Early pandemic associations of latitude, sunshine duration, and vitamin D status with COVID-19 incidence and fatalities: A global analysis of 187 Countries
Reagan M. Mogire

TL;DR
This study found that higher latitude and lower vitamin D levels were linked to more severe COVID-19 outcomes in 187 countries during the early pandemic.
Contribution
The study provides a global analysis linking environmental and vitamin D factors to early pandemic outcomes.
Findings
Higher latitude was associated with increased case fatality rates of COVID-19.
Lower 25(OH)D levels were linked to higher mortality and incidence rates.
Sunshine duration showed a negative association with case fatality rates.
Abstract
In the face of the COVID-19 pandemic, understanding the interplay between environmental factors and virus spread is crucial for global preparedness strategies. This study explores how geographic latitude, sunshine duration, and vitamin D status were associated with the incidence and fatality rates of COVID-19 across 187 countries during the crucial early months of the outbreak. Data on the total number of COVID-19 cases by country were obtained from the COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) as of June 30, 2020. Univariate and multivariate regression analyses were conducted to determine the associations between COVID-19 cases and latitude, average hours of sunshine from January to June, and mean 25-hydroxyvitamin D (25(OH)D) levels. The average COVID-19 cumulative incidence and mortality per million population were 2,087 and 69, respectively,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig 1
Fig 1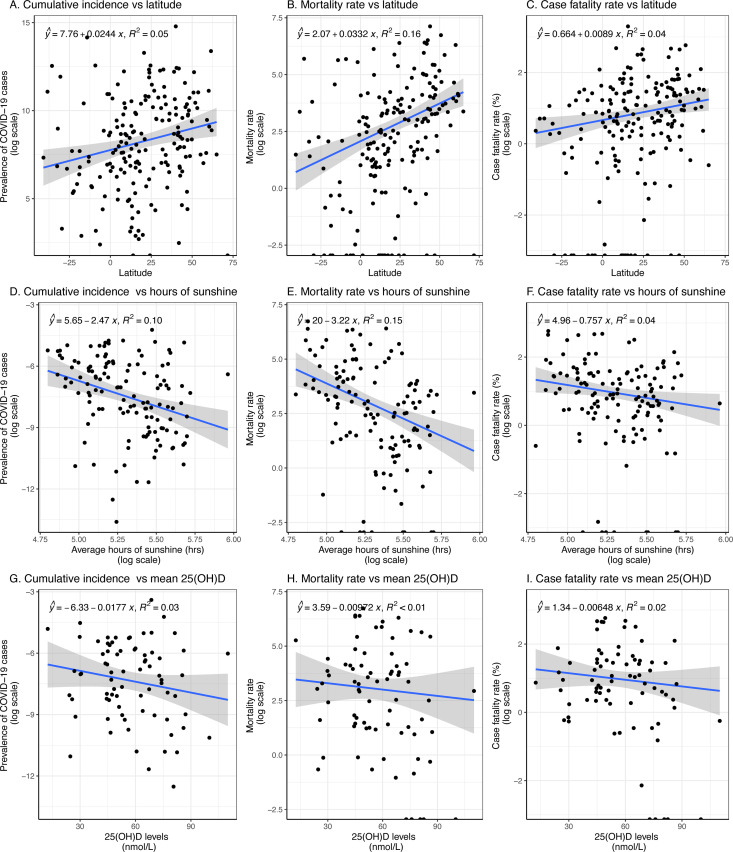 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin D Research Studies · COVID-19 Clinical Research Studies · Vitamin C and Antioxidants Research
Introduction
As of 2024, the COVID-19 pandemic caused by the novel coronavirus SARS-CoV-2 continues to pose significant global health challenges [1,2]. Despite advancements in vaccination and treatment strategies, the virus remains endemic in many regions due to factors such as viral mutations, vaccine hesitancy, and unequal access to healthcare resources [3,4]. The persistent circulation of COVID-19, along with the possibility of future SARS-like epidemics, underscores the urgent need to understand the factors influencing the incidence, transmission, and severity of such infectious diseases [5].
COVID-19 has resulted in substantial morbidity and mortality worldwide. By October 2024, the World Health Organization reported over 770 million confirmed cases and nearly 7 million deaths globally [1]. While factors like age, sex, and underlying comorbidities (e.g., hypertension, diabetes, obesity) have been identified as key determinants of disease severity [6], disparities in COVID-19 incidence and outcomes among different countries and populations suggest that additional factors may contribute to these variations [7].
Notably, some countries with limited healthcare infrastructure and high population densities in Africa experienced relatively lower COVID-19 incidence and mortality rates than other countries [8]. In contrast, populations of African descent residing in temperate regions such as the United States and the United Kingdom have been disproportionately affected, exhibiting higher rates of severe disease and mortality compared to other ethnic groups [9,10]. These disparities have prompted investigations into environmental and nutritional factors, including the potential role of vitamin D status, that may influence susceptibility to and outcomes from COVID-19 [11,12].
Vitamin D deficiency has emerged as a potential modifiable risk factor affecting COVID-19 outcomes [13,14]. Vitamin D, primarily obtained through skin synthesis upon exposure to ultraviolet B (UVB) radiation from sunlight, plays a crucial role in modulating immune function [15]. Several studies have suggested that low vitamin D levels may be associated with an increased risk of respiratory infections, including COVID-19 [16,17]. Early in the pandemic, several experts advocated vitamin D supplementation to mitigate respiratory viral infections, citing evidence from previous influenza and coronavirus outbreaks [18]. Moreover, geographical factors such as latitude and sunshine duration, which influence the endogenous production of vitamin D, may contribute to the observed differences in COVID-19 incidence and mortality rates across regions [19].
Previous research examining the associations between COVID-19 outcomes and factors like latitude, sunshine exposure, and vitamin D status has often been limited to specific cities or regions, potentially restricting the generalizability of the findings [20–22]. To address this gap, a comprehensive analysis was conducted on data from 187 countries to investigate the relationships between COVID-19 cumulative incidence, mortality rate, case fatality rate (CFR), and factors such as latitude, sunshine duration, and mean vitamin D status. Understanding these associations is critical not only for enhancing current public health interventions against COVID-19 but also for preparing for future respiratory epidemics [23,24]. Insights gained from this study may inform strategies for prevention and management, including nutritional interventions and policies aimed at mitigating the impact of COVID-19 and similar infectious diseases.
Methods
This study utilized open-access COVID-19 data from the COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University, available at https://github.com/CSSEGISandData/COVID-19. The dataset includes daily cumulative cases and deaths from January 2020, when only China had reported cases, up to June 30, 2020, covering the transition into summer in the Northern Hemisphere on June 21, 2020.
COVID-19 data were primarily analyzed as of June 30, 2020, serving as the central reference point for this study. For comparative analysis, data from two additional dates—March 31 and September 30, 2020—were also examined. Multiple entries for each country, including data reported for individual states or provinces, were aggregated to provide a single, comprehensive value for each country. Country population data were obtained from the United Nations’ World Population Prospects 2019 Revision [25]. Monthly average sunshine duration data for each country were sourced from the World Meteorological Organization (WMO) [26]. Mean 25-hydroxyvitamin D (25(OH)D) levels for countries were compiled from published literature, prioritizing national surveys. Where unavailable, community-based studies or country-level data were used.
For the analyses, cumulative incidence was defined as the number of COVID-19 cases per one million population in a country. The mortality rate was defined as the number of deaths per one million population. The case fatality rate (CFR) was calculated as the percentage of confirmed COVID-19 patients who died (number of deaths divided by the number of confirmed cases, multiplied by 100) in a country.
Statistical analyses were conducted using R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria), available at https://www.R-project.org/. Variable normality was evaluated using the Kolmogorov-Smirnov test. To enable parametric analyses, numbers of COVID-19 cases and deaths, along with other parameters, were log-transformed to approximate a normal distribution. However, mean values were calculated from untransformed data for descriptive statistics. Associations between COVID-19 metrics—cumulative incidence, mortality rate, and case fatality rate—and factors such as latitude, average sunshine duration, and mean 25-hydroxyvitamin D (25(OH)D) levels were explored using univariate and multivariate linear regression models. The multivariate models were adjusted for gross domestic product (GDP) to account for socioeconomic status, elderly dependency ratio (EDR) to capture population aging, and population density to adjust for the differences in transmission potential. Logistic regression, which requires individual-level binary outcomes, were not applicable to this ecological dataset. Scatter plots were used to visualize these relationships for each country, with a p-value of less than 0.05 denoting statistical significance. For analyses involving geographic position, latitudes north of the equator were coded as positive values, indicating greater distance from the equator, while southern latitudes were coded as negative, indicating proximity to the equator. This coding reflects the seasonal variation in sunlight exposure relevant until June, after which the seasons significantly change.
Ethics statement
This study utilized publicly available, aggregated data at the country level from reputable sources such as the World Health Organization and the World Bank. No individual-level or personally identifiable information was collected or analyzed. Therefore, ethical approval and informed consent were not required.
Results
Population characteristics
This study analyzed data up to June 30^th^ from 187 countries across the seven UN world regions (Table 1, Fig 1 and S1 Fig). The dataset included 10,446,927 confirmed COVID-19 cases and 508,459 deaths. The average COVID-19 cumulative incidence and mortality rates per million population were 2,087 and 69, respectively, with an overall CFR of 3.19%.
Table 1: Regional COVID-19 Statistics as of June 30, 2020.
Case fatality rate (%) of COVID-19 by country as at 30th June 2020.Country borders and coastlines are based on Natural Earth data (public domain, https://www.naturalearthdata.com; terms of use: public domain, CC0‑equivalent). Maps were generated in R using the sf, ggplot2, and rnaturalearth packages. Case fatality rate (CFR) was calculated as: (Number of deaths / Number of reported cases) × 100.
Effect of latitude on COVID-19 cumulative incidence, mortality rate, and case fatality rate
Linear multivariate regression analyses demonstrated a positive association between latitude and COVID-19 cumulative incidence (β = 0.012; 95% CI: 0.001, 0.024), mortality rate (β = 0.042; 95% CI: 0.014, 0.070), and CFR (β = 0.030; 95% CI: 0.013, 0.050) (Table 2). Similar trends were observed through March 2020; however, by September 2020, the associations were no longer significant (S1 Table). Scatter plots also showed a positive association between latitude and COVID-19 metrics (Fig 2A, 2B and 2C). Latitude accounted for 5%, 16%, and 4% of the variation in COVID-19 cumulative incidence, mortality rate, and CFR, respectively by the end of June 2020 (Fig 2).
Table 2: Effect of latitude, amount of sunshine and vitamin D status on COVID-19 outcomes.
Correlations between COVID-19 metrics and environmental factors across countries.Each point on the plots represents data for an individual country. The COVID-19 cumulative incidence is defined as the total number of reported cases per 1 million population, the mortality rate as the number of deaths per 1 million population, and the case fatality rate as the percentage of reported cases resulting in death, multiplied by 100.
Effect of sunshine duration on COVID-19 cumulative incidence, mortality rate, and case fatality rate
Univariate analyses suggested an inverse association between the average number of sunshine hours and the parameters investigated; however, these associations were not statistically significant in multivariate analyses–COVID-19 cumulative incidence (β = 0.16; 95% CI: -1.30, 1.62), mortality rate (β = 0.22; 95% CI: -3.06, 3.50), and CFR (β = -1.51; 95% CI: -4.44, 1.41). Similar effects were noted up to the end of March for cumulative incidence and mortality rates, but the association with CFR was not statistically significant. By the end of September, none of these associations remained significant. Scatter plots also indicated an inverse relationship between sunshine duration and COVID-19 metrics (Fig 2D, 2E and 2F). Sunshine duration explained 9.9%, 12%, and 1.4% of the variation in COVID-19 cumulative incidence, mortality rate, and CFR, respectively (Fig 2).
Effect of vitamin D Status on COVID-19 cumulative incidence, mortality rate, and case fatality rate
Mean serum 25(OH)D levels were inversely associated with COVID-19 mortality rate (β = –0.052; 95% CI: –0.094, –0.009) and CFR (β = –0.033; 95% CI: –0.061, –0.006). However, the association between 25(OH)D levels and COVID-19 cumulative incidence was not statistically significant (β = –0.018; 95% CI: –0.041, 0.005; p = 0.13). In March, mean 25(OH)D levels were significantly associated with mortality rate but not with cumulative incidence or CFR (S1 Table). By the end of September, significant associations were observed between mean 25(OH)D levels and COVID-19 mortality rate and CFR, but not with cumulative incidence (S1 Table). Mean 25(OH)D levels explained 3.2%, 2%, and 2.1% of the variation in COVID-19 cumulative incidence, mortality rate, and CFR, respectively (Fig 2).
Discussion
This study investigated the associations between geographical factors, vitamin D status, and COVID-19 outcomes across 187 countries during the first six months of 2020. The findings indicate that the cumulative incidence, mortality rate, and case fatality rate (CFR) of COVID-19 were positively associated with latitude and inversely associated with sunshine duration and mean 25(OH)D levels. These associations were significant up to the end of March 2020 but diminished by the end of September, except for the inverse relationship between mean 25(OH)D levels and COVID-19 cumulative incidence and CFR. These results suggest potential environmental and nutritional influences on COVID-19 outcomes and highlight a temporal dimension to these relationships.
The positive association between latitude and COVID-19 metrics aligns with previous studies. Rhodes et al. (2020) reported higher COVID-19 mortality rates in countries above 35º North latitude compared to those below, suggesting that latitude may play a role in disease severity [8]. Similarly, higher COVID-19 incidence and transmission rates have been observed in cities and countries farther from the equator [27,28]. Benedetti et al. (2020) found that COVID-19 mortality rates were positively correlated with latitude and negatively correlated with average temperature across regions in the United States and Europe [29]. The influence of latitude on COVID-19 outcomes may be attributed to lower sunlight exposure during winter months at higher latitudes, leading to vitamin D deficiency [15]. Additionally, lower temperatures associated with higher latitudes may facilitate viral transmission, as seen in past epidemics like SARS and influenza [30,31].
The inverse associations between COVID-19 cumulative incidence, mortality rate, and CFR with average sunshine duration are consistent with previous research. Byass (2020) reported that the incidence of COVID-19 decreased with increasing solar radiation in various locations across China during January and February 2020 [32]. Furthermore, a study conducted in Jakarta, Indonesia, demonstrated that increased sunlight exposure improved recovery rates among COVID-19 patients [33]. Reduced sunlight exposure may influence COVID-19 outcomes by affecting vitamin D synthesis, which plays a crucial role in immune function [15,16].
Current findings also indicated that mean 25(OH)D levels were inversely associated with COVID-19 mortality rate and CFR. This observation aligns with Laird et al. (2020), who reported that mean 25(OH)D levels in European countries were inversely associated with COVID-19 incidence and mortality rates [21]. Additionally, D’Avolio et al. (2020) found that patients who tested positive for SARS-CoV-2 had significantly lower mean 25(OH)D levels compared to those who tested negative [14]. Vitamin D deficiency may increase susceptibility to COVID-19 by modulating the immune response and influencing the expression of angiotensin-converting enzyme 2 (ACE2), which is involved in viral entry into cells [11]. Elevated ACE2 expression has been associated with increased survival in COVID-19 patients [34]. Moreover, vitamin D deficiency is linked to comorbidities such as hypertension, diabetes, and obesity, which are known risk factors for severe COVID-19 outcomes [6,35].
The waning of the observed associations by the end of September may be attributed to the implementation of control measures, changes in testing rates, or seasonal variations. Increased public health interventions, such as lockdowns and social distancing, could have mitigated the influence of environmental factors on COVID-19 transmission [3,4]. Seasonal changes leading to increased sunlight exposure during the summer months may have improved vitamin D status in populations, potentially affecting disease outcomes [36,37].
It is important to acknowledge that, due to the observational nature of this study, causality cannot be inferred, and confounding factors may influence the relationships observed. Other variables such as government policies, healthcare capacity, socioeconomic status, and population behaviors were not accounted for and could confound the results [8,38]. For instance, Lawal (2021) discussed the paradox of low COVID-19 mortality rates in Africa despite limited healthcare resources, suggesting that factors like younger population demographics and prior exposure to infectious diseases may play a role [8]. Large‑scale educational campaigns can rapidly raise population‑level supplementation rates; for example, targeted outreach in Slovenia increased vitamin D supplementation [39]. Although this study did not measure supplementation directly, such initiatives may partly explain between‑country differences in mean vitamin D status.
A major strength of this study is the inclusion of data from all countries reporting COVID-19 cases and deaths during the study period, which reduces potential selection bias. Additionally, the analysis considered multiple geographical and environmental factors, including latitude, sunshine duration, and vitamin D status, providing a comprehensive overview of potential influences on COVID-19 outcomes. However, several limitations should be acknowledged. First, the observational design limits the ability to establish causal relationships. Second, sunshine duration and mean 25(OH)D levels were not available for several countries, which may affect the generalizability of the findings. Third, other potential confounding factors, such as variations in testing rates, reporting practices, public health interventions, and genetic differences among populations, were not accounted for in the analysis. Furthermore, vitamin D levels were based on mean values from existing literature, which may not accurately reflect current the population status. In addition, each observation in the analyses represented an entire country; sub‑national factors such as urban‑rural residence could therefore not be examined.
This global analysis suggests that higher latitude is associated with increased COVID-19 cumulative incidence, mortality rate, and case fatality rate during the early phase of the pandemic, while higher mean 25-hydroxyvitamin D (25(OH)D) levels are associated with reduced COVID-19 outcomes. These findings indicate potential environmental and nutritional influences on COVID-19 incidence and disease severity, highlighting vitamin D status as a possible contributing factor. However, recent randomized controlled trials have yielded mixed results regarding the efficacy of vitamin D supplementation in preventing or treating COVID-19. Some studies have shown no significant benefit of high-dose vitamin D supplementation on hospital length of stay or mortality [40,41], while others have suggested a reduction in severe outcomes with vitamin D administration [42,43]. Therefore, while observational data support a potential association between vitamin D status and COVID-19 outcomes, causality cannot be established based on current evidence. Considering the ongoing circulation of COVID-19 and the potential for future SARS-like epidemics, understanding the factors that influence disease transmission and severity remains critical. Insights from this study may inform public health strategies aimed at improving population health through safe sun exposure and addressing vitamin D deficiency where prevalent.
Supporting information
S1 TableEffect of latitude, amount of sunshine and vitamin D status on COVID-19 cumulative incidence, mortality rate and case fatality rate by March 31^st^ and September 30^th^ 2020.(DOCX)
S1 FigCumulative incidence (number of COVID-19 cases per one million population) of COVID-19 by country as of June 30^th^ 2020.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organization WH. WHO Coronavirus (COVID-19) Dashboard. 2024 [cited 2024 December 2024]. https://covid 19.who.int/
- 2Fauci AS, Lane HC, Redfield RR. Covid-19—navigating the uncharted. N Engl J Med. 2020:1268–9.32109011 10.1056/NEJ Me 2002387 PMC 7121221 · doi ↗ · pubmed ↗
- 3Burki TK. Lifting of COVID-19 restrictions in the UK and the Delta variant. Lancet Respir Med. 2021;9(8):e 85. doi: 10.1016/S 2213-2600(21)00328-3 34265238 PMC 8275031 · doi ↗ · pubmed ↗
- 4Mallapaty S. Vaccines are curbing COVID: Data from Israel show drop in infections. Nature. 2021;590(7845):197. doi: 10.1038/d 41586-021-00316-4 33547434 · doi ↗ · pubmed ↗
- 5Woolhouse M, Scott F, Hudson Z, Howey R, Chase-Topping M. Human viruses: discovery and emergence. Philos Trans R Soc Lond B Biol Sci. 2012;367(1604):2864–71. doi: 10.1098/rstb.2011.0354 22966141 PMC 3427559 · doi ↗ · pubmed ↗
- 6Jordan RE, Adab P, Cheng KK. Covid-19: risk factors for severe disease and death. BMJ. 2020.10.1136/bmj.m 119832217618 · doi ↗ · pubmed ↗
- 7Ssentongo P, Ssentongo AE, Heilbrunn ES, Ba DM, Chinchilli VM. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. P Lo S One. 2020;15(8):e 0238215. doi: 10.1371/journal.pone.0238215 32845926 PMC 7449476 · doi ↗ · pubmed ↗
- 8Lawal Y. Africa’s low COVID-19 mortality rate: A paradox?. Int J Infect Dis. 2021;102:118–22. doi: 10.1016/j.ijid.2020.10.038 33075535 PMC 7566670 · doi ↗ · pubmed ↗