Knowledge of Iron Deficiency Anaemia and Associated Attributes Among School Adolescents in Eastern India: A Cross-Sectional Evaluation
Bijit Biswas, Anuradha Gautam, G. Jahnavi, Richa Richa, Pratima Gupta, Saurabh Varshney

TL;DR
This study evaluated school adolescents in Eastern India's knowledge about iron deficiency anemia and related health programs, finding that older students and those with literate parents had better knowledge.
Contribution
The study identifies demographic and symptom-related factors influencing knowledge of anemia and interventions among school adolescents in Eastern India.
Findings
Median knowledge scores for IDA were 14, and for WIFS and deworming were 9.
Knowledge was higher in older students, higher grades, and those with literate parents.
Boys had higher WIFS knowledge than girls.
Abstract
Background: This study assessed knowledge related to iron deficiency anaemia (IDA), weekly iron and folic acid supplementation (WIFS), and school-based deworming among school-going adolescents in Eastern India, along with key associated attributes. Methods: A cross-sectional survey was conducted among 843 students (Standards 8-10) from four government schools in Deoghar, Jharkhand, using multistage probability sampling. A validated Hindi questionnaire was used to assess knowledge alongside symptoms, clinical pallor, and anthropometry. Results: Median knowledge scores were 14 (interquartile range (IQR): 7-18) for IDA and 9 (IQR: 6-11) for WIFS and deworming. IDA knowledge positively correlated with the number of anaemia-related symptoms (ρ = 0.269, p < 0.001); WIFS and deworming knowledge showed a similar trend (ρ = 0.276, p < 0.001). Participants reporting ≥ 3 symptoms had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
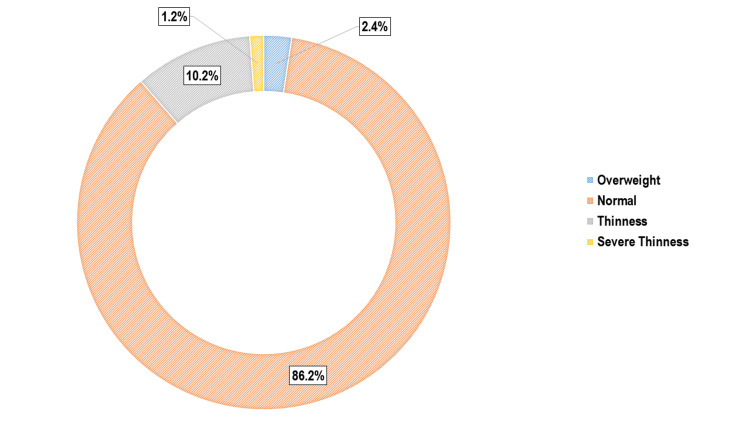 Figure 1
Figure 1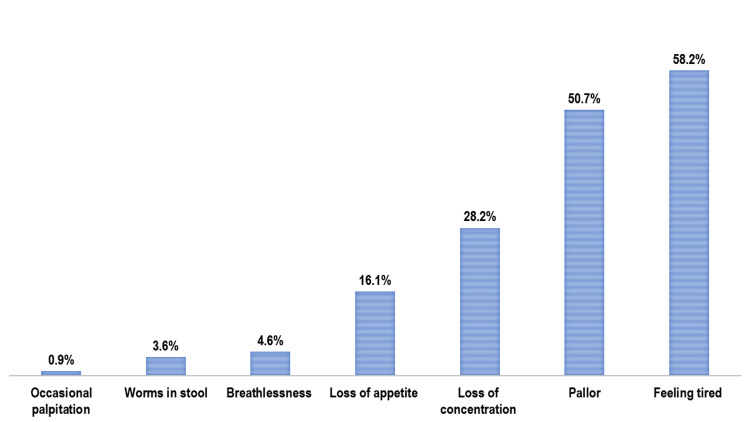 Figure 2
Figure 2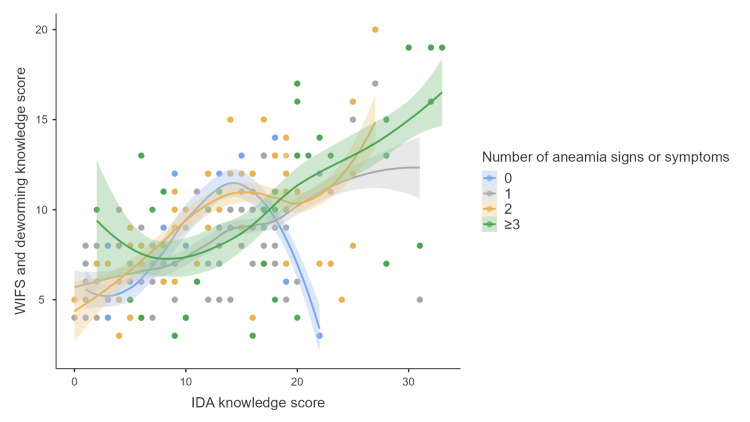 Figure 3
Figure 3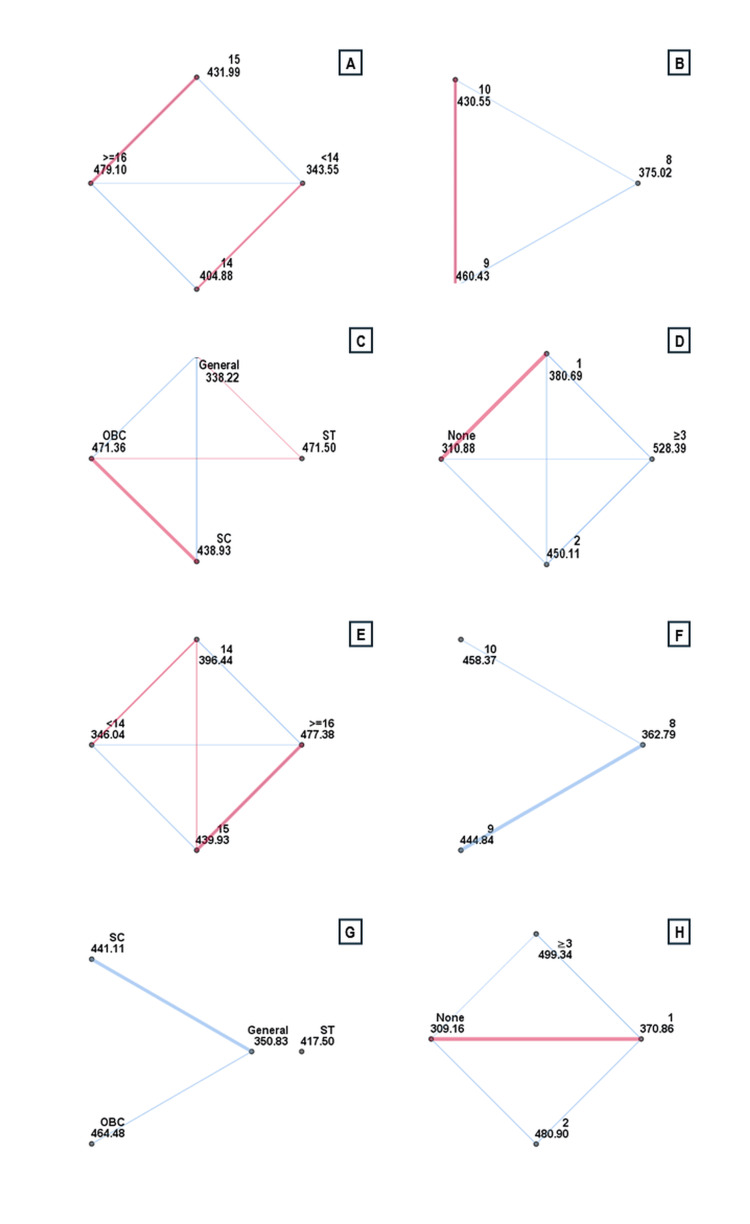 Figure 4
Figure 4| Item | Variable | Correct Response | N (%) |
| Knowledge regarding IDA | |||
| What do you know about the symptoms of anaemia? | |||
| K1 | Feeling tired is a symptom of anaemia | True | 472 (56.0) |
| K2 | Anaemia can cause difficulty in concentrating | True | 251 (29.8) |
| K3 | Loss of appetite can be a sign of anaemia | True | 324 (38.4) |
| K4 | Passing worms in the stool can be related to anaemia | True | 167 (19.8) |
| K5 | People with anaemia may feel their heart beating fast (palpitations) | True | 172 (20.4) |
| How can you recognize someone who has anaemia? | |||
| K6 | People with anaemia often feel weak | True | 519 (61.6) |
| K7 | Anaemia can cause paleness in the skin, tongue, or palms | True | 281 (33.3) |
| K8 | Spoon-shaped nails (koilonychia) can be a sign of anaemia | True | 177 (21.0) |
| K9 | Anaemic people may fall sick more often | True | 195 (23.1) |
| What do you know about the effects of anaemia on adolescents? | |||
| K10 | Anaemia can affect your physical growth | True | 334 (39.6) |
| K11 | It can lead to poor performance in school | True | 386 (45.8) |
| K12 | Anaemia can reduce your ability to fight infections | True | 276 (32.7) |
| K13 | It may cause menstrual problems in girls | True | 174 (20.6) |
| What are the causes of IDA? | |||
| K14 | Not eating enough iron-rich foods can cause anaemia | True | 448 (53.1) |
| K15 | Infections like malaria or worm infestation can lead to anaemia | True | 294 (34.9) |
| K16 | Heavy bleeding during periods may cause anaemia | True | 225 (26.7) |
| K17 | Walking barefoot can increase the chance of getting worm infestation | True | 87 (10.3) |
| K18 | Not taking iron tablets (IFA) can lead to anaemia | True | 166 (19.7) |
| K19 | Not taking deworming medicine (Albendazole) can increase anaemia risk | True | 264 (31.3) |
| How can anaemia be prevented? | |||
| K20 | Eating iron-rich foods helps prevent anaemia | True | 556 (66.0) |
| K21 | Eating fruits rich in vitamin C helps the body absorb iron | True | 418 (49.6) |
| K22 | Taking iron tablets regularly can prevent anaemia | True | 272 (32.3) |
| K23 | Treating infections early helps in preventing anaemia | True | 151 (17.9) |
| What are some good sources of iron? | |||
| K24 | Green leafy vegetables (like spinach) are rich in iron | True | 470 (55.8) |
| K25 | Jaggery (gur) is a good source of iron | True | 488 (57.9) |
| K26 | Whole grains (like wheat, bajra) contain iron | True | 462 (54.8) |
| K27 | Fruits (like pomegranate, apple) are sources of iron | True | 514 (61.0) |
| K28 | Liver (animal source) contains iron | True | 312 (37.0) |
| K29 | Fish is a good source of iron | True | 354 (42.0) |
| K30 | Pulses and legumes (like lentils, rajma) are rich in iron | True | 226 (26.8) |
| K31 | Nuts (like almonds, groundnuts) contain iron | True | 327 (38.8) |
| What helps or harms iron absorption and adolescent needs? | |||
| K32 | Drinking tea or coffee after meals reduces iron absorption | True | 535 (63.5) |
| K33 | Eating vitamin C-rich foods (like lemon or amla) helps absorb iron | True | 461 (54.7) |
| K34 | Teenagers need more iron and folic acid than children or adults | True | 415 (49.2) |
| Knowledge regarding WIFS and deworming | |||
| How should iron tablets (IFA) AND deworming tablets (albendazole) be taken in school? | |||
| K35 | How often should the iron tablet (IFA) given in school be taken? | Weekly | 306 (36.3) |
| K36 | When should the iron tablet (IFA) be taken? | After Food | 318 (37.7) |
| K37 | How often should the deworming tablet (albendazole) be taken in school? | Twice a year (Bi-annually) | 474 (56.2) |
| What are the benefits of taking iron tablets (IFA)? | |||
| K38 | Iron tablets (IFA) have no benefit | False | 755 (89.6) |
| K39 | Iron tablets help improve concentration | True | 339 (40.2) |
| K40 | Iron tablets help you feel healthier | True | 496 (58.8) |
| K41 | Iron tablets help in gaining weight | True | 187 (22.2) |
| K42 | Iron tablets reduce tiredness | True | 261 (31.0) |
| What are the benefits of taking deworming tablets (albendazole)? | |||
| K43 | Deworming tablets have no benefit | False | 794 (94.2) |
| K44 | Deworming tablets kill stomach worms | True | 632 (75.0) |
| K45 | Deworming tablets kill filaria parasites | True | 353 (41.9) |
| What are the common side effects of iron tablets (IFA)? | |||
| K46 | Iron tablets have no side effects | False | 667 (79.1) |
| K47 | Iron tablets can make stool look black | True | 210 (24.9) |
| K48 | Iron tablets can cause a metallic taste in mouth | True | 267 (31.7) |
| K49 | Iron tablets can make the stomach feel full | True | 194 (23.0) |
| K50 | Iron tablets can cause constipation | True | 99 (11.7) |
| K51 | Iron tablets can cause stomach pain | True | 144 (17.1) |
| K52 | Iron tablets can cause loose motion (diarrhoea) | True | 123 (14.6) |
| K53 | Iron tablets can cause nausea | True | 162 (19.2) |
| K54 | Iron tablets can cause headache | True | 191 (22.7) |
| Variable | N (%) | Knowledge Score Regarding IDA Median (IQR) | Test Statistic | p-value | Knowledge Score Regarding WIFS and Deworming Median (IQR) | Test Statistic | p-value |
| School: | |||||||
| 1 | 215 (25.5) | 13 (7-18) | 0.642 | 0.887# | 8 (6-11) | 1.513 | 0.679# |
| 2 | 224 (26.6) | 14 (8-18) | 8 (6-11) | ||||
| 3 | 196 (23.3) | 14 (7-19) | 9 (7-11) | ||||
| 4 | 208 (24.7) | 14 (6-19) | 9 (6-11) | ||||
| Age in completed years: | |||||||
| < 14 | 104 (12.3) | 10 (6-17) | 22.197 | <0.001# | 7 (5-9) | 23.866 | <0.001# |
| 14 | 272 (32.3) | 13 (6-18) | 8 (6-11) | ||||
| 15 | 294 (34.9) | 14 (6-19) | 9 (6-11) | ||||
| ≥ 16 | 173 (20.5) | 15 (9-19) | 9 (7-11) | ||||
| Gender: | |||||||
| Male | 401 (47.6) | 14 (8-18) | 0.065 | 0.948* | 9 (7-11) | 5.674 | <0.001* |
| Female | 442 (52.4) | 14 (6-19) | 7 (6-11) | ||||
| Reading standard: | |||||||
| 8 | 281 (33.3) | 12 (6-17) | 17.849 | <0.001# | 8 (6-10) | 25.578 | <0.001# |
| 9 | 281 (33.3) | 15 (7-19) | 9 (6-11) | ||||
| 10 | 281 (33.3) | 14 (8-18) | 9 (7-11) | ||||
| Caste: | |||||||
| General | 276 (32.7) | 9 (4-16) | 50.652 | <0.001# | 7 (6-10) | 36.912 | <0.001# |
| OBC | 397 (47.1) | 15 (9-19) | 9 (7-11) | ||||
| SC | 150 (17.8) | 15 (6-19) | 9 (6-12) | ||||
| ST | 20 (2.4) | 15 (12-19) | 9 (7-10) | ||||
| Religion: | |||||||
| Hindu | 761 (90.3) | 14 (7-19) | 1.178 | 0.239* | 9 (6-11) | 0.637 | 0.524* |
| Muslim | 82 (9.7) | 14 (7-16) | 9 (6-10) | ||||
| Father's educational level: | |||||||
| Illiterate | 269 (31.9) | 11 (6-17) | 3.993 | <0.001* | 8 (6-10) | 4.686 | <0.001* |
| Literate | 574 (68.1) | 14 (8-19) | 9 (7-11) | ||||
| Mother's educational level: | |||||||
| Illiterate | 306 (36.3) | 11 (6-16) | 5.669 | <0.001* | 7 (5-9) | 7.269 | <0.001* |
| Literate | 537 (63.7) | 15 (8-19) | 10 (7-11) | ||||
| PCMI (in USD): | |||||||
| Q1 (6.1-10.2) | 179 (21.2) | 15 (7-17) | 6.000 | 0.112# | 8 (6-10) | 14.150 | 0.003# |
| Q2 (10.3-15.2) | 147 (17.4) | 15 (10-19) | 9 (7-11) | ||||
| Q3 (15.3-21.4) | 238 (28.2) | 14 (1-18) | 9 (7-11) | ||||
| Q4 (21.5-203.4) | 279 (33.1) | 11 (6-19) | 9 (6-12) | ||||
| Type of diet: | |||||||
| Vegetarian | 85 (10.1) | 7 (3-16) | 4.525 | <0.001* | 7 (4-11) | 3.242 | 0.001* |
| Non-vegetarian | 758 (89.9) | 14 (8-19) | 9 (7-11) | ||||
| Nutritional status: | |||||||
| Normal | 727 (86.2) | 14 (7-19) | 3.301 | 0.001* | 9 (6-11) | 0.143 | 0.887* |
| Malnourished | 116 (13.8) | 12 (8-16) | 8 (7-12) | ||||
| Number of anaemia signs or symptoms: | |||||||
| None | 94 (11.2) | 9 (3-17) | 62.866 | <0.001# | 7 (5-9) | 66.511 | <0.001# |
| 1 | 331 (39.3) | 13 (6-17) | 8 (6-10) | ||||
| 2 | 260 (30.8) | 15 (9-19) | 10 (7-12) | ||||
| ≥ 3 | 158 (18.7) | 17 (10-22) | 10 (7-13) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Child Nutrition and Water Access · Hemoglobinopathies and Related Disorders
Introduction
Iron deficiency anaemia (IDA) continues to pose a significant public health challenge globally, particularly among adolescents in low- and middle-income countries. It is estimated that over 2 billion individuals are anaemic, with iron deficiency accounting for nearly half of all cases [1,2]. Adolescents are especially vulnerable due to rapid physical growth, poor dietary diversity, and in girls additional losses from menstruation [1,3]. The consequences of IDA include impaired cognitive and physical development, increased susceptibility to infections, and reduced academic and work productivity [1,3,4].
India bears a substantial share of this burden. According to the National Family Health Survey (NFHS-5), anaemia prevalence among adolescents aged 15-19 years rose from 55.8% to 59.1% in girls and from 30.2% to 31.1% in boys compared to NFHS-4 [5]. In Jharkhand, the prevalence is even higher: 65.8% in girls and 39.7% in boys [6]. To address this issue, the Government of India introduced the weekly iron and folic acid supplementation (WIFS) programme in 2012 and the National Deworming Day (NDD) initiative in 2015, targeting adolescents through schools and anganwadis [7,8]. These programs provide weekly iron-folic acid tablets, biannual albendazole, and health education. However, despite nationwide implementation, studies have reported poor awareness, low compliance, and persistent misconceptions about supplementation, especially in underserved areas [9-11].
While most existing studies have focused on adolescent girls or evaluated program effectiveness, few have explored knowledge levels and their correlates among adolescents in school settings [10-14]. This study was conducted to assess knowledge regarding IDA, WIFS, and deworming among school-going adolescents in Deoghar district of Jharkhand, and to examine associations with socio-demographic, clinical, and nutritional attributes. The findings aim to inform more targeted and context-specific adolescent anaemia prevention strategies.
Materials and methods
Study design and setting
An analytical cross-sectional study was conducted among school-going adolescents enrolled in Standards 8-10 across four coeducational government schools in Deoghar district, Jharkhand, India. The study aimed to assess knowledge related to IDA and associated factors. To capture contextual variability, two administrative blocks, Devipur and Deoghar, were purposively selected from the 10 blocks comprising the district. According to school cluster mapping, Devipur included nine school clusters with an average of 24 schools per cluster (range: 19-26), while Deoghar had 17 clusters with an average of 22 schools (range: 9-45) [15,16]. From each block, two clusters were randomly selected, and one coeducational school was randomly chosen from each cluster.
Sample size and sampling technique
The sample size was calculated based on the assumption that 15.1% of participants would demonstrate correct knowledge about IDA, as previously reported by Subba et al. in a school-based study from Anantapur district, Andhra Pradesh [12]. With a 95% confidence level, 20% relative precision, and a design effect of 1.5 to account for cluster sampling, the minimum required sample size was calculated to be 817 using the Statulator online tool [17]. A total of 843 students were ultimately enrolled in the study.
Sample allocation to each school was performed using the probability proportionate-to-size (PPS) method. Within each selected school, students were identified using computer-generated random number lists produced via OpenEpi [18]. 12 lists, one for each class section, contained roll numbers ranging from 1 to 150. On the day of the survey, students were approached based on these lists until the target number was reached for each school.
Data collection tools and procedures
Following written informed consent, data were collected using a structured, self-administered questionnaire in Hindi. The tool was developed through an extensive literature review focusing on adolescent anaemia, the WIFS programme, and school-based deworming initiatives [2,7,10-12,14,19-21]. Face, content, and criterion validity were established through expert consultation.
The questionnaire consisted of three sections. The first section captured socio-demographic information, including age, sex, caste, religion, parental education, and per capita monthly income (PCMI). The second section assessed knowledge of IDA using 34 items across seven domains: symptoms, clinical signs, consequences, causes, prevention, dietary sources, and absorption-related factors. Each correct response was scored as ‘1’, and incorrect as ‘0’, yielding a total possible score of 0-34. This section demonstrated high internal consistency (Cronbach’s α = 0.894).
The third section included 20 items related to WIFS and deworming, covering recommended intake schedules, benefits, and common side effects of iron and albendazole tablets. Scoring followed the same binary format (range: 0-20), with satisfactory internal consistency (Cronbach’s α = 0.783) (Appendix 1).
On the day of data collection, students were selected using class-wise, computer-generated random number lists corresponding to school roll numbers. Participants also self-reported common anaemia-related symptoms such as fatigue, dizziness, loss of appetite, and difficulty concentrating. Clinical pallor was assessed by the study investigators under natural daylight through inspection of the lower palpebral conjunctiva.
Anthropometric measurements were performed following World Health Organization (WHO) protocols. Body weight was measured to the nearest 0.1 kg using calibrated analogue weighing scales, and height was recorded to the nearest 0.1 cm using a fixed, non-stretchable measuring tape. BMI was calculated and categorized using WHO BMI-for-age percentile charts into five groups: severe thinness (< 3rd percentile), thinness (3rd- < 15th), normal (15th- < 85th), overweight (85th- < 97th), and obesity (≥ 97th percentile) [22].
In addition to knowledge, data on attitudes toward anaemia and practices related to WIFS and deworming-such as perceived vulnerability, severity, and self-reported consumption of tablets-were also collected as part of the broader mixed-methods study. These findings are reported separately in a dedicated manuscript focused on programmatic barriers and enablers of iron and folic acid supplementation and deworming in school settings [9].
Statistical analysis
Data were entered in Microsoft Excel and analyzed using Jamovi software (version 2.3.26). Descriptive statistics were used to summarize participant characteristics and knowledge responses. The distribution of knowledge scores related to IDA, WIFS, and deworming was assessed using Q-Q plots and the Kolmogorov-Smirnov (K-S) test. As the scores were not normally distributed (K-S test, p < 0.001), non-parametric tests were employed for group comparisons. The Mann-Whitney U test was used for binary variables, and the Kruskal-Wallis test was applied for variables with more than two categories. Where applicable, Dunn’s post hoc test with Bonferroni correction was performed for multiple comparisons. Spearman’s rank correlation coefficient (ρ) was used to examine the relationship between knowledge scores and the number of anaemia-related symptoms. A two-tailed p-value < 0.05 was considered statistically significant.
Results
Knowledge regarding IDA among participants varied widely, with correct responses ranging from 87 (10.3%) to 556 (66.0%). The least known item was the role of walking barefoot in increasing the risk of hookworm infestation (87; 10.3%), while the most commonly identified was that consuming iron-rich foods helps prevent anaemia (556; 66.0%). The median IDA knowledge score was 14 (interquartile range (IQR): 7-18; range: 0-33). For WIFS and deworming, correct responses ranged from 99 (11.7%) to 794 (94.2%). The least known item was that iron tablets can cause constipation (99; 11.7%), while the highest correct response was recorded for identifying the false statement that deworming tablets have no benefit (794; 94.2%). The median WIFS knowledge score was 9 (IQR: 6-11; range: 3-20) (Table 1).
The median age of participants was 15 years (IQR: 14-15; range: 12-18), with a slightly higher proportion of females (442 (52.4%)) than males (401 (47.6%)). The median PCMI was USD 15.3 (IQR: 10.2-21.4). Nutritional assessment showed that 116 (13.8%) participants were malnourished, including 86 (10.2%) with thinness, 10 (1.2%) with severe thinness, and 20 (2.4%) who were overweight (Figure 1). Fatigue was the most frequently reported symptom of anaemia (491; 58.2%), followed by difficulty concentrating (238; 28.2%) and loss of appetite (136; 16.1%). Clinical pallor was observed in 427 (50.7%) participants (Figure 2).
Doughnut diagram showing distribution of the study participants as per their nutritional status (n = 843)
Bar chart showing distribution of the study participants as number of reported signs or symptoms of IDA (n = 843)IDA: Iron deficiency anaemia
Knowledge regarding IDA was significantly associated with age, educational grade, caste, number of anaemia-related symptoms, parental literacy, diet type, and nutritional status (p < 0.001). Post hoc comparisons revealed significantly higher knowledge among participants aged 14 years (mean rank difference = 61.334; p = 0.029), 15 years (88.442; p = 0.001), and ≥ 16 years (135.550; p < 0.001) compared to those aged < 14 years. Those aged ≥ 16 years also outperformed 14-year-olds (74.216; p = 0.002) and 15-year-olds (47.108; p = 0.043). Students in Standards 9 and 10 had higher scores than those in Standard 8 (85.416; p < 0.001 and 55.536; p = 0.007, respectively). Participants from Other Backward Class (OBC) (133.138; p < 0.001), Scheduled Caste (SC) (100.716; p < 0.001), and Scheduled Tribe (ST) groups (133.283; p = 0.018) scored significantly higher than the General category. IDA knowledge increased with the number of anaemia-related symptoms: Those reporting one symptom (69.812; p = 0.014), two symptoms (139.225; p < 0.001), and ≥ 3 symptoms (217.503; p < 0.001) had progressively higher scores than those with none, with all pairwise comparisons statistically significant. Additionally, higher knowledge was observed among participants whose fathers (p < 0.001) or mothers (p < 0.001) were literate, those consuming a non-vegetarian diet (p < 0.001), and those with normal nutritional status (p = 0.001).
Knowledge regarding WIFS and deworming was significantly associated with age, educational grade, caste, number of anaemia-related symptoms, gender, per capita monthly income (PCMI), parental literacy, and dietary practices (p < 0.001). Participants aged 15 years had significantly higher knowledge than those aged < 14 years (93.890; p = 0.001) and 14 years (43.486; p = 0.033), while those aged ≥16 years scored higher than participants aged <14 years (131.340; p < 0.001) and 14 years (80.936; p = 0.001). Students in Standards 9 and 10 had greater knowledge than those in Standard 8 (82.046 and 95.584; both p < 0.001). OBC (133.651; p < 0.001) and SC participants (90.282; p < 0.001) had higher scores than the General category. Knowledge increased with the number of reported anaemia symptoms: Those with one (61.704; p = 0.029), two (171.737; p < 0.001), and ≥ 3 symptoms (190.182; p < 0.001) had significantly higher scores than those with none. Participants from the lowest PCMI quartile (Q1) had lower knowledge than those in Q2 (76.191; p = 0.005), Q3 (66.263; p = 0.006), and Q4 (82.393; p < 0.001). Male participants had higher WIFS knowledge than females (p < 0.001). Higher knowledge was also associated with literate parents (father and mother: both p < 0.001) and a non-vegetarian diet (p = 0.001), but not with nutritional status.
There was a significant positive correlation between IDA and WIFS-deworming knowledge scores (Spearman’s ρ = 0.546, p < 0.001). IDA knowledge was also significantly correlated with the number of anaemia-related signs or symptoms (ρ = 0.269, p < 0.001), as was WIFS and deworming knowledge (ρ = 0.276, p < 0.001) (Table 2, Figures 3, 4).
Scatter plot depicting the distribution of study participants by the number of reported anaemia-related signs or symptoms and their knowledge scores on IDA, WIFS, and deworming (n = 843)IDA: Iron deficiency anaemia; WIFS: Weekly iron and folic acid supplementation
Pairwise comparison of study participants based on age, reading standard, caste, number of reported signs or symptoms of anaemia and their knowledge scores related to IDA (n = 843)Statistical analysis was performed using the Kruskal–Walli’s test.A: IDA awareness score by age; B: IDA awareness score by reading standard; C: IDA awareness score by caste; D: IDA awareness score by number of reported signs or symptoms of anaemia. E: WIFS and deworming awareness score by age; F: WIFS and deworming awareness score by reading standard; G: WIFS and deworming awareness score by caste; H: WIFS and deworming awareness score by number of reported signs or symptoms of anaemia IDA: Iron deficiency anaemia; WIFS : Weekly iron and folic acid supplementation; OBC: Other Backward Class; SC: Scheduled Caste; ST: Scheduled Tribe
Discussion
This cross-sectional study assessed knowledge related to IDA, WIFS, and deworming among school-going adolescents in four coeducational government schools in Deoghar, Jharkhand, using multistage sampling. While every second student identified iron-rich foods as preventive, only one in every nine surveyed knew that walking barefoot could lead to worm infestation and anaemia. About one in four participants recognized that anaemia could cause menstrual problems or reduce immunity. Knowledge levels were higher among older students, those in higher grades, and those with literate parents, normal nutritional status, or non-vegetarian diets. While nearly nine in ten students recognized the benefits of deworming tablets, only about one in three correctly identified the recommended intake schedule, and just one in six were aware of common side effects such as stomach pain.
In the present study, knowledge regarding the causes of anaemia ranged from 10.3% to 53.1%, which was considerably lower than that reported by Sasmita et al. (84.3%) [20]. Awareness of iron-rich food sources varied between 26.8% and 61.0%, which was comparable to findings from Salam et al. in northern Karnataka (19.4-46.0%) and Verma et al. in western Rajasthan (4.2-56.5%) but notably higher than Subba et al. in Anantapur, Andhra Pradesh (11.6%) [12,13,19]. However, these figures were still lower than those reported by Sasmita et al. (83.5%) [20].
Knowledge regarding dietary practices influencing iron absorption, such as avoiding tea or coffee after meals (63.5%) and consuming vitamin C-rich foods (54.7%), was substantially higher in our study than that reported by Subba et al. (29.2% and 19.5%, respectively) [12]. Recognition of anaemia’s impact on academic performance was also greater in our study (45.8%) compared to Salam et al. (13.6%) [19]. Conversely, awareness of anaemia’s immunological consequences was lower (32.7%) than that observed by Salam et al. (45.0%), possibly due to limited health messaging on systemic effects [19].
Regarding WIFS and deworming, 36.3% of participants knew that iron tablets should be taken weekly similar to Salam et al. (34.6%) [19]. Awareness that IFA tablets may cause black stools was 24.9% in our study, higher than Salam et al. 18.6%) [19]. Knowledge that IFA should be taken after meals (37.7%) was again comparable to Salam et al. (34.1%) [19]. More than half (56.2%) were aware of the biannual deworming schedule, exceeding the proportion reported by Salam et al. (36.1%) [19].
In the present study, knowledge regarding IDA, WIFS, and deworming was significantly higher among older adolescents, which aligns with the findings of Subba et al. and Chainisha et al. from Guntur district of Andra Pradesh, where age was also associated with better awareness [12,14]. We also observed that students in higher standards had greater knowledge, similar to the results reported by Chainisha et al. [14]. Participants with literate parents, especially mothers, had significantly higher knowledge scores in our study, consistent with Subba et al. and Chainisha et al., both of whom identified maternal education as a key determinant [12,14]. A significant association between PCMI and knowledge was also observed in our study, which parallels findings by Chainisha et al. [14]. Additionally, adolescents consuming a non-vegetarian diet had better knowledge scores, in line with Chainisha et al., who reported a significant association between dietary pattern and anaemia awareness [14].
Variations in findings across studies may be attributed to differences in participant profiles and study designs. Our study included both male and female students from Standards 8 to 10, whereas Sasmita et al. focused on students from Standards 5 and 6, Salam et al. on Standards 6 and 7, and Verma et al., Chainisha et al., and Subba et al. exclusively on adolescent girls [12-14,20]. Moreover, Subba et al. and Verma et al. employed a cross-sectional design, while Salam et al. and Sasmita et al. conducted pre-post interventional studies [12,13,19,20]. The inclusion of older students in our study likely contributed to higher knowledge scores, possibly due to increased cognitive maturity and greater exposure to curriculum-based health content. The use of a structured, validated questionnaire and data collection within schools that had ongoing WIFS and deworming programmes likely facilitated better recall and understanding of related content. The strong correlation observed between IDA and WIFS and deworming knowledge scores (ρ = 0.546, p < 0.001) suggested that these topics were often delivered together through integrated school-based messaging. Additionally, knowledge scores increased with the number of self-reported anaemia symptoms (IDA: ρ = 0.269; WIFS: ρ = 0.276; both p < 0.001), indicating that students experiencing symptoms may have paid closer attention to relevant health information.
This study has certain limitations that should be acknowledged. First, it was conducted in four government-run, coeducational schools in a single district, which may limit the generalizability of findings to other settings such as private institutions, rural tribal areas, or out-of-school adolescents. Second, although the questionnaire demonstrated high internal consistency, the reliance on self-reported responses may have led to recall bias or overestimation of knowledge, particularly in domains where personal experience with symptoms may influence responses. Third, due to the cross-sectional design, the observed associations, such as higher knowledge among students with more anaemia-related symptoms or those with better nutritional status, should be interpreted as correlational rather than causal.
Conclusions
This study found that school-going adolescents in Deoghar had limited knowledge of IDA, WIFS, and deworming. While awareness of dietary prevention was relatively common, understanding of parasitic causes, correct tablet schedules, and side effects was low. Knowledge was significantly higher among older students, those in higher grades, with literate parents, more anaemia-related sign or symptoms, non-vegetarian diets, and normal nutritional status based on BMI. These findings highlight the need for targeted school-based education to address key gaps in anaemia prevention and supplementation awareness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anaemia 6 2025 2025 https://www.who.int/news-room/fact-sheets/detail/anaemia
- 2Prevalence of iron deficiency and iron deficiency anaemia in adolescent girls in a tertiary care hospital J Clin Diagn Res Kumari R Bharti RK Singh K Sinha A Kumar S Saran A Kumar U 0611201710.7860/JCDR/2017/26163.10325 PMC 562074928969109 · doi ↗ · pubmed ↗
- 3Anemia and iron deficiency among school adolescents: burden, severity, and determinant factors in southwest Ethiopia Adolesc Health Med Ther Tesfaye M Yemane T Adisu W Asres Y Gedefaw L 189196620152671973610.2147/AHMT.S 94865 PMC 4687608 · doi ↗ · pubmed ↗
- 4Attention for and awareness of anemia in adolescents in Karnataka, India: a qualitative study P Lo S One Gillespie B Katageri G Salam S 018202310.1371/journal.pone.0283631 PMC 1007543537018289 · doi ↗ · pubmed ↗
- 5Anaemia in Indians aged 10-19 years: prevalence, burden and associated factors at national and regional levels Matern Child Nutr Scott S Lahiri A Sethi V 018202210.1111/mcn.13391 PMC 948089735719126 · doi ↗ · pubmed ↗
- 6National Family Health Survey-5: 2019-2021—State Fact Sheet, Jharkhand Sciences International Institute for Population Sciences Ministry of Health and Family Welfare, Government of India 2022 https://www.dhsprogram.com/pubs/pdf/OF 43/OF 43.JH.pdf
- 7Operational framework: weekly iron and folic acid supplementation programme for adolescents 6 2025 2012 https://nhm.gov.in/images/pdf/programmes/wifs/operational-framework-wifs/operational_framework_wifs.pdf
- 8National deworming day 6 2025 2015 https://nhm.gov.in/index 1.php?lang=1&level=3&sublinkid=1454&lid=803