Factors influencing recurrence after in-hospital treatment of odontogenic-related oromaxillofacial infections: a single-centre experience
Andreas Sakkas, Majeed Rana, Mario Scheurer, Robin Kasper, Marcel Ebeling, Frank Wilde, Alisa Schramm, Jasmin Engelbrecht

TL;DR
This study identifies factors like age, BMI, and specific clinical symptoms that increase the risk of infection recurrence and longer hospital stays after treating oromaxillofacial infections.
Contribution
The study provides new insights into predictors of infection recurrence and hospital length of stay in odontogenic-related oromaxillofacial infections.
Findings
Older age, higher BMI, and mandibular infections are linked to higher recurrence risk.
Postoperative ICU stay increases recurrence risk by 9.13-fold.
Elevated inflammatory markers and specific clinical symptoms at admission are associated with worse outcomes.
Abstract
Evidence regarding specific factors influencing recurrence after treatment of oromaxillofacial infections is limited. This study aimed to evaluate the incidence and identify predictors of recurrence following in-hospital treatment. A secondary aim was to analyze associations between patient- and procedure-specific variables, treatment outcomes, and hospital length of stay (LOS), and to identify high-risk patients. In this retrospective, single-center study, patients with odontogenic-related oromaxillofacial infections treated surgically or conservatively over a 4-year period were included. Demographic, clinical, radiological, and treatment data were analyzed. Multivariable analyses were performed to identify predictors of recurrence and LOS. A total of 939 patients (mean age 44.66 ± 22.95 years) met the inclusion criteria. The recurrence rate was 5.01%, and the mean LOS was 3.55 ±…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
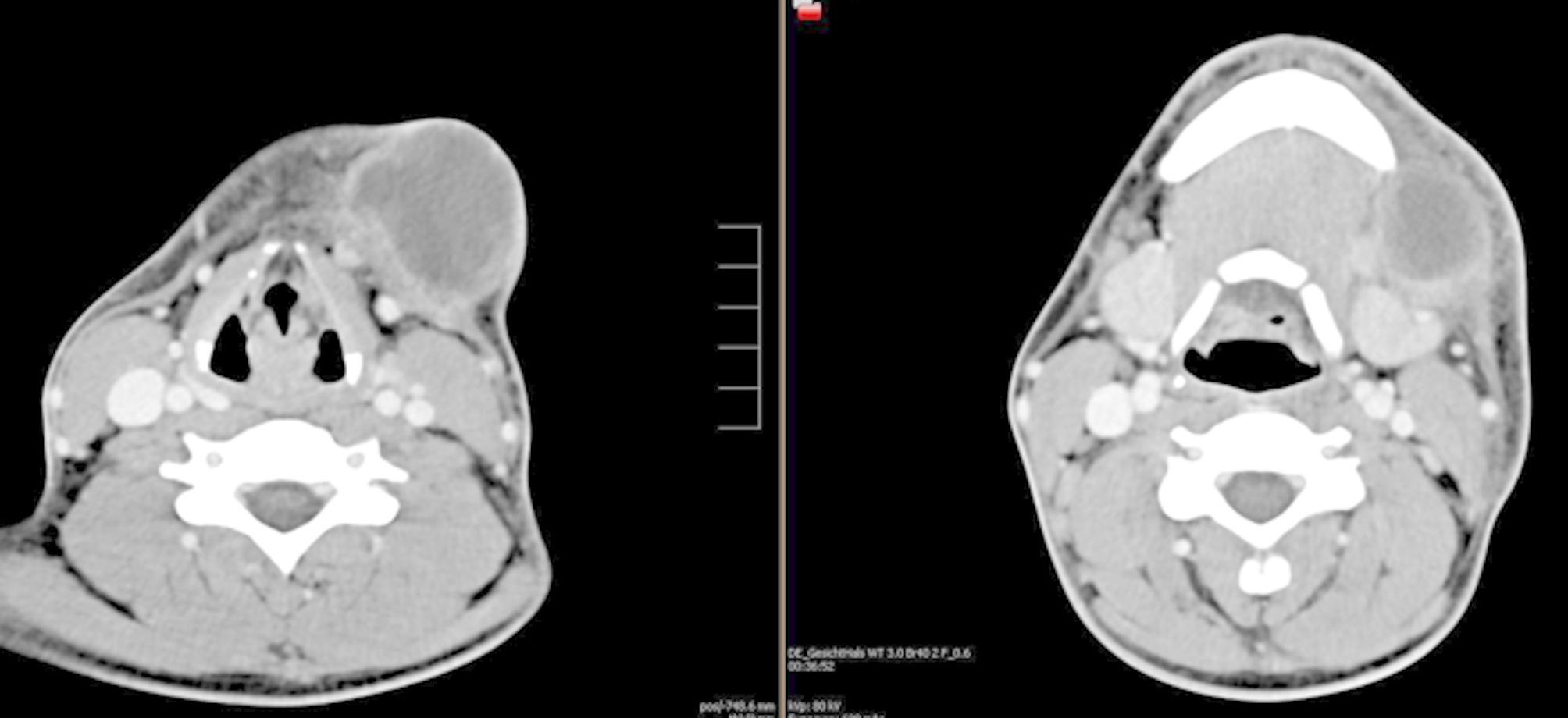 Figure 1
Figure 1 Figure 2
Figure 2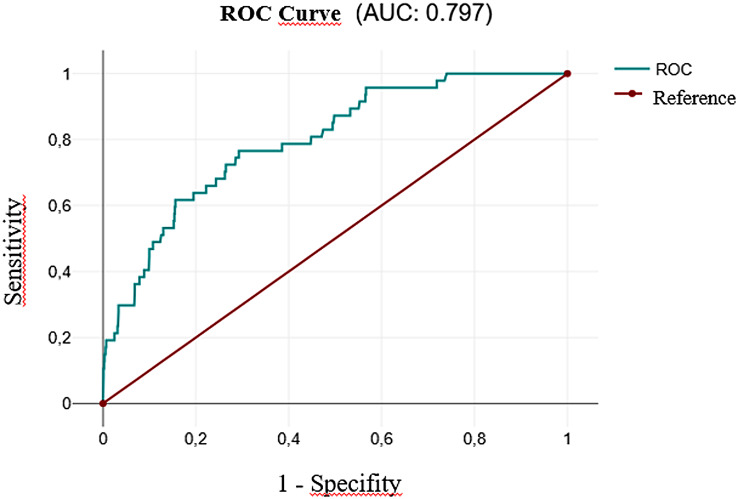 Figure 3
Figure 3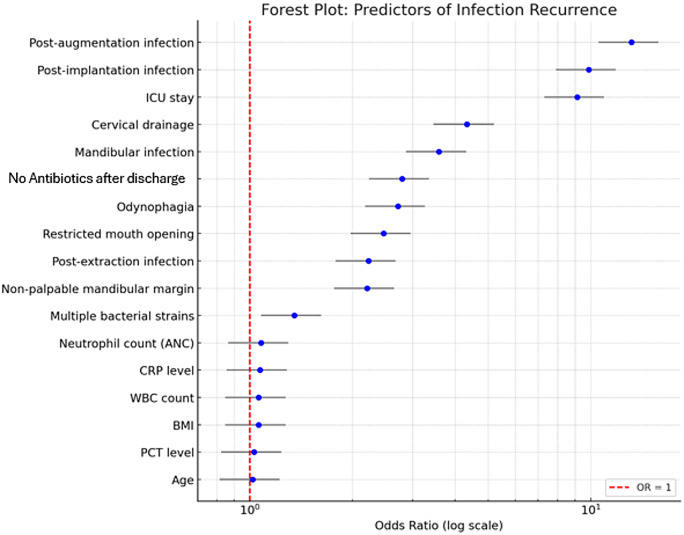 Figure 4
Figure 4- —Universitätsklinikum Ulm (8941)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Infectious Diseases and Tuberculosis · Streptococcal Infections and Treatments
Introduction
Despite improvements in oral health, broader access to dental care, and the widespread use of broad-spectrum antibiotics, infections of the oral and maxillofacial region remain a significant burden on public health systems [1–8]. Several studies have reported a rise in emergency department admissions for these infections, contributing to increasing healthcare costs [1–3, 8].
Oromaxillofacial infections may arise from various odontogenic pathologies, including chronic apical periodontitis, dental caries, and pericoronitis, as well as complications following dental procedures such as implant placement, bone grafting, or osteomyelitis of different origins with or without prodromic symptoms, with and without preoperative medications and operations to reduce the incidence [3, 5, 9–14]. Microbiological studies revealed mixed bacterial flora, predominantly composed of oral commensals with variations based on the specific oral site [11, 15–17].
Treatment of infections in this anatomically complex region is challenging. Factors such as bacterial virulence, impaired host immunity, and inadequate treatment can allow infections to spread to deep spaces of the head and neck, resulting in severe complications, prolonged hospitalization, ICU admissions, and even mortality [1–7, 9–11]. Rapid diagnosis and appropriate therapy are critical for favorable outcomes, reduced hospitalization times, and prevention of systemic complications, as emphasized in previous studies [9–11].
Diagnostic workup should include comprehensive clinical and radiological evaluations to support differential diagnosis [7, 11]. Therapeutic management depends on various factors, including the source and severity of infection. Key components include airway management, empiric or targeted antibiotic therapy, surgical drainage, removal of the infection source, and appropriate dental treatment [5, 9–11, 18, 19].
Although the need for empiric antibiotic therapy has been debated, it remains necessary until culture-based antimicrobial guidance is available [7, 11]. However, no consensus exists regarding standardized treatment protocols concerning surgical intervention, the type and duration of antibiotic therapy, or criteria for hospitalization [7, 19].
Even after seemingly successful therapy, oromaxillofacial infections may recur. Recurrence may be influenced by patient-related factors (e.g., smoking, immunosuppression, diabetes, antiresorptive therapy), poor oral hygiene, and patient non-compliance. Microbiological factors, including polymicrobial infections and bacterial resistance, can also impair therapeutic success. Furthermore, treatment-related factors such as insufficient antibiotic duration, delayed surgical intervention, inadequate debridement, or residual infection foci can contribute to recurrence.
At our center, odontogenic or iatrogenic infections constitute a frequent cause of hospitalization. Despite advances in diagnostic and therapeutic approaches, infection recurrence remains a significant clinical challenge. However, the specific factors contributing to persistence or recurrence have not been clearly identified in the existing literature.
Understanding the interplay between patient-related, microbiological, and treatment-related factors is critical for preventing recurrence. Clinicians must consider these aspects during treatment planning and educate patients on the importance of oral hygiene and treatment adherence. A comprehensive approach can optimize outcomes and minimize recurrence risk.
The primary aim of this study was to evaluate the incidence and identify factors associated with recurrence of oromaxillofacial infections following in-hospital treatment. The secondary aim was to assess the association between patient- and treatment-specific variables with hospital length of stay (LOS) and to identify high-risk patients.
Methods
Patient cohort
This observational, retrospective single-center study included patients with odontogenic-related oromaxillofacial infections who received either surgical or conservative in-hospital treatment at the Department of Oral and Maxillofacial Surgery between September 2019 and April 2023. Medical records were retrieved from the hospital’s electronic database. Ethical approval was obtained from the Ethics Committee of the Chamber of Physicians in Baden-Württemberg, Ulm, Germany (approval number: 189/23; approval date: 20 July 2023). The study was conducted in accordance with the Declaration of Helsinki (1964) and its subsequent amendments.
Inclusion criteria were: (1) patients of any age, (2) clinically and radiologically confirmed odontogenic-related infections originating from the maxilla or mandible, (3) patients treated surgically (with antibiotics) or conservatively (with antibiotics only), and (4) hospitalization following diagnosis and treatment decision. Exclusion criteria were: (1) non-odontogenic orofacial infections, (2) outpatient treatment only, and (3) incomplete medical records.
Patient screening
Diagnosis of odontogenic-related infections followed a standardized protocol including clinical assessment, laboratory testing, and radiological imaging. Radiological evaluation involved panoramic radiographs and/or computed tomography (CT) scans to assess the infection source, extent, and airway involvement. Clinical assessment focused on swelling, dysphagia, dyspnea, stridor, palpability of the mandibular margin, and mouth opening. Hospitalization and treatment decisions (surgical vs. conservative) were made by board-certified oral and maxillofacial surgeons.
Odontogenic sources included chronic apical periodontitis, dental caries, odontogenic and non-odontogenic cysts, pericoronitis, peri-implantitis, and complications following dental extraction, implant placement, or bone augmentation surgery.
Infection treatment
Antibiotic therapy was initiated at admission and continued until discharge for both surgical and conservatively treated patients. Standard antibiotic regimens included ampicillin-sulbactam (Unacid©) at 3 g three times daily for patients > 70 kg and 2 g three times daily for patients ≤ 70 kg. Pediatric doses were adjusted to 150 mg/kg/day. Patients allergic to penicillin received clindamycin (600 mg three times daily).
Abscess incision was performed intraorally or extraorally under local or general anesthesia, depending on the origin, location, size of the abscess, and the patient’s clinical condition. For extraoral drainage, a submandibular skin-fold incision was made, preserving the marginal branch of the facial nerve. Drainage tubes were inserted following debridement. Microbiological samples were obtained after pus drainage, and wounds were irrigated with disinfectant solutions.
The dental source of the infection, which was considered to have a poor prognosis, was removed either during the same procedure or in a follow-up intervention, depending on clinical severity. This could occur either during hospitalization or at an outpatient follow-up. If the prognosis was positive, the patient was referred to our outpatient clinic or to the referring dental practitioner after completing of the initial in-hospital treatment in order to initiate root canal treatment.
Data collection
Patient data were extracted from electronic hospital records and anonymized prior to analysis. Data collected included: age, gender, body mass index (BMI), smoking status, diabetes mellitus, arterial hypertension, penicillin allergy, laboratory results, infection localization, clinical symptoms at admission (mouth opening, subjective odynophagia, extraoral mandibular margin palpability), infection etiology, treatment method (surgical/conservative), surgical access (intraoral/extraoral), antibiotic therapy details, anesthesia type (local anesthesia, intubation anesthesia, sedation, laryngeal mask), microbiological data, and outcomes (ICU stay, length of stay, recurrence, duration till recurrence).
Radiological findings relevant to abscess formation in orofacial spaces (e.g., paramandibular, submandibular, perimandibular, mouth floor, submental, masseteric, pterygomandibular, parapharyngeal) were documented. Two board-certified radiologists independently reviewed all imaging for interrater reliability (Figs. 1 and 2).
Fig. 1. Axial contrast-enhanced computed tomography (CT) scan demonstrating a perimandibular abscess on the left side. The image shows a hypodense, rim-enhancing fluid collection adjacent to the left mandibular body, with surrounding soft tissue swelling and signs of inflammatory infiltration
Fig. 2. Coronal and axial contrast-enhanced computed tomography (CT) images illustrating the odontogenic origin of the infection. The scans reveal an apical osteolytic lesion associated with the left second mandibular molar, indicating it as the causative focus for the development of the perimandibular abscess
Follow-up
Clinical follow-up assessments were performed to confirm wound healing, resolution of symptoms, and absence of infection recurrence.
Recurrence was defined as the reappearance of infection-related symptoms (e.g., soft tissue swelling, purulent discharge, persistent pain) in the same anatomical location as the initial infection, with radiological evidence present within a follow-up period of 6 months after completion of the initial in-hospital treatment. All patients showing clinical deterioration suggestive of infection recurrence were readmitted for additional in-hospital treatment. Repeat imaging was performed only when recurrence was clinically suspected.
Since post-hospital follow-up care was provided by various referring dental practitioners or maxillofacial surgeons, patients who did not return to our clinic within 6 months after the initial in-hospital treatment and from whom no complications were reported were presumed to have healed successfully. Therefore, aside from the recurrence cohort, it was not possible to collect information on whether the infection source identified during the initial infection in cases with a good prognosis was treated or not after the initial in-hospital treatment. The follow-up period was only documented in the recurrence cohort, which represents the time between the initial in-hospital treatment and the readmission following a recurrence diagnosis.
Study variables
Potential predictor variables included:
- Demographic: Age (< 30, 30–49, ≥ 50 years), gender.
- Anamnestic: BMI (< 25, 25–29.9, ≥ 30), smoking status, diabetes mellitus, arterial hypertension, penicillin allergy.
- Clinical: Etiology, location, jaw involved, clinical symptoms (restricted mouth opening, dysphagia, mandibular margin palpability).
- Laboratory: CRP (mg/dL), WBC (/nL), absolute neutrophil count (%), procalcitonin (ng/mL).
- Microbiology: Number and type of bacterial strains (aerobic/anaerobic).
- Treatment: Treatment method, surgical approach (intraoral/extraoral), antibiotic regimen, ICU admission, hospital length of stay.
Primary outcome: infection recurrence.
Secondary outcome: hospital length of stay (LOS). LOS greater than 5 days (≥ 5) was defined as prolonged.
Statistical analysis
Data were compiled electronically using Microsoft Excel and analyzed with SAS^®^, Release 9.4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were used to summarize baseline characteristics. Categorical variables were expressed as counts and percentages.
The Kolmogorov-Smirnov test confirmed non-normal distribution for age and LOS; thus, LOS and follow-up were reported as medians with ranges. Associations between categorical variables and outcomes were tested using chi-square or Fisher’s exact tests. Multivariable logistic regression models were performed to identify independent predictors for infection recurrence. Predictor variables were selected based on clinical relevance and univariate significance (p < 0.1), while considering the limited number of recurrence events (n = 47) to minimize the risk of overfitting. Variables with excessive missing data (e.g., BMI and PCT) were excluded from the multivariable analysis to minimize bias. The number of predictors included in the model was limited in accordance with the number of observed recurrence events to reduce the risk of overfitting. Spearman correlations and chi-square tests analyzed associations with LOS. Dichotomization of LOS using a 5-day threshold for statistical analysis was avoided, as this cutoff value is based primarily on clinical experience rather than evidence-based outcome data. To preserve the full variability and potential prognostic value of this parameter, LOS was retained as a continuous variable in the analysis. A p-value ≤ 0.05 was considered statistically significant.
Results
Demographic distribution
A total of 939 patients met the inclusion criteria. The cohort consisted of 532 males (56.6%) and 407 females (43.3%), yielding a male-to-female ratio of 1.30:1. The mean age at admission was 44.66 ± 22.95 years, ranging from 0 to 95 years. Patients aged ≥ 50 years represented the largest subgroup (n = 393; 41.8%). The most frequent age group among males (n = 196; 36.8%) and females (n = 197; 48.4%) was ≥ 50 years. A total of 246 patients (26.20%) reported being active smokers. The distribution of demographic, anamnestic, microbiological, and treatment-related predictor variables in relation to infection recurrence is summarized in Table 1.
Table 1. Distribution of predictor variables in correlation with infection recurrenceNo infection recurrenceInfection recurrencePredictor variablesp valuen% of variable groupn% of variable group% of recurrenceTotal% of the sample Demographic variables
Age at admission 0.093*< 30 years25796.25%103.75%21.28%26728.43%30–50 years26896.06%113.94%23.40%27929.71%≥ 50 years36793.38%266.62%55.32%39341.85% Gender male51095.86%224.14%46.81%53256.66%0.162**female38293.86%256.14%53.19%40743.34% Anamnestic variables
BMI 0.126*< 2518193.30%136.70%27.65%19420.66%25–308087.91%1112.09%23.40%919.69%≥ 305787.69%812.31%17.02%656.92%NA57497.45%152.54%31.91%58962.73% Smoking status 0.530Yes23294.31%145.69%29.79%24626.20%No65295.32%324.68%68.09%68472.84%suspended888.89%111.11%2.13%90.96% Diabetes mellitus 0.155Yes9392.08%87.92%17.02%10110.76%No79995.35%394.65%82.98%83889.24% Arterial hypertension 0.366Yes21482.98%146.14%29.79%22824.28%No67895.36%334.64%70.21%71175.72% Penicillin allergy 0.454*Yes3892.68%37.32%6.38%414.37%No85495.10%444.90%93.62%89895.63% Microbiology variables
Bacteria culture 0.053**aerobic10891.53%108.47%28.57%11818.82%anaerobic17394.02%115.98%31.43%18429.35%both10191.82%98.18%25.71%11017.54%normal flora21097.67%52.33%14.29%21534.29% Treatment variables
Treatment method 0.950Surgical intervention + antibiotics83394.98%445.02%93.62%87793.40%Antibiotics only5995.16%36.38%4.84%626.60% Surgical approach für drainage 0.001cervical5885.29%1014.71%22.73%687.75%intraoral71996.12%293.88%65.91%74885.29%both5691.80%58.20%11.36%616.96% Preoperative antibiotic therapy 0.480Yes23195.85%104.15%21.28%24125.67%No66194.70%375.30%78.72%69874.33% Antibiotic therapy after discharge 0.025Yes22397.81%52.19%10.64%22824.28%No66994.09%425.91%89.36%71175.72% Postoperative stay in ICU 0.003**Yes969.23%430.77%8.51%131.38%No88395.36%434.64%91.49%92698.62%Abbreviations: n=Number; %=Percentage; NA=Not applicable; ICU=Intensive Care Unit Mann-Whitney U-Test; ** Chi²-Test; *** Fisher’s exact Test^1^related to 627 patients with microbiology test
Etiology and location
Infections were located in the mandible in 66.67% of cases (n = 626) and in the maxilla in 33.33% (n = 313). Chronic apical periodontitis was the leading cause (58.15%; n = 546), followed by post-extraction infections (18.10%; n = 170) and dental caries (16.19%; n = 152).
The most frequently involved anatomical spaces were the paramandibular space (n = 294; 31.31%), canine fossa (n = 180; 19.17%), and perimandibular space (n = 118; 12.57%). The infection most commonly affected the first molar region (n = 188; 20.02%), followed by the third molar (n = 160; 17.04%) and the anterior teeth region (n = 155; 16.51%). Table 2 presents the distribution of clinical variables, including etiology and infection site characteristics, in correlation with infection recurrence.
Table 2. Distribution of clinical variables in correlation with infection recurrenceNo infection recurrenceInfection recurrence Clinical variables Total p value n% of variable groupn% of variable group% of recurrence Etiology of infection Chronic apical parodontitis52095.24%264.76%55.32%546 0.687* Post-extraction15591.18%158.82%31.91%170 0.012* Caries15199.34%10.66%2.13%152 0.056* Pericoronitis24100%00%0%24 0.627** Parodontitis17100%00%0%17 1.000** Post implantation466.67%233.33%4.26%6 0.032** Post augmentation360%240%4.26%5 0.022** Post anterior tooth trauma5100%00%0%5 1.000** Post explantation3100%00%0%3 1.000** Post apicectomy2100%00%0%2 1.000** Unsuccessful extraction attempt2100%00%0%2 1.000** Tooth preparation trauma00%1100%2.13%1 0.050** Globulomaxillary cyst1100%00%0%1 1.000** follicular cyst1100%00%0%1 1.000** Post implant exposure1100%00%0%1 1.000** Spontaneous implant failure1100%00%0%1 1.000** Periimplantitis1100%00%0%1 1.000** Infected gingival cyst1100%00%0%1 1.000**
Location of infection Paramandibular28496.6%103.4%21.28%294 0.128* Canine fossa17697.78%42.22%8.51%180 0.057* Perimandibular10891.53%108.47%21.28%118 0.065* Submucous61100%00%0%61 0.067** Submandibular5289.66%610.34%12.77%58 0.063** Paramaxillary posterior43100%00%0%43 0.162** Posterior floor of the mouth3892.68%37.32%6.38%41 0.454** Pterygomandibular3291.43%38.57%6.38%35 0.413** Buccal3291.43%38.57%6.38%35 0.413** Palatal15100%00%0%15 1.000** Anterior floor of the mouth1071.43%428.57%8.51%14 0.056** Paramaxillary anterior14100%00%0%14 1.000** Submental1184.62%215.38%4.26%13 0.135** Mental8100%00%0%8 1.000** Periodontal4100%00%0%4 1.000** Parapharyngeal266.67%133.33%2.13%3 0.143** Retromaxillary266.67%133.33%2.13%3 0.143**
Affected jaw
0.002* Maxilla30798.08%61.92%12.77%313Mandible58593.45%416.55%87.23%626 Mouth opening
0.003* Normal49096.84%163.16%34.04%506Restricted38592.55%317.45%65.96%416NA17 Subjective odynophagia
0.001 Yes17890.36%199.64%40.43%197No71496.23%283.77%59.57%742 Extraoral palpability of the mandibular basal margin
0.018 Palpable43595.19%224.81%53.66%457Non-palpable14389.94%1610.06%39.02%158NA324Abbreviations: n = number; %=percentage; NA = not applicable; ICU = Intensive Care Unit* Chi²-Test; ** Fisher’s exact Test
Clinical symptoms and laboratory findings
Upon admission, restricted mouth opening was observed in 416 patients (44.30%). Dysphagia was reported by 197 patients (20.98%), and dyspnea by 11 patients (1.17%).
Among patients with mandibular infections (n = 626), the mandibular basal margin was non-palpable in 159 cases (25.40%).
Body temperature at admission was recorded in 720 patients, with a mean of 36.85 ± 0.66 °C (range: 35.0–40.0 °C). Normothermia (36.3–37.4 °C) was observed in 523 cases (55.70%). Associations between continuous numeric variables and infection recurrence were further assessed using linear regression models, as shown in Table 3.
Table 3. Linear regression analysis of numeric predictor variables and infection recurrenceInfection recurrence n meanSDMinimumMaximump value Age
0.009* No89244.2122.89095Yes4753.1722.91092 BMI ^¤^
0.031* No31823.956.7810.546.28Yes3226.645.6215.7940.15 Temperature °C ^¤^
0.889** No68636.850.663540Yes3436.90.7835.839.2 CRP (mg/dl) ^¤^
0.004** No8196.266.440.0637.4Yes4610.49.750.234.61 WBC count (/nL) ^¤^
0.042** No81811.7904.3702.10056.100Yes4713.2305.2306.10033.700 ANC count (%) ^¤^
< 0.001** No81172.469.081495Yes4777.348.654996 PCT level (ng/ml) ^¤^
0.022** No521.596.390.0340.42Yes93.648.990.1127.49 Number of bacterial strains ^¤^
0.022** No5921.111.105Yes351.511.0404Abbreviations: n = number; %=percentage; SD = Standard Deviation; ICU = Intensive Care Unit; BMI = Body Mass Index; CRP = C-Reactive protein; WBC = White Blood Cells; ANC = Absolut Neutrophil Count; PCT = Procalcitonin* t-Test; ** Mann-Whitney U-Test^¤^ relating only to the documented case number
Infection treatment and length of stay
Surgical intervention was performed in 877 patients (93.40%), while 62 patients (6.60%) received conservative antibiotic treatment only. The majority (n = 748; 85.29%) underwent intraoral incision and drainage; 68 patients (7.75%) underwent cervical/submandibular drainage, and 61 patients (6.96%) required both approaches.
Pre-admission antibiotic therapy had been administered to 241 patients (25.67%), most commonly with ampicillin-sulbactam (n = 810; 92.36%) or clindamycin (n = 50; 5.70%). Postoperative antibiotic regimens were similar, with ampicillin-sulbactam prescribed in 804 cases (91.68%) and clindamycin in 48 cases (5.47%). Predictor variables associated with the length of hospital stay are summarized in Table 4.
Table 4. Distribution of predictor variables in correlation with length of stayLength of stay n meanSDMinimumMaximump value Demographic variables
Age at admission < 0.001*< 30 years2672.821.8701230–50 years2793.571.9118≥ 50 years3934.033047 Gender **0.863****Male5323.542.64047Female4073.552.22018 Anamnestic variables
BMI < 0.001*< 251943.352.5901225–30915.515.09147≥ 30655.142.75118 Smoking status **0.154Yes2463.641.78111No6843.512.68047suspended93.671.9416 Diabetes mellitus **0.059Yes1013.892.25014No8383.52.49047 Arterial hypertension **0.001Yes2284.013.47147No7113.42.02018 Penicillin allergy **0.701Yes413.611.91112No8983.542.49047 Microbiology variables
Bacteria culture 0.451*Aerobic1184.152.66118Anaerobic1843.822.05112Both1104.254.56147Normal flora2153.631.94014 Treatment variables
Method of anesthesia < 0.001****Local anesthesia5543.271.52018Intubation anesthesia2664.743.65047Sedation361.170.6104Laryngeal mask211.381.4307No anesthesia623.051.2615 Treatment method Surgical intervention + antibiotics8773.582.530470.193Antibiotics only623.051.2615 Surgical approach für drainage Cervical685.965.41047Intraoral7483.171.77018Both616.032.59118 Preoperative antibiotic therapy 0.222Yes2413.712.09018No6983.492.58047 Antibiotic therapy after discharge 0.013Yes2282.091.29112No7114.012.57047 Postoperative stay in ICU **0.028***Yes1311.2311.21547No9263.441.92018Abbreviations: n = number; %=percentage; ICU = Intensive Care Unit; SD = Standard Deviation Kruskal-Wallis test; ** Mann-Whitney U-test; *** t- test
The mean hospital length of stay (LOS) was 3.55 ± 2.47 days (range: 0–47 days). A prolonged LOS (≥ 5 days) was reported in 227 (24.17%) patients. Thirteen patients (1.38%) required postoperative ICU care, with an average ICU stay of 3.92 ± 5.54 days (range: 1–21 days). The results of the linear regression analysis of clinical variables influencing hospital length of stay are presented in Table 5.
Table 5. Linear regression analysis of clinical variables and length of stayLength of stay n meanSDMinimumMaximump value Clinical variables
Etiology of infection Chronic apical parodontitis5463.542.64147 0.617* Post-extraction1704.282.05012 < 0.001* Caries1522.661.87011 < 0.001* Pericoronitis243.711.417 0.253* Parodontitis173.291.7616 0.870* Post implantation65.836.08218 0.403* Post augmentation55.41.6748 0.019* Post anterior tooth trauma50.60.5501 < 0.001* Post explantation35.673.2128 0.192* Post apicectomy22.50.7123-Unsuccessful extraction attempt23033-Tooth preparation trauma15-55-Globulomaxillary cyst14-44-follicular cyst18-88-Post implant exposure13-33-Spontaneous implant failure15-55-Periimplantitis11-11-Infected gingival cyst12-22- Location of infection Paramandibular2943.111.6012 < 0.001* Canine fossa1802.721.2507 < 0.001* Perimandibular1184.972.15014 < 0.001* Submucous612.331.3906 < 0.001* Submandibular584.481.8819 < 0.001* Paramaxillary posterior432.841.4617 0.016* Posterior floor of the mouth414.462.7118 0.004* Pterygomandibular356.47.32247 < 0.001* Buccal353.771.99110 0.323* Palatal152.670.9814 0.096* Anterior floor of the mouth144.644.07118 0.276* Paramaxillary anterior142.211.2515 0.007* Submental134.692.39110 0.038* Mental82.750.7124 0.260* Periodontal42.52.3816 0.218* Parapharyngeal37.672.08610 0.007* Retromaxillary38.333.21612 0.007*
Affected jaw
< 0.001* Maxilla3132.781.47012Mandible6263.932.76047 Mouth opening
< 0.001* Normal5062.951.61011Restricted4164.363.05047NA171.350.703 Subjective odynophagia Yes1974.983.9047 < 0.001* No7423.161.73012 Extraoral palpability of the mandibular basal margin
< 0.001* Palpable4573.371.8018Non-palpable1595.444.07047NA324----Abbreviations: n = number; %=percentage; NA = not applicable; ICU = Intensive Care Unit* Mann-Whitney U-test
Infection recurrence
Of the 939 patients, 47 (5.01%) experienced postoperative recurrence. Among them, 28 (59.7%) patients had a prolonged LOS. The most common sites of recurrent swelling were the cervical (19.15%), paramandibular (19.15%), submandibular (17.02%), and buccal regions (12.77%).
In 16 patients (34.04%), the primary odontogenic cause was still present at the time of recurrence diagnosis.
Among the patients with recurrence, 41 (87.23%) underwent surgical re-intervention combined with antibiotic therapy, while six (12.77%) were treated conservatively with antibiotics alone.
The mean time to recurrence was 21.7 ± 30.43 days. Significant predictors for infection recurrence identified through multivariable analysis are summarized in Table 6.
Table 6. Significant predictor variables for higher risk of infection recurrenceSignificant predictor variablesOdds Ratio95% CI: x-yp valueHigher risk of infection recurrenceAge1.020.9–1.10.009≥ 50 yearsBMI1.060.9–1.20.031≥ 30Affected jaw3.591.5–8.60.002MandibleEtiology of infection2.231.0-3.70.012Post-extraction9.873.5–38.00.032Post-implantation13.174.5–38.00.022Post-augmentationMouth opening2.471.1–5.80.003RestrictedOdynophagia2.721.1–6.20.001PresentExtraoral palpability of the mandibular basal margin2.211.0-4.90.018Non-palpableCRP level, mg/dl1.070.9–1.20.004↑WBC count /nL1.060.9–1.20.042↑ANC count (%)1.080.9–1.3< 0.001↑PCT level, ng/ml1.030.8–1.30.022↑Surgical approach for drainage4.331.8–10.40.001CervicalAntibiotic therapy after discharge2.80.1–0.90.025No antibiotic therapyMultiple bacterial strains (≥ 2)1.350.7–2.60.022↑ICU stay9.132.8–29.50.003YesAbbreviations: CI = Confidence interval; BMI = Body Mass Index; CRP = C-Reactive protein; WBC = White Blood Cells; ANC = Absolut Neutrophil Count; PCT = Procalcitonin; ICU = Intensive Care Unit
Clinical recurrence risk score
Based on our multivariable analysis, we developed a structured Clinical Recurrence Risk Score to provide clinicians with an actionable tool for the early identification of high-risk patients with odontogenic oromaxillofacial infections.
The score incorporates key predictors significantly associated with infection recurrence, including age, BMI, mandibular infection, post-extraction, post-implantation and post-augmentation infection, trismus, odynophagia, non-palpable mandibular margin, cervical drainage, elevated inflammatory markers (CRP, WBC, ANC, PCT), polymicrobial infections and postoperative ICU stay.
Each risk factor was weighted according to its odds ratio, resulting in a cumulative score ranging from 0 to 31 points. The proposed risk categories are defined as follows: low risk (0–6 points), moderate risk (7–13 points), and high risk (≥ 14 points).
Patients classified as high-risk — especially those with cervical drainage, ICU stay, or infections following implantation or augmentation procedures — may benefit from more aggressive surgical management, longer hospitalization, and intensified follow-up to reduce recurrence rates.
The internal validation of the Recurrence Risk Score using receiver operating characteristic (ROC) analysis yielded an area under the curve (AUC) of 0.797, indicating acceptable discriminatory ability. The ROC curve is shown in Fig. 3.
Fig. 3ROC curve showing the discriminatory ability of the Recurrence Risk Score (AUC = 0.797)
A forest plot summarizing the odds ratios and 95% confidence intervals of significant predictors is shown in Fig. 4.
Fig. 4. Forest plot summarizing the odds ratios and 95% confidence intervals of significant predictors for infection recurrence
Detailed point allocations, predictor characteristics, and their clinical interpretation are summarized in Table 7.
Table 7. Clinical recurrence risk score. Assigned points were derived from the odds ratios using a simplified proportional weighting method, resulting in a cumulative score ranging from 0 to 31 points. The proposed risk categories are defined as follows: low risk (0–6 points), moderate risk (7–13 points), and high risk (≥ 14 points)PredictorORPointsCommentAge1.021Weak individual predictorBMI1.061Additive with ageMandibular infection3.592Strong anatomical risk factorPost-extraction infection2.232Post-implantation infection9.873Highest individual procedure riskPost-augmentation infection13.23Highly vulnerable groupRestricted mouth opening2.472Indicator of disease severityOdynophagia2.722Proxy for deep space involvementNon-palpable mandibular margin2.212Indicates deep or diffuse swellingCRP level, mg/dl1.071Inflammatory burdenWBC count /nL1.061Standard infection markerANC count (%)1.082Stronger than total WBCPCT level, ng/ml1.031Less specific but relevantCervical drainage4.332Reflects advanced infectionAntibiotic therapy after discharge2.82Suggests postoperative considerationMultiple bacteria strains1.351Suggests complex floraICU stay9.133Strongest overall risk indicatorAbbreviations: OR = Odds Ratio; BMI = Body Mass Index; CRP = C-Reactive protein; WBC = White Blood Cells; ANC = Absolut Neutrophil Count; PCT = Procalcitonin; ICU = Intensive Care Unit
Discussion
This study aimed to assess the incidence of oromaxillofacial infection recurrence after in-hospital treatment and to evaluate the associations between patient- and treatment-related variables, recurrence rate, and hospital length of stay (LOS).
The demographic characteristics of our cohort are consistent with previous studies [20–24]. The recurrence rate of 5.01% observed in our study aligns with the reported range of 3–11% in the literature [2, 21–25]. Liau et al. reported a 4.5% reoperation rate among 672 patients, while Christensen et al. found a higher recurrence rate of 11.2% in a smaller cohort [23, 25]. Differences between studies may result from variations in patient populations, diagnoses, and treatment protocols.
We hypothesized that specific variables would be associated with recurrence and might offer opportunities for outcome improvement. Our multivariate analysis identified key predictors for both recurrence and extended LOS: advanced age, increased BMI, mandibular involvement, infection following extraction or augmentation, clinical symptoms at admission (restricted mouth opening, dysphagia, non-palpable mandibular margin), elevated inflammatory markers (CRP, leukocytes, neutrophils, procalcitonin), and cervical surgical approach.
Older age has been linked to a higher risk of infection recurrence in some studies [23], although other investigations did not find significant associations [22, 24, 26]. In the study by Kaercher et al., reoperation rates were higher in older individuals than in younger people, although the difference was not significant [27]. Possible explanations include reduced immune competence and the presence of comorbidities that impair healing [28–30]. Additionally, elderly patients may face challenges in maintaining postoperative oral hygiene due to reduced mobility.
Increased BMI was significantly associated with both recurrence and LOS in our cohort. Although literature directly addressing this association is scarce, it is plausible that higher adiposity impairs antibiotic distribution, complicates surgical access, and facilitates abscess spread.
Contrary to our initial assumptions, smoking status was not significantly associated with recurrence, in agreement with other studies [22–24, 26].
Mandibular infections posed a significantly higher recurrence risk compared to maxillary infections, increasing the odds of recurrence 3.59-fold. This finding is supported by previous studies reporting a higher complication rate in mandibular infections [24, 31, 32]. The complex anatomy and proximity to multiple fascial spaces may explain the increased surgical difficulty and higher recurrence risk.
Post-extraction and post-augmentation infections were independently associated with higher recurrence rates and increased hospitalization. These findings may reflect tissue trauma, altered bacterial colonization, or postoperative complications following dental interventions.
While no specific abscess location predicted recurrence, infections involving multiple spaces have been associated with increased risk [22–24]. The present study also confirmed that restricted mouth opening, dysphagia, and non-palpable mandibular margins at admission correlated with higher recurrence risk and longer LOS [26, 33]. These clinical signs may reflect advanced disease spread, complicating surgical drainage.
Elevated inflammatory markers (CRP, leukocytes, neutrophils, procalcitonin) were significant predictors of both recurrence and increased hospitalization, corroborating findings from previous studies [3, 23, 24, 26, 34–37]. The magnitude of systemic inflammation may thus serve as a valuable marker for disease severity.
Regarding surgical technique, the use of a cervical approach for drainage was associated with a 4.33-fold higher recurrence risk compared to intraoral access, consistent with previous findings [24, 33]. This may reflect the more extensive spread of infection requiring extraoral drainage.
Interestingly, pre-hospital antibiotic treatment was not significantly associated with recurrence, confirming previous observations [26]. However, patients who received antibiotic therapy after discharge exhibited a higher recurrence risk, possibly reflecting earlier discharge in patients with incomplete infection resolution.
The presence of multiple bacterial strains increased recurrence risk, although specific pathogen types did not. This finding suggests that polymicrobial infections complicate antibiotic selection and treatment effectiveness.
Finally, a postoperative ICU stay was associated with a 9.13-fold increased recurrence risk, highlighting the severe disease burden among these patients.
It is noteworthy that in 61.7% of recurrence cases, the initial infection focus was no longer present at the time of diagnosis. However, persistence of the original focus was not statistically associated with recurrence risk, indicating that recurrence mechanisms are multifactorial and not solely dependent on residual infection.
Our study has several limitations. First, the retrospective design introduces potential biases, including incomplete documentation and variability in clinical management. Second, differences in surgeon experience and inconsistencies in medical record detail may also have influenced the results. The management of the odontogenic source following the initial infection was not evaluated in greater detail due to the retrospective nature of the study and the lack of standardized documentation, particularly for patients referred from external practitioners. As a result, detailed information regarding the timing, extent, and quality of dental/surgical interventions was often incomplete or unavailable. This limits our ability to assess the potential impact of definitive odontogenic treatment on recurrence risk and represents a relevant constraint in the interpretation of our findings. Third, we were unable to provide the duration of follow-up after hospital discharge for the entire study sample. This is because the post-discharge follow-up care was administered by various referring dental colleagues or maxillofacial surgeons. Therefore, a further important limitation is the assumption that patients lost to follow-up did not experience a recurrence. While this approach is commonly used in retrospective analyses, it may have resulted in an underestimation of the actual recurrence rate, particularly if patients with unresolved or recurrent symptoms were less likely to return for follow-up care. This introduces a potential source of attrition bias, as the outcomes of patients not captured in the follow-up period may differ systematically from those who remained under observation. Consequently, the findings—especially regarding recurrence rates and the predictive performance of the risk score—should be interpreted with caution. Furthermore, due to decentralized post-hospital follow-up, data on the post-discharge management of the infection source were unavailable for patients with favorable outcomes. As a result, it was not possible to verify whether definitive treatment was completed in these cases, nor to include them in statistical analyses regarding treatment adequacy and recurrence risk. Fourth, variability in LOS and patient compliance post-discharge may limit generalizability. We acknowledge the limited statistical power in subgroups of certain variables with small sample sizes. Variables with substantial missing data were excluded from the multivariable models to preserve model validity. Fifth, the lack of data on oral hygiene status and treatment compliance with postoperative care and medication regimens may potentially influence the risk of recurrence. These patient-related factors are known to play a critical role in the healing process and in the prevention of recurrent infections, particularly in odontogenic maxillary sinusitis. Their absence from the analysis limits the ability to adjust for potentially important confounders and may have influenced the observed recurrence rate. As such, the interpretation of the identified risk factors should take into account the possibility that unmeasured differences in oral hygiene or treatment adherence may have contributed to the outcomes. Sixth, defining LOS as ≥ 5 days as prolonged was arbitrary and not clinically relevant. Therefore, no statistical analysis was conducted to correlate outcomes with a cut-off value of 5 days of LOS as a binary classification. This is because LOS is influenced not only by the variables examined, but also by physicians’ perspectives and institutional financial policies. Using a random value like 5 days could potentially mislead readers to incorrect take-home messages.
The Recurrence Risk Score developed in this study should be interpreted as a preliminary, exploratory and hypothesis-generating tool derived from retrospective data. While the score integrates statistically significant predictors from multivariate analysis, it lacks external validation. Therefore, prospective external validation in independent patient cohorts is a prerequisite before this score can be considered for routine implementation in clinical practice. Until such validation is achieved, the applicability of the score in routine clinical decision-making remains limited. Furthermore, due to the relatively small number of recurrence events and the associated risk of model overfitting, the derived odds ratios and corresponding score weights should be interpreted with particular caution.
Nonetheless, this large patient cohort provides valuable insights into factors associated with infection recurrence and hospitalization duration. Early identification of high-risk patients based on demographic, clinical, and laboratory findings can improve treatment strategies and outcomes. Future prospective studies are warranted to validate these predictors and the introduced risk model and optimize management protocols and its clinical applicability.
Conclusion
The results of this study suggest that increased age and BMI, mandibular involvement, post-extraction or post-augmentation infections, clinical symptoms at admission (restricted mouth opening, dysphagia, non-palpable mandibular margin), elevated inflammatory markers, cervical drainage approaches, and stay in ICU are associated with both a higher risk for recurrence and increased hospital stay. Multiple bacterial strains and no continuous antibiotic therapy after discharge also indicated a higher risk of recurrence, while surgery under intubation anesthesia was linked to an increased length of stay only.
These factors should be identified early and incorporated into the clinical decision-making process. However, the developed Recurrence Risk Score represents a preliminary and exploratory tool and requires prospective external validation in independent cohorts before it can be considered for routine clinical application. A structured, evidence- and experience-based treatment strategy—particularly regarding the choice of surgical approach—may help reduce complication rates, improve outcomes, and shorten hospitalization.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yankov YG, Dimanov S, Nikolaev NI, Stoev L, Yotsova RV, Stoeva M. Etiology and Demographic Distribution of Odontogenic Abscesses in the Maxillofacial Area in Patients Over 18 Years of Age: A Five-Year Retrospective Study. Cureus [Internet]. 2024 Apr 30 [cited 2024 Sep 21]; Available from: https://www.cureus.com/articles/251132-etiology-and-demographic-distribution-of-odontogenic-abscesses-in-the-maxillofacial-area-in-patients-over-18-years-of-age-a-five-year-retrospective-study 10.7759/cureus.593 · doi ↗ · pubmed ↗
- 2Jung J, Oh Y, Cha S, Ohe J. An analysis of contributing factors of head and neck space infections of odontogenic origin: A long-term retrospective clinical study (including COVID-19 pandemic period). Med Oral. 2020;0–0.10.4317/medoral.26018 PMC 1063562137330958 · doi ↗ · pubmed ↗
- 3Zawiślak E, Nowak R. Odontogenic Head and Neck Region Infections Requiring Hospitalization: An 18-Month Retrospective Analysis. Khani Jeihooni A, editor. Bio Med Research International. 2021;2021:1–8.10.1155/2021/7086763 PMC 783477833532496 · doi ↗ · pubmed ↗
- 4Loperfido A, Stasolla A, Giorgione C, Mammarella F, Celebrini A, Acquaviva G et al. Management of Deep Neck Space Infections: A Large Tertiary Center Experience. Cureus [Internet]. 2023 Feb 14 [cited 2024 Sep 21]; Available from: https://www.cureus.com/articles/138589-management-of-deep-neck-space-infections-a-large-tertiary-center-experience 10.7759/cureus.34974 PMC 1001955336938157 · doi ↗ · pubmed ↗