Interval colorectal cancer: Lesson from looking back
Giovanni Aldinio, Helmut Neumann, Luigi Boni, Emanuele Dabizzi, Luca Elli, Marco Maggioni, Gian Eugenio Tontini

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1 Fig. 2
Fig. 2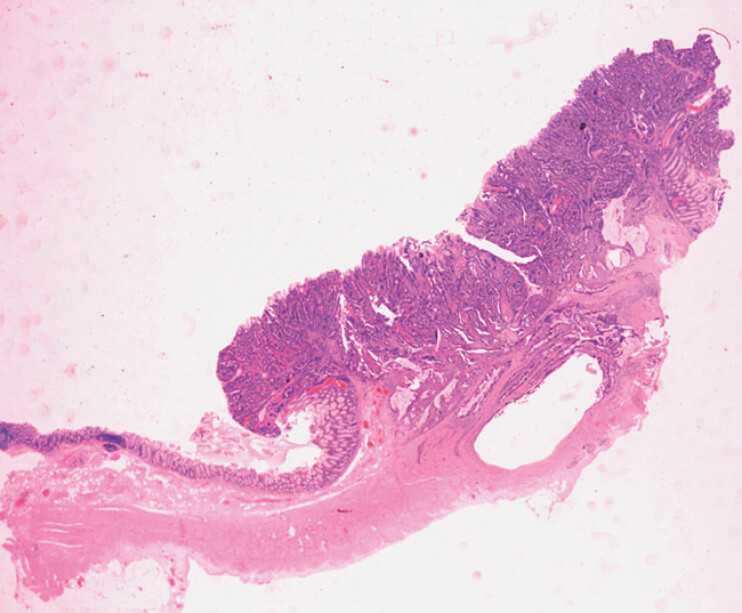 Fig. 3
Fig. 3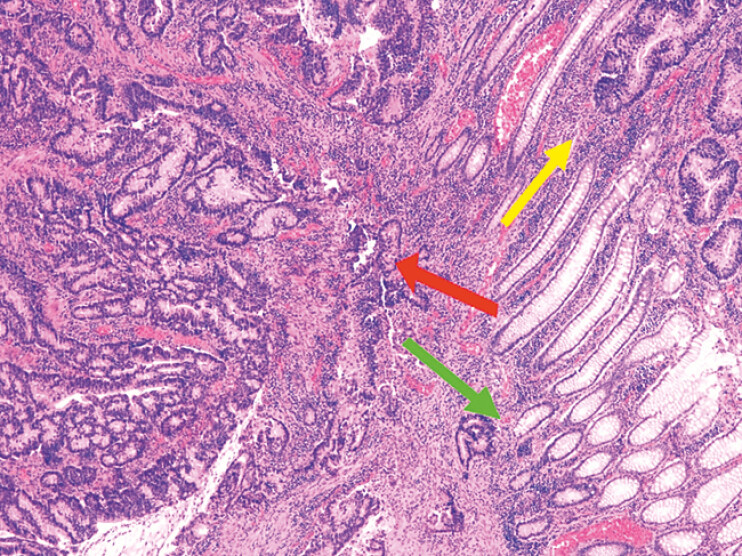 Fig. 4
Fig. 4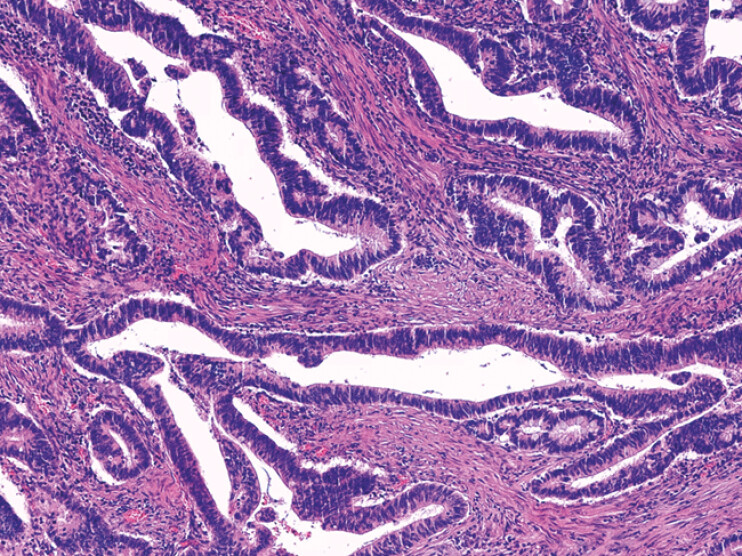 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Screening and Detection · Genetic factors in colorectal cancer · Gastric Cancer Management and Outcomes
Interval colorectal cancer (CRC), defined as cancer diagnosed after a negative colonoscopy but before the next recommended screening, accounts for approximately 2.8% to 4.9% of all CRCs and is predominantly located in the right colon 1 . Despite advancements in endoscopic techniques, its prevalence underscores the need for improved detection methods to reduce missed lesions.
Several strategies have been proposed to enhance adenoma detection rate (ADR), including techniques and devices for enhanced mucosal exposure, advanced imaging technologies 2 , water-aided colonoscopy, and computer-aided detection 3 4 . Retroflexion in the right colon is another technique that has gained attention as a method to improve visualization, particularly for lesions located behind folds or in difficult-to-reach areas. Numerous studies have shown that retroflexion can increase right-sided colonic ADR by 6% 5 . However, the procedure carries certain risks, including mucosal injury or perforation (0.03%) 5 , and requires relative operator expertise.
We report the case of an 83-year-old woman on a direct oral anticoagulant (DOAC) for atrial fibrillation who presented with anemia and a positive fecal occult blood test. High-definition colonoscopy 3 (Pentax Ec38-i10L, EPK-i7010) with a second and a third forward look of the right colon identified no lesion. Right colon retroflexion was performed, revealing a 20 × 15-mm non-pedunculated lesion (Paris 0-IIa) with advanced adenomatous features (Kudo V N ) ( Video 1 ). Endoscopic biopsies confirmed presence of adenocarcinoma and the patient underwent right hemicolectomy (TNM: pT2, G1, N0) ( Fig. 1 , Fig. 2 , Fig. 3 , Fig. 4 , Fig. 5 ).
This video-documented case shows how retroflexion in the right colon revealed a missed colorectal cancer, highlighting its potential role in improving lesion detection.Video 1
Macroscopic presentation of the right hemicolectomy surgical specimen.
Close-up of the cancerous lesion (in the circle) in the ascending colon, located on the antimesocolic side.
Histological overview of large bowel wall including the adenocarcinoma; hematoxylin and eosin (H&E) stain at 5x magnification.
Histological border of the cancerous lesion including normal crypts in the lower right (green arrow), dysplasia at the top right (yellow arrow), and invasive adenocarcinoma on the left (red arrow); H&E stain at 40x magnification.
Histology of the adenocarcinoma; H&E stain at 200x magnification.
This case provides video-documentation of a CRC diagnosis achieved through retroflexion, hereby highlighting its potential role, especially in patients with a high probability of advanced neoplasia 1 . Second, the anatomical documentation makes clear the antimesocolic region of the hepatic flexure as a challenging location for endoscopic inspection, despite standard endoscopic maneuvers to enhance blind spots. Finally, the report adds to the growing literature on endoscopic techniques to improve ADR and minimize risk of missed advanced colorectal lesions: retroflexion could be performed by operators who feel confident in its execution, with adequate instruments and in anatomical conditions that provide sufficient space for safe maneuvering.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh S Singh PP Murad MH Prevalence, risk factors, and outcomes of interval colorectal cancers: a systematic review and meta-analysis Am J Gastroenterol 20141091375138910.1038/ajg.2014.17124957158 · doi ↗ · pubmed ↗
- 2Ishaq S Siau K Harrison E Technological advances for improving adenoma detection rates: The changing face of colonoscopy Digest Liver Dis 20174972172710.1016/j.dld.2017.03.03028454854 · doi ↗ · pubmed ↗
- 3Kaminski MF Thomas-Gibson S Bugajski M Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative Endoscopy 20174937839710.1055/s-0043-10341128268235 · doi ↗ · pubmed ↗
- 4Bisschops R East JE Hassan C Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2019 Endoscopy 2019511155117910.1055/a-1031-765731711241 · doi ↗ · pubmed ↗
- 5Desai M Bilal M Hamade N Increasing adenoma detection rates in the right side of the colon comparing retroflexion with a second forward view: a systematic review Gastrointest Endosc 20198945345900030222971 10.1016/j.gie.2018.09.006 · doi ↗ · pubmed ↗