of loose/watery stools and low birth weight. Moreover, sociodemographic and environmental exposure variables, including maternal and paternal education, number of under-5-year-old children in the household, presence of animals in the household, quality of sanitary facilities, quality of water sources and wealth quintile of the household, were evaluated. These characteristics have been detailed in online supplemental note 1.
Whole stool samples were collected, and where not possible, a flocked rectal swab was obtained. Diarrhoea-specific aetiology was determined from these samples, frozen at −80°C until analysis, using a quantitative PCR (qPCR) and a customised 85-target TaqMan array card. The details of the qPCR analysis have been described elsewhere14 but briefly, using the QIAmp Stool Fast DNA Mini kit (Qiagen, Valencia, CA), total nucleic acid was extracted from the samples, put into the TAC card and run in a ViiA 7 or QuantStudio 7 Flex Real Time PCR system (Thermo Fisher, CA). The method used for determining aetiology cut-offs was adapted from previous large multisite diarrhoea studies.14 Briefly, this was based on the quantity of the pathogen DNA/RNA in the stool sample (ie, pathogen burden) at the species level. Each cut-off was determined by calculating the median quantity-specific OR from site-specific models in the previous studies; two large multisite diarrhoea studies: the seven-site GEMS study and the eight-site Malnutrition and the Consequences for Child Health and Development cohort study. Subsequently, the episode-specific attributable fraction (AFe) was computed. A locally estimated scatterplot smoothing regression was then applied, and the highest cycle threshold (Ct) value with an AFe greater than 0.5 was selected as the cut-off for each pathogen. In this analysis, rotavirus aetiology 32.0 Ct cut-off value was used, as per previous studies.14
Rotavirus vaccination status was determined by reviewing the child’s vaccination card or, if the card was not available, then queried by caretaker recall. One or more doses of rotavirus vaccine were categorised as yes/no variable for any prior receipt of rotavirus vaccine. Other exposure variables were obtained via questionnaires at baseline by asking the mother/caregiver. Clinical characteristics were determined by clinician assessment at baseline.
Statistical analysis
We hypothesised that among children presenting with diarrhoea, those with a prior receipt of rotavirus vaccine would have a lower probability of rotavirus diarrhoea than unvaccinated children. Second, we hypothesised that those presenting with low birth weight, longer duration of diarrhoea, more loose/watery stools and being moderately malnourished would have a higher probability of rotaviral diarrhoea aetiology than those without these characteristics. Finally, we hypothesised that those having low maternal and paternal education, lower wealth quintile, poor source of water, no latrine, parents with domestic animal ownership or high number of under-5-year-old children would have a higher probability of rotaviral diarrhoea aetiology in comparison to those without these characteristics.
In order to determine the association between any prior receipt of rotavirus vaccine or selected sociodemographic and clinical factors and rotaviral diarrhoea aetiology, we calculated prevalence ratios (PR) with log-binomial regression models.15 If the log-binomial models did not converge, we used log-Poisson models, which provided consistent but not fully efficient estimates of the prevalence ratios and their CIs.16 We referred to estimates as prevalence ratios in this study rather than relative risks due to the cross-sectional design of the study. This was done to avoid inferring directionality of the relationship, particularly for clinical factors at presentation which may be a consequence of the diarrhoeal pathogens. Unadjusted (bivariate) as well as adjusted (multivariable) analyses were conducted. The multivariable models encompassed variables that were deemed to be potential confounders for the association between diarrhoeal aetiology and prior rotavirus vaccination.
For statistical analysis, the outcome variable was rotaviral diarrhoea aetiology, categorised as yes/no based on the Ct cut-off values as described above. The main exposure of any prior receipt of rotavirus vaccine was categorised as yes/no. Other variable categorisation details are available in the online supplemental note 1.
We conducted sensitivity analyses to determine the association of clinical factors with rotavirus aetiology after adjusting for rotavirus vaccination as well. We also evaluated the association of sociodemographic factors with rotavirus aetiology after adjusting for clinical factors together with rotavirus vaccination. Furthermore, we evaluated these associations with rotavirus aetiology without a coinfection noted at an aetiological level. This was determined by using the Ct cut-off value for only rotavirus aetiology present in the stool without any coinfection from other aetiology (if any other aetiology was present based on the cut-off, it was considered non-rotaviral aetiology). All statistical analyses were carried out using R version 4.0.2 Software (R Foundation for Statistical Computing).
Results
All 8268 children aged 2–23-month-old with moderate-to-severe diarrhoea were enrolled in the ABCD trial. Of these, 6,699 provided a stool sample that was analysed with qPCR of which two participants had missing microbiological results. This resulted in 6,697 infants having a result on the microbiological aetiology of the diarrhea episode (figure 1).
Flow chart of 2–23-month-old children presenting with moderate to severe diarrhoea. ‘Likely’ diarrhoea-associated aetiology was determined by Ct value cut-offs for specific enteropathogens. Ct values greater than these cut-offs but <35 were considered ‘possible’ aetiologies, while Ct value >35 was considered ‘Unlikely’ aetiology. ‘Likely’ rotaviral diarrhoea aetiology was determined by Ct value cut-off of 32.0. Ct, cycle threshold.
The mean age of infants was 11.6 months (SD: 5.3) and 53.8% were male across all sites (table 1). The proportion of children with rotaviral diarrhoea aetiology was 21.1% in the full study population, with lowest proportion at the Kenya (11.0%), Pakistan (11.6%) and Tanzania (11.1%) sites while the highest proportion was in Bangladesh (47.3%) (online supplemental table 1a). The proportion of children with prior receipt of locally available (online supplemental table 1a) rotavirus vaccination was 59.9%, ranging from 1.0%, 2.7% and 7.3% in Asian sites (Bangladesh, India and Pakistan, respectively) and over 99% coverage in Tanzania, Kenya and Malawi (online supplemental table 1a). Each site had a different type of rotavirus vaccination type and number of doses that was administered at the national level (online supplemental table 1b).
The prevalence of rotavirus aetiology was 21.1% in this cohort; 17.6% among participants who had had at least one prior rotavirus vaccination and 25.9% among those who were unvaccinated. Rotavirus vaccination was inversely associated with the prevalence of rotaviral diarrhoea aetiology in unadjusted models (p value <0.001); however, after adjusting for potential confounders, the association between rotavirus vaccination and the prevalence of rotaviral diarrhoea aetiology at presentation was not statistically significant (PR: 0.71, 95% CI 0.49, 1.03) (table 2). Similarly, there was no association of rotavirus vaccination with the prevalence of rotavirus aetiology with no coinfection after adjusting for confounders in sensitivity analyses (online supplemental table 2).
We also examined five clinical correlates of rotavirus aetiology (table 3). Of these, only diarrhoea duration was associated with rotavirus aetiology. The prevalence of rotavirus aetiology was 21.9% in those with shorter duration (0–6 days before presentation) vs 6.3% in those with prolonged diarrhoea (7–13 days) (PR: 2.65; 95% CI: 1.29 to 5.45). No association was noted between any clinical characteristic with the prevalence of a single rotavirus aetiology only (without any other aetiology present as determined by Ct cut-off values) in sensitivity analyses (online supplemental table 3).
Of the seven studied sociodemographic factors, both maternal and paternal education were associated with rotavirus aetiology (table 4). Children whose mothers had at least a secondary education had a lower prevalence of rotavirus aetiology (PR 0.86, 95% CI 0.74, 1.00) as compared with no formal maternal education (table 4). Similarly, those whose fathers had at least secondary education also had a lower prevalence of rotavirus aetiology (PR 0.87, 95% CI 0.75, 1.00) in comparison to those without formal paternal education (table 4). In a sensitivity analysis adjusting for rotavirus vaccination, a potential mediator, there was no association of maternal or paternal education with rotavirus aetiology. There was also no association between any sociodemographic characteristic and the prevalence of rotavirus aetiology without coinfection in sensitivity analyses (online supplemental table 4).
Discussion
Among 2–23-month-old children presenting with acute diarrhoea and increased risk of mortality at outpatient clinics, we found a few clinical and socioeconomic factors associated with rotaviral diarrhoea. The association between rotavirus vaccination and the prevalence of rotaviral diarrhoea aetiology was not statistically significant after adjusting for potential confounders. Of the clinical factors, age, risk-defining criteria, frequency of loose stools and low birth weight were not associated with prevalence of rotaviral diarrhoea. Only shorter diarrhoea duration was associated with higher prevalence of rotaviral aetiology. Of the socioeconomic factors, wealth quintile, number of children <5 years of age, presence of animal, improved water and improved sanitation were not associated with prevalence of rotaviral diarrhoea. Only maternal and paternal education was associated with a lower prevalence of rotavirus aetiology.
Our estimates of rotaviral diarrhoea aetiology and the relationship with rotavirus vaccine and sociodemographic and clinical correlates are applicable to children in LMICs with diarrhoea and increased risk of mortality that presented to a facility. The range of the exposure was wide since rotavirus vaccination rates varied between sites (from as low as 1.0% to 99.9%). This heterogeneity could lead to lack of precision and therefore, we adjusted for site of enrolment in all multivariable analyses. In addition, there is likely some degree of maternal recall bias in variables like duration of diarrhoea and number of stools prior to enrolment. This could bias the findings towards the null hypothesis. Nevertheless, our findings suggest that rotaviral aetiology among 2–23-month-old children with acute diarrhoea cannot be reliably determined by data on previous rotavirus vaccination, clinical and sociodemographic factors.
An association between shorter diarrhoea duration and increased prevalence of rotavirus aetiology is consistent with the knowledge that rotavirus causes a more severe form of diarrhoea compared with other viruses, causing children to be sicker and more likely to be dehydrated, leading to hospital presentation.9 This is also confirmed by the fact that rotavirus usually has a short incubation period of less than 48 hours.17 Results from a cross-sectional study from Nigeria18 were consistent with our findings that maternal or paternal secondary education is associated with lower prevalence of rotavirus. It is known globally that maternal education has great impact on child health outcomes19 and parent’s education level influences beneficial practices such as uptake of vaccines.
There are some limitations in our study data, including its cross-sectional nature, restricting the cohort to a specific group, the method of determining enteropathogens and not assessing other inflammatory influences or collecting certain variables. First, the nature of this cross-sectional, observational analysis prevents us from making causal inferences. Moreover, the participants in the study included only children with diarrhoea and increased risk of mortality which limits the generalisability of our findings. Using enteropathogen cut-offs is complex, especially within sites where there is high carriage of asymptomatic enteropathogens. Another potential reason behind the poorer response to rotavirus vaccine in LMICs is environmental enteric dysfunction (EED) as suggested in prior studies but not measured in our study.20 Due to the parent trial enrolment criteria, we cannot make inferences about rotaviral diarrhoea aetiology in the community or among all children presenting to a facility nor the relationship of factors with diarrhoea incidence or hospitalisation.
The prevalence of rotaviral diarrhoea aetiology in children has been studied widely. However, this unique cohort in children with increased risk of mortality, presenting with diarrhoea at health facilities, provides an opportunity to understand this high-risk group. Most studies focused on the impact on rotaviral diarrhoea aetiology after introduction of rotavirus vaccination, where they noted that after introduction of rotavirus vaccination, the prevalence of rotaviral diarrhoea aetiology is lower. However, this reduction is not as much in low-income settings as it is in high-income settings implying varying vaccine effectiveness globally.4 6 7 21 Additionally, malnutrition with micronutrient deficiencies, which is common in low and middle-income settings like those in our study, may play a role in the effectiveness of rotavirus vaccine.22 Studies have suggested factors that reduced effectiveness of rotavirus vaccine in such settings include differences in gut microbiota, immaturity of infant immune system and coinfections among others.23 Moreover, rotavirus has over 100 different serotypes and rotavirus vaccine covers only some of the most common of them. Therefore, vaccination cannot confer complete protection.24 Additionally, association of biomarkers of environmental enteropathy (a subclinical intestinal condition characterised by gut barrier dysfunction, reduced intestinal absorption as well as gut inflammation) is associated with reduced responses to rotavirus vaccination.25 26 Conversely, a study noted no associations between EED biomarkers and rotavirus vaccine immunogenicity in rural Zimbabwean infants.20 We did not measure EED biomarkers or immunogenicity specifically in this trial and therefore, we cannot explain the reason behind this non-significant association of rotavirus vaccination and rotaviral diarrhoea aetiology.
In summary, in the analysis of this large cohort, we note that a rotaviral aetiology cannot be accurately determined among 2–23-month-old children with acute diarrhoea by information on the child’s earlier vaccination. Receiving any prior rotavirus vaccination does not mean complete protection to rotaviral diarrhoea aetiology among those presenting with diarrhoea especially in an LMIC. Moreover, it is complicated to use characteristics as risk factors of rotaviral diarrhoea aetiology. Although association of risk factors such as shorter diarrhoea duration and maternal and paternal education exists, it may not be very useful in assisting clinical staff in identifying children with rotaviral diarrhoea among all those presenting with diarrhoea at a health facility.
Supplementary material
10.1136/bmjgh-2024-018337online supplemental file 1
10.1136/bmjgh-2024-018337online supplemental table 1
10.1136/bmjgh-2024-018337online supplemental table 2
10.1136/bmjgh-2024-018337online supplemental table 3
10.1136/bmjgh-2024-018337online supplemental table 4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UNICEF DATA Diarrhoea Availablehttps://data.unicef.org/topic/child-health/diarrhoeal-disease/Accessed 02-Mar-2024
- 2Troeger C Blacker BF Khalil IA et al Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016 Lancet Infect Dis 20181812112810.1016/S 1473-3099(18)30362-130243583 PMC 6202444 · doi ↗ · pubmed ↗
- 3Clark A Black R Tate J et al Estimating global, regional and national rotavirus deaths in children aged P Lo S ONE 201712 e 018339210.1371/journal.pone.018339228892480 PMC 5593200 · doi ↗ · pubmed ↗
- 4Weldegebriel G Mwenda JM Chakauya J et al Impact of rotavirus vaccine on rotavirus diarrhoea in countries of East and Southern Africa Vaccine (Auckl)20183671243010.1016/j.vaccine.2017.10.050PMC 1197673429102168 · doi ↗ · pubmed ↗
- 5Chissaque A Cassocera M Gasparinho C et al Rotavirus A infection in children under five years old with a double health problem: undernutrition and diarrhoea - a cross-sectional study in four provinces of Mozambique BMC Infect Dis 2021211810.1186/s 12879-020-05718-933407207 PMC 7788695 · doi ↗ · pubmed ↗
- 6Du Y Chen C Zhang X et al Global burden and trends of rotavirus infection-associated deaths from 1990 to 2019: an observational trend study Virol J 20221916610.1186/s 12985-022-01898-936266651 PMC 9585833 · doi ↗ · pubmed ↗
- 7Platts-Mills JA Amour C Gratz J et al Impact of Rotavirus Vaccine Introduction and Postintroduction Etiology of Diarrhea Requiring Hospital Admission in Haydom, Tanzania, a Rural African Setting Clin Infect Dis 20176511445110.1093/cid/cix 49428575304 PMC 5850044 · doi ↗ · pubmed ↗
- 8Madhi SA Cunliffe NA Steele D et al Effect of human rotavirus vaccine on severe diarrhea in African infants N Engl J Med 20103622899810.1056/NEJ Moa 090479720107214 · doi ↗ · pubmed ↗