Surgical preferences in anterior cruciate ligament reconstruction: A cross-sectional study in a low-middle income country
José Fernando Sánchez-Carbonel, José Calmet-Rojas, Fabriccio J. Visconti-Lopez, Diego Urrunaga-Pastor, David Torres-Manrique

TL;DR
This study explores the surgical preferences of Peruvian orthopedic surgeons for anterior cruciate ligament reconstruction, highlighting common techniques and graft choices.
Contribution
This is the first study to report on ACLR surgical preferences among Peruvian orthopedic surgeons.
Findings
The anteromedial portal is the most popular technique for femoral tunnel drilling.
Most surgeons prefer autografts, particularly from hamstring tendons.
There is variability in tourniquet use among surgeons.
Abstract
Anterior cruciate ligament reconstruction (ACLR) is one of the most common surgical procedures in sports orthopedics; however, there is a lack of literature related to this topic in Peru. This study aimed to describe the current surgical preferences in ACLR among Peruvian orthopedic surgeons. An analytical cross-sectional study based on an online survey sent to 500 Peruvian orthopedic surgeons, supplemented with physical surveys distributed during the “IX OrthoTrauma Update” congress held in October 2022 in Lima, Peru. The survey collected demographic characteristics (e.g., residence area, health care sector), employment characteristics (e.g., experience as orthopedic surgeon, experience in ACLR), and surgical preferences for ACLR (choice of femoral tunnel drilling technique, choice of graft, tourniquet use). A total of 162 surgeons responded (32.4%). A total of 134 responses were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
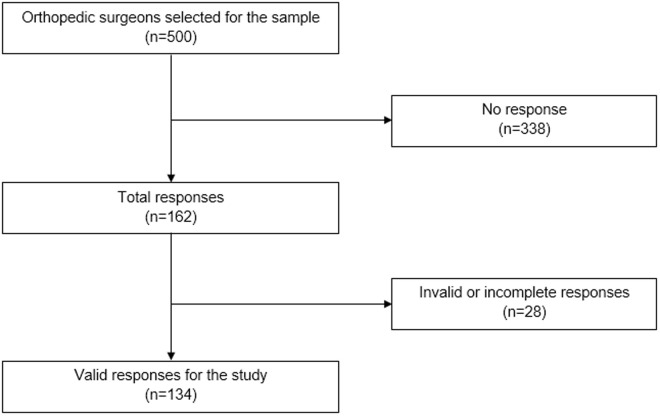 Fig 1
Fig 1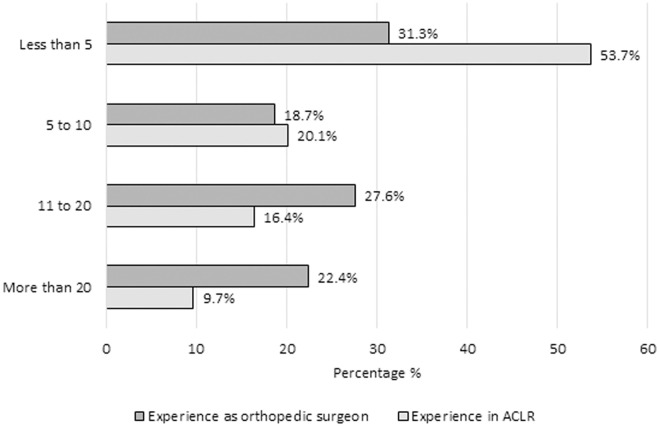 Fig 2
Fig 2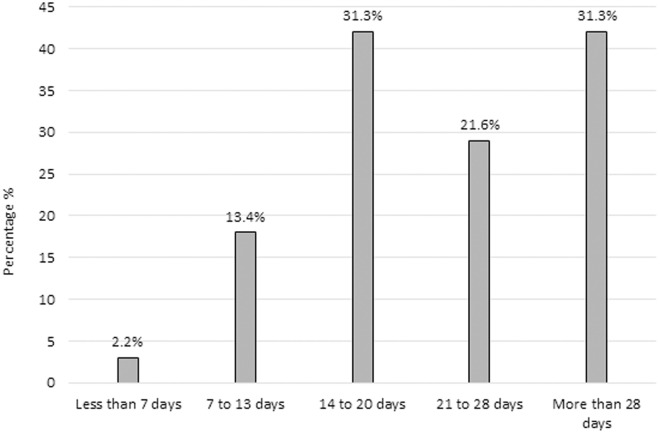 Fig 3
Fig 3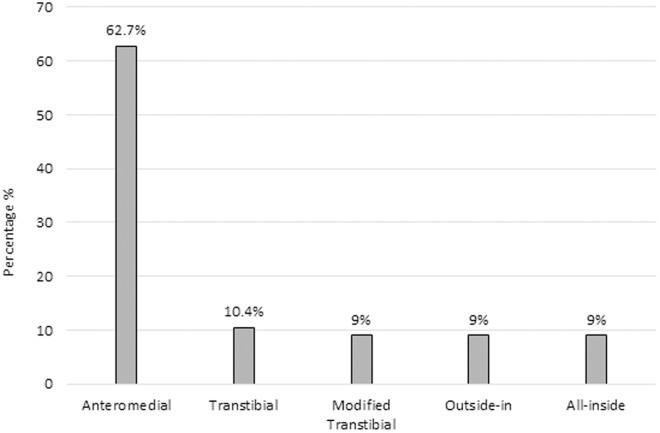 Fig 4
Fig 4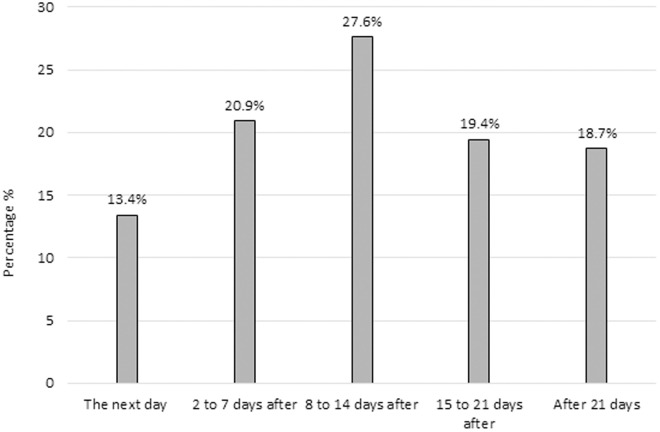 Fig 5
Fig 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Sports injuries and prevention · Total Knee Arthroplasty Outcomes
Introduction
The anterior cruciate ligament (ACL) is the primary stabilizer of the anterior translation of the tibia, and plays a secondary role in controlling knee rotation [1]. ACL injuries are among the most common sports-related injuries. In the United States alone, approximately 120,000 ACL reconstructions are performed annually, reflecting a substantial clinical burden in high-demand populations [2]. Therefore, ACL reconstruction (ACLR) is one of the most common surgical procedures in sports orthopedics, widely performed to address instability and prevent further joint damage [3,4].
The torn ligament is removed and replaced with a graft, which may come from the patient’s own tissue (autograft), from a tissue bank (allograft) or a combination of both (hybrid graft) [5]. The autograft is preferred for its shorter operative time and faster recovery compared to allografts, which are associated with higher failure rates and longer incorporation times [4,6,7]. On the other hand, the success and failure rates of hybrid grafts are similar to those of autografts [8]. Another critical surgical decision involves the femoral tunnel drilling technique, with options including transtibial (TT), anteromedial (AM), outside-in (OI), and all-inside (AI) approaches [7,9]. Studies suggest that the AM technique better replicates the anatomical femoral tunnel compared to TT, while OI and AI techniques offer advantages in specific patient populations, such as those with skeletal immaturity or obesity [9–19].
Studies on new trends in orthopedic surgery are important since they guide orthopedic surgeons in the choice of the most adequate technique and investigate and improve techniques to provide better and more effective treatment [20,21]. Currently, there is literature describing the surgical preferences in ACLR in the United States, Europe and Asia [3,4,22,23]. However, no similar research has been found in Latin America or Peru. Furthermore, the findings of the previously mentioned studies cannot be extrapolated to Peru because the resources available, population type, and level of sports activity are not the same as in high-income countries [24,25]. It is therefore important to investigate the preferences of Peruvian orthopedic surgeons in a context completely different to that of previous studies.
This study describes the surgical preferences of Peruvian orthopedic surgeons regarding ACLR techniques and graft choices. We hypothesize that Peruvian orthopedic surgeons’ ACLR differ from those in high-income countries, potentially influenced by factors such as resource availability, training background, and institutional settings.
Methods
Design and study population
We conducted an analytical cross-sectional study based on surveys sent to a self-selected sample of 500 participants between March and October 2022. The survey was sent to orthopedic surgeons who are members of the Peruvian Society of Orthopedics and Traumatology (SPOT) or who have attended a congress organized by this society and have access to email (Fig 1). This was a census-based study aimed at surveying the entire population of orthopedic surgeons affiliated with SPOT. Therefore, no sample size calculation was performed, as the objective was to include the entire available population.
Flowchart of the study participant selection.
Variable and measurement
We designed an ad hoc instrument in a web application (REDCap®) based on the experience of two authors, an experienced orthopedic surgeon and a medical resident in orthopedic surgery (DTM & JSC) and a previous study [22]. This instrument was composed of two sections: a general data section and a section related to the preferences of ACLR. The instrument was validated following a Delphi methodology by 6 health professionals, including 3 epidemiologists, and 3 orthopedic surgeons. Similarly, a pilot sample of 5 orthopedic surgeons was included to evaluate the clarity and understandability of the content. The modifications suggested were gradually incorporated until the instrument was approved by consensus by the group of experts.
We divided the questionnaire into two parts: 1) Demographic and work-related variables: sex (male, female), age (under 30, 30–40, 41–50, 51–60, 61–70, and over 70 years), area of residence (Lima, Coast without Lima, Highlands and Jungle) and main health care working sector (public hospital, social insurance hospital, private clinic and armed forces); 2) Surgical preferences for ACLR: years as a trauma specialist (less than five years, between five and ten years, between 11 and 20 years, more than 20 years), years of experience in ACLR (less than five years, between five and ten years, between 11 and 20 years, more than 20 years), the time interval in which ACLR is usually performed from day of injury (less than seven days, seven to 13 days, 14–20 days, 21–28 days and more than 28 days), femoral tunnel drilling arthroscopic technique (AM, TT, modified TT, OI, AI), time interval in which physical therapy is usually indicated after ACLR (the next day, two to seven days after, eight to 14 days after, 15–21 days after, after 21 days), type of graft used most frequently for ACLR (autograft, allograft, hybrid graft), choice of anatomical graft site (hamstrings, patellar tendon, quadriceps tendon), tourniquet use during ACLR (always, sometimes, never) and use of any component after performing ACLR (intra-articular corticosteroid, tranexamic acid, platelet-rich plasma, none, others).
Data collection and analysis
The data collection was carried out between 21^st^ March and 31^st^ October 2022. The survey was sent to the institutional emails of the SPOT member surgeons during March and April 2022. Additionally, physical surveys were distributed to all the SPOT members at the “IX OrthoTrauma Update” congress held in October 2022 in the city of Lima, Peru. An identifier was considered to exclude duplicate responses. These surveys were subsequently digitized by the authors in REDCap®. The data collected was exported from the REDCap® platform to a spreadsheet in Microsoft Excel 2020. The analyzed database did not contain identifiers. All analyses were performed using Stata version 18.0 (StataCorp, TX, USA). We used descriptive statistics to summarize the data, reporting absolute and relative frequencies, and 95% confidence intervals for all categorical variables.
Ethical approval
The study protocol was approved by the Ethics Committee of the Universidad Peruana de Ciencias Aplicadas (FCS-SCEI/051-02-22). Respondents to the self-applied survey were provided with detailed information on the conditions, objectives, and benefits of the study. Written informed consent was obtained from all participants prior to their involvement in the study. They were informed that participation was voluntary, and they could withdraw from the study at any time without any consequences. The survey did not contain any data that could personally identify the participants with their responses.
Results
From the total of 500 orthopedic surgeons members of the SPOT, we obtained 162 responses (32.4%) and excluded 28 (17.3%) due to incomplete responses. We analyzed the responses of 134 orthopedic surgeons (Fig 1). Among the sample, 93.3% (n = 125; 95% CI: 87.3–96.7) were male, 47% (n = 63; 95% CI: 38.7–55.5) were younger than 40, and 27.6% (n = 37) were older than 60 years. Also, 61.2% (n = 82; 95% CI: 52.6–69.1) resided in Lima, followed by 33.6% (n = 45; 95% CI: 26.0–42.1) in the coast. Moreover, 53% (n = 71; 95% CI: 44.5–61.3) worked mainly in the private sector and 42% (n = 57; 95% CI: 34.4–51.1) worked in a public or social insurance hospital. Only 4.5% (n = 6; 95% CI: 2.0–9.7) reported working in the armed forces (Table 1).
Table 1: Demographic characteristics and surgical preferences for anterior cruciate ligament reconstruction in the study participants (n = 134).
We found that 50% (n = 67; 95% CI: 41.5–58.5) of respondents had more than 10 years of experience as an orthopedic surgeon, whereas 53.7% (n = 72; 95% CI: 45.2–62.1) had less than 5 years of experience in ACLR (Fig 2). Regarding the interval of time in which ACLR is performed from day of injury, 31.3% (n = 42; 95% CI: 24.0–39.8) of the participants reported preferring to perform surgery between day 14–20 and later than 28 days after injury. Only 2.2% (n = 3; 95% CI: 0.7–6.8) reported choosing to perform surgery within 7 days after injury (Fig 3).
Distribution of years of experience among orthopedic surgeons in general practice and specifically in anterior cruciate ligament reconstruction (n = 134).
Time interval between injury and anterior cruciate ligament reconstruction among Peruvian orthopedic surgeons (n = 134).
The position of femoral tunnel drilling using the anteromedial portal was the most preferred with 62.7% (n = 84; 95% CI: 54.1–70.5) of answers. In contrast, there were no significant differences between the other options of femoral tunnel drilling: TT, modified TT, OI, and AI (Fig 4). The use of autograft was the most common choice among the participants, representing 85.1% (n = 114; 95% CI: 77.9–90.2) of the total, while 13.4% (n = 18; 95% CI: 8.6–20.4) reported using allograft, and only 1.5% (n = 2; 95% CI: 0.4–5.8) preferred the use of a hybrid graft. Concerning the graft site of choice, 83.6% (n = 112; 95% CI: 76.2–89.0) reported preference for the hamstrings tendon, 16.4% (n = 22; 95% CI: 11.0–23.8) preferred using the patellar tendon, and none of the respondents reported using the quadriceps tendon or another type of graft.
Preferred arthroscopic femoral tunnel drilling techniques in anterior cruciate ligament reconstruction (n = 134).
There were no distinct differences between the use of tourniquet. Thirty-four percent (n = 46; 95% CI: 26.7–42.8) reported never using a tourniquet during surgery, 37.3% (n = 50; 95% CI: 29.5–45.9) reported using it sometimes, and 28.4% (n = 38; 95% CI: 21.3–36.6) always used a tourniquet in their ACLR surgeries. It was found that 65.7% (n = 88; 95% CI: 57.2–73.3) of the surgeons surveyed did not use any compound after completion of the intervention. The most common compound used after surgery by 12.7% (n = 17; 95% CI: 8.0–19.5) of respondents was intra-articular corticosteroids, and 7.5% (n = 10; 95% CI: 4.0–13.4) of respondents reported using hyaluronic acid. Regarding the time interval before initiating physical therapy after surgery, 27.6% (n = 37; 95% CI: 20.7–35.9) of the respondents reported indicating physical therapy 8–14 days after surgery. The answers varied greatly with no clear differences between them (Fig 5).
Time to initiate physical therapy following anterior cruciate ligament reconstruction (n = 134).
Discussion
This cross-sectional study identifies trends in ACL surgery in Peru and offers an initial exploratory overview of local surgical preferences. A total of 134 valid responses were collected. The majority of respondents were male (93.3%), and 47% were under 40 years of age, and over half (53%) worked in the private sector. Regarding experience, 50% had over 10 years of practice as orthopedic surgeons. In terms of surgical techniques, 62.7% preferred drilling the femoral tunnel using the anteromedial portal. The most common graft choice was autograft (85.1%), with the hamstring tendon being the most used (83.6%). Responses about tourniquet use were varied: 34% never used it, and 28.4% always did. Finally, 27.6% recommended starting physical therapy 8–14 days after surgery.
It is important to highlight that more half of the participants had more than 10 years of knee surgery expertise. Arthroscopic ACLR requires expertise and constant training. A lengthy learning curve with years of correctly practicing this procedure provides orthopedic surgeons sufficient experience to establish which technique and factors produce the most positive postoperative results [26,27]. In this survey 67 of the 134 responding surgeons had been orthopedic surgeons for more than 10 years, and among these surgeons, 35 had more than 10 years of experience with this particular procedure. One of the key steps in performing ACLR is the accuracy and precision of tibial and femoral tunnel placement, which may take more than 64 cases to achieve an adequate learning curve [28].
In the 1980s the gold standard procedure for tunnel placement during ACLR was transtibial (TT) drilling for making the tibial and femoral tunnel [16,29]. However, TT drilling was correlated with a rotational instability because the femoral tunnel position depends on the tibial tunnel orientation, creating a non-anatomic reconstruction of the ACL in some cases [16,29]. Studies have shown that the AM portal enables more anatomic femoral tunnel placement, improving rotational stability in many cases [16]. On comparing the TT vs. the AM technique, the latter showed to be significantly better with the IKDC subjective score, the Lachman test, and the pivot-shift sign [30,31]. Six out of ten members of the SPOT, who participated in this survey, preferred the AM technique. Nevertheless, one out of ten of the respondents still used the TT technique. The persistence of TT technique use among a subset of respondents may reflect variations in training, access to updated resources, or surgeon familiarity. Our study did not explore these factors in detail, highlighting a need for further research.
One of the most discussed choices in ACLR is the graft type. In our study, 83.6% of surgeons reported using hamstring tendon autografts, a higher proportion than that reported in similar international surveys [22]. This preference may reflect both surgeon familiarity and perceptions of reduced donor site morbidity [32]. Although bone–patellar tendon–bone grafts are associated with higher rates of anterior knee pain and extension loss [33], our study did not collect clinical outcome data to assess whether such complications influenced graft selection. Further local research could clarify the factors guiding these decisions.
One potentially unexpected finding was that 34% of respondents reported never using a tourniquet during ACL reconstruction. Intraoperative knee visualization, surgery time and postoperative pain could be some of the factors why an orthopedic surgeon chooses to use a tourniquet. In the present survey, 66% of the respondents always or sometimes used a tourniquet. Nevertheless, in a previous meta-analysis there were no significant differences between the use or not of a tourniquet for the intraoperative joint visualization [34]. Regarding the surgical time, Nakayama et al. reported no statistical difference in ACLR with or without the use of a torniquet [35]. Furthermore, immediate post-operative symptoms of pain were significantly higher at 4h and 10h following torniquet use according to the visual analog scale [36]. Further studies are needed to establish a strong recommendation of the intraoperative use of this flow restriction device.
Regarding the intraarticular compounds used after an ACLR, more than 65% of the participants perform this procedure without the use of any of the above-mentioned compounds. The use of these medications is to reduce postoperative pain, postoperative hemarthrosis or the range of motion [37]. It has been reported that the administration of an intra-articular corticosteroid after a traumatic event decreases the biomarkers of chondral degeneration with no increase in the risk of infection [38,39]. Nevertheless, the cytotoxic effects of corticosteroid administration is the principal concern for this therapy and should be widely evaluated before its use [40]. Eight of the respondents reported using tranexamic acid. A recent meta-analysis showed that in comparison to intraarticular administration of tranexamic acid only intravenous administration significantly reduced hemarthrosis and pain scores without increasing thromboembolic events [37]. The same number of participants reported using platelet-rich plasma (6%). According to these respondents, platelet-rich plasma was used to help the maturation of the graft in the bone. However, a systematic review showed that while the results were promising, a recommendation for its use could not yet be made [41]. Regarding the use of hyaluronic acid and bupivacaine for reducing postoperative pain, the use of the first showed a significant reduction during the first two weeks in comparison with a control group [42]. On the other hand, a meta-analysis reported that intra-articular administration of bupivacaine did not show a significant reduction in postoperative pain [43]. Nevertheless, bupivacaine in combination with morphine was found to reduce pain up to 12 hours after surgery with significantly lower postoperative opioid use [43]. Further studies comparing all these compounds are needed in order to make recommendations.
Currently, there is no strict recommendation on the type or time of initiation of physiotherapy [44]. However, postoperative physiotherapy is essential for patient recovery following ACLR and important for returning to sports activities [45]. Our results show that there is no concrete postoperative protocol, but eight out of ten of the surgeons interviewed prefer to start in the first three weeks after reconstruction, according to the current general recommendation of an early rehabilitation program [44].
This study presents the first comprehensive analysis of ACL reconstruction practices in Peru, revealing distinct patterns that differ from commonly reported practices in North American and European literature [46]. Notable findings include Peruvian surgeons’ preference for delayed surgical timing (14–20 days or beyond 28 days post-injury) rather than early intervention, and a strong predilection for hamstring autografts (83.6%) with a complete absence of quadriceps tendon usage, despite its growing international popularity [47]. These insights are particularly valuable as they highlight how surgical practices in a developing country may differ from more extensively studied regions, potentially reflecting variations in resource availability, training patterns, and clinical decision-making [46]. This baseline data about regional surgical preferences could help inform the development of more globally representative surgical guidelines and identify opportunities for educational interventions regarding newer techniques in ACL reconstruction.
The research results have potential applications which extend past academic purposes. National training programs and residency curricula should use this information to prioritize the techniques which surgeons most frequently use in Peru. The findings about graft selection and rehabilitation methods will help create standardized clinical guidelines which match the Peruvian healthcare environment. Future policy initiatives should concentrate on enhancing access to advanced graft solutions and unproven technologies that have not spread throughout our region.
While the results offer a snapshot of current practices, they also underscore the need for further research to standardize treatment protocols in ACLR. The variability in surgical timing, graft choices, and post-operative care (such as the use of compounds and physical therapy initiation) highlights areas where more evidence-based guidelines could be developed. Additionally, the differences in tourniquet use and the low rate of armed forces involvement suggest that broader studies may be needed to assess how these factors impact long-term outcomes. Future research should explore the benefits and disadvantages of different surgical approaches and graft sites, the role of post-operative treatments, and optimal rehabilitation timelines, to enhance the consistency and effectiveness of ACLR procedures across diverse clinical settings.
The main limitation of this study is the potential for selection bias. Although we attempted to reach all orthopedic surgeons performing ACL reconstruction within SPOT, the response rate was not high enough to be considered fully representative. This limited number of responses may affect the generalizability of the findings, as non-respondents could have different surgical practices or preferences compared to respondents. Although the survey did not cover the majority of SPOT members, there is a higher likelihood of finding specialists on this topic within this society at the Peruvian level. The results cannot be extrapolated to other countries because of the population type and accessibility of resources. For that reason, a comparison of all the points of the survey cannot be objectively made. This was an exploratory study and therefore our main interest was to identify ACLR preferences among a sample of Peruvian orthopedic surgeons. Consequently, no conclusions or suggestions for the most advantageous therapy can be inferred. Nevertheless, it should be noted that the ACL knee surgeons in Peru have the same trends as the other 57 countries reviewed [22]. Future studies could evaluate differences in preferences based on demographic and contextual factors, using diverse study designs to provide a more comprehensive understanding.
To our knowledge, this is the first national survey of ACLR practices in Peru, providing a valuable baseline on surgical preferences in the region. Notable findings include the high preference for hamstring autografts, frequent use of the anteromedial portal technique, and variability in the timing of physical therapy initiation, with most surgeons starting within the first three weeks. These trends contrast with some practices reported in high-income countries and may reflect contextual factors such as training, resource availability, and institutional protocols. Future research should investigate how these surgical preferences impact clinical outcomes, rehabilitation effectiveness, and long-term joint stability in the Peruvian population. Additionally, further studies could help inform the development of national guidelines and consensus statements tailored to regional needs.
Supporting information
S1 FileSurvey.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Domnick C, Raschke MJ, Herbort M. Biomechanics of the anterior cruciate ligament: physiology, rupture and reconstruction techniques. World J Orthop. 2016;7(2):82–93. doi: 10.5312/wjo.v 7.i 2.82 26925379 PMC 4757662 · doi ↗ · pubmed ↗
- 2Kaeding CC, Léger-St-Jean B, Magnussen RA. Epidemiology and diagnosis of anterior cruciate ligament injuries. Clin Sports Med. 2017;36(1):1–8. doi: 10.1016/j.csm.2016.08.001 27871652 · doi ↗ · pubmed ↗
- 3Leathers MP, Merz A, Wong J, Scott T, Wang JC, Hame SL. Trends and demographics in anterior cruciate ligament reconstruction in the United States. J Knee Surg. 2015;28(5):390–4. doi: 10.1055/s-0035-1544193 25635874 · doi ↗ · pubmed ↗
- 4Mall NA, Chalmers PN, Moric M, Tanaka MJ, Cole BJ, Bach Jr BR. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42:2363–70.25086064 10.1177/0363546514542796 · doi ↗ · pubmed ↗
- 5Kiapour AM, Murray MM. Basic science of anterior cruciate ligament injury and repair. Bone Joint Res. 2014;3(2):20–31. doi: 10.1302/2046-3758.32.2000241 24497504 PMC 3922117 · doi ↗ · pubmed ↗
- 6Kaeding CC, Aros B, Pedroza A, Pifel E, Amendola A, Andrish JT, et al. Allograft versus autograft anterior cruciate ligament reconstruction: predictors of failure from a MOON prospective longitudinal cohort. Sports Health. 2011;3(1):73–81. doi: 10.1177/1941738110386185 23015994 PMC 3445196 · doi ↗ · pubmed ↗
- 7Maletis GB, Inacio MCS, Funahashi TT. Risk factors associated with revision and contralateral anterior cruciate ligament reconstructions in the Kaiser Permanente ACLR registry. Am J Sports Med. 2015;43(3):641–7. doi: 10.1177/0363546514561745 25548148 · doi ↗ · pubmed ↗
- 8Wang H-D, Gao S-J, Zhang Y-Z. Hamstring autograft versus hybrid graft for anterior cruciate ligament reconstruction: a systematic review. Am J Sports Med. 2020;48(4):1014–22. doi: 10.1177/0363546519849483 31166113 · doi ↗ · pubmed ↗