Targeted Therapy in HER2 Exon 20-Mutant Non-small Cell Lung Cancer With Leptomeningeal Disease: A Case-Based Approach to Treatment Decision-Making
Osama Elzaafarany

TL;DR
This paper presents a rare case of brain cancer caused by a specific lung cancer mutation and discusses treatment options using targeted therapy.
Contribution
The paper highlights the use of trastuzumab deruxtecan in treating HER2-mutant NSCLC with leptomeningeal disease, where no standard guidelines exist.
Findings
Trastuzumab deruxtecan was used based on evidence from other cancers with CNS involvement.
The case emphasizes the need for clinical trials addressing CNS complications in HER2-mutant NSCLC.
Precision oncology was applied in the absence of approved therapies for this rare condition.
Abstract
A rare and clinically challenging case of leptomeningeal disease (LMD) secondary to HER2-mutated non-small cell lung cancer (NSCLC), marked by both exon 20 insertion and gene amplification, is presented. In the absence of LMD-specific therapeutic guidelines for HER2-driven NSCLC, treatment was initiated with trastuzumab deruxtecan (Enhertu), based on extrapolated evidence from clinical trials in systemic NSCLC and HER2-positive breast cancer with central nervous system involvement. The patient, a 69-year-old woman with good performance status, developed LMD following prior systemic therapy and local CNS treatments. MRI and CSF cytology confirmed the diagnosis. Given the lack of approved therapies for HER2-mutant NSCLC with LMD, the treatment strategy was informed by available clinical data and supporting literature on the CNS activity of Enhertu. Other options such as poziotinib and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
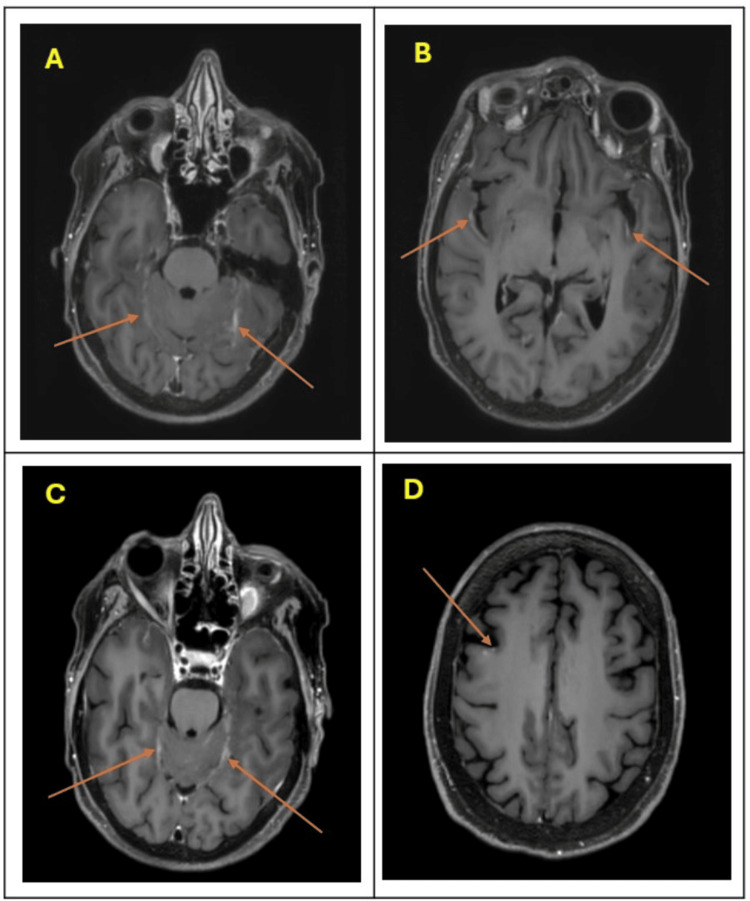 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer Genomics and Diagnostics · Lung Cancer Research Studies
Introduction
Leptomeningeal disease (LMD) in non-small cell lung cancer (NSCLC) represents a rare and therapeutically challenging complication, particularly when associated with uncommon oncogenic drivers. LMD is observed in approximately 3-9% of NSCLC cases, underscoring its rarity and complexity. Without any therapy, the prognosis for LMD is generally poor, with median survival often measured in weeks. However, medical interventions such as whole-brain radiotherapy (WBRT) and chemotherapy can offer some improvement in survival and quality of life, though their efficacy varies. WBRT may provide symptomatic relief, while chemotherapy's effectiveness is often limited by the blood-brain barrier [1].
Human epidermal growth factor receptor 2 (HER2) alterations, including exon 20 insertions and gene amplification, are detected in a small subset of NSCLC patients, with mutations found in approximately 2-4% and amplification occurring in about 2-5% of cases. The coexistence of both mutations in the context of LMD is exceedingly rare. Treatment guidelines in this molecular and anatomic setting are lacking, especially as clinical trials frequently exclude patients with LMD. Conducting a molecular study of LMD itself could refine therapy by identifying specific targets for treatment, potentially improving outcomes [1].
This case exemplifies the therapeutic dilemma and highlights a rationale for extrapolating systemic data to guide treatment, emphasizing the need for personalized treatment strategies and the importance of expanding clinical trial eligibility to include patients with such complex presentations.
This article was previously posted to the Research Square preprint server on June 17, 2024, under the title “Targeted Therapy Decision in HER2 Exon 20-Mutant Non-small Cell Lung Cancer With Leptomeningeal Disease: A Case-Based Perspective”.
Case presentation
A 69-year-old female ex-smoker presented in early 2024 with respiratory symptoms and right cervical lymphadenopathy. CT scans revealed a right upper lobe mass with associated mediastinal lymphadenopathy and distant metastases to the brain and bone. Bronchoscopic biopsy from mediastinal lymph nodes confirmed lung adenocarcinoma, staged as T4N2M1c. Immunohistochemistry demonstrated programmed death-ligand 1 (PD-L1) expression <1%. Circulating tumor DNA analysis using the Guardant360 assay detected a HER2 exon 20 insertion mutation, along with HER2 gene amplification.
The patient was initiated on first-line systemic therapy with carboplatin, pemetrexed, and pembrolizumab, followed by maintenance pemetrexed and pembrolizumab. Stereotactic radiosurgery (SRS) was delivered to multiple brain metastases, and palliative external beam radiation therapy was administered to osseous sites of disease.
In April 2025, the patient developed worsening headaches. Brain MRI revealed multifocal leptomeningeal enhancement with stable parenchymal metastases. Lumbar puncture confirmed leptomeningeal metastases (LMD) via positive cerebrospinal fluid (CSF) cytology. Despite this diagnosis, she remained neurologically intact, with non-focal examination findings and no requirement for corticosteroids or antiepileptic medications.
The case was referred to our institution in May 2025. Repeat lumbar puncture again demonstrated atypical cells in the CSF, with normal glucose and protein levels. MRI findings were consistent with diffuse leptomeningeal involvement (Figure 1). The only presenting neurologic symptom was a persistent headache. Given her preserved performance status, the patient was treated with whole neuraxis proton radiotherapy.
Axial contrast-enhanced brain MRI demonstrating leptomeningeal disease (LMD).Axial post-contrast T1-weighted MRI of the brain (labeled A–D) demonstrating abnormal enhancing lesions (arrows) concerning for leptomeningeal disease (LMD).(A) and (C): Enhancement along the bilateral cerebellar folia and posterior fossa leptomeninges.(B): Leptomeningeal enhancement involving the bilateral temporal lobes.(D): Focal gyral enhancement over the high convexity region, suggestive of cortical involvement.These imaging findings are characteristic of LMD, often seen in advanced metastatic disease.
In the absence of standard-of-care therapies for HER2-mutant NSCLC with LMD, and the limited efficacy of currently available tyrosine kinase inhibitors in this molecular subtype, the decision was made to initiate systemic therapy with trastuzumab deruxtecan (Enhertu), a HER2-directed antibody-drug conjugate. At the time of this report, follow-up data following treatment initiation are not yet available.
Discussion
The use of trastuzumab deruxtecan in this case was informed by several lines of evidence. The DESTINY-Lung02 trial demonstrated the efficacy of this agent in HER2 exon 20-mutant NSCLC, though it excluded patients with LMD [2]. Its CNS activity is better characterized in HER2-positive breast cancer, where studies such as the DEBBRAH trial and ROSET-BM have reported responses in patients with brain metastases and LMD [3,4]. Additional retrospective studies have supported its ability to cross the blood-brain barrier and generate meaningful responses in LMD from breast cancer [5].
Alternative options were considered, including Poziotinib, a pan-HER tyrosine kinase inhibitor. This drug demonstrated clinical benefits in a phase 2 study involving 50 patients with EGFR exon 20 mutant advanced NSCLC [6]. Additionally, a case report by Fan et al. described a clinical response to Poziotinib in a patient with HER2 exon 20-mutated NSCLC with LMD [7]. However, the current evidence is insufficient to support its use specifically for LMD. There are also concerns regarding the risk-benefit ratio and toxicity observed in clinical trials, highlighting the need for further data from randomized controlled studies.
Zongertinib, an emerging irreversible HER2-selective tyrosine kinase inhibitor, has shown promising results in a phase 1 study for previously treated HER2-mutant NSCLC. However, its efficacy in the subset of patients with LMD is lacking [8]. Nevertheless, Zongertinib may be the preferred second-line option when trastuzumab deruxtecan (Enhertu) is contraindicated or not tolerated, particularly in patients experiencing severe fatigue or poor performance status in the setting of whole neuraxis radiotherapy, which is a common practice in managing LMD.
Intrathecal trastuzumab was not pursued, as HER2 exon 20 insertions typically affect the intracellular domain, limiting the utility of extracellular monoclonal antibodies [9,10].
This case underscores the challenge of treating LMD in molecularly defined NSCLC subsets. Given the rarity of HER2 exon 20 insertions with concurrent amplification and LMD, therapeutic decisions must often rely on extrapolated evidence from related disease settings.
Conclusions
This case highlights a rare molecular and anatomic scenario: HER2 exon 20-mutated and amplified NSCLC with LMD. In the absence of guideline-recommended therapies, we utilized trastuzumab deruxtecan based on extrapolated data from NSCLC and breast cancer trials. This case emphasizes the importance of expanding clinical trial eligibility to include patients with LMD, as well as the need for dedicated studies addressing treatment strategies in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leptomeningeal metastasis from non-small cell lung cancer and current landscape of treatments Clin Cancer Res Ozcan G Singh M Vredenburgh JJ 11292920233597243710.1158/1078-0432.CCR-22-1585 · doi ↗ · pubmed ↗
- 2Trastuzumab deruxtecan in patients with HER 2-mutant metastatic non-small-cell lung cancer: primary results from the randomized, phase II DESTINY-Lung 02 trial J Clin Oncol Goto K Goto Y Kubo T 485248634120233769434710.1200/JCO.23.01361 PMC 10617843 · doi ↗ · pubmed ↗
- 3Trastuzumab deruxtecan in patients with central nervous system involvement from HER 2-positive breast cancer: the DEBBRAH trial Neuro Oncol Pérez-García JM Vaz Batista M Cortez P 1571662520233563982510.1093/neuonc/noac 144PMC 9825345 · doi ↗ · pubmed ↗
- 4Treatment with trastuzumab deruxtecan in patients with HER 2-positive breast cancer and brain metastases and/or leptomeningeal disease (ROSET-BM)NPJ Breast Cancer Niikura N Yamanaka T Nomura H 82920233782151410.1038/s 41523-023-00584-5PMC 10567705 · doi ↗ · pubmed ↗
- 5Durable responses to trastuzumab deruxtecan in patients with leptomeningeal metastases from breast cancer with variable HER 2 expression J Neurooncol Rogawski D Cao T Ma Q Roy-O'Reilly M Yao L Xu N Nagpal S 20921717020243907368710.1007/s 11060-024-04788-y · doi ↗ · pubmed ↗
- 6Poziotinib for EGFR exon 20-mutant NSCLC: clinical efficacy, resistance mechanisms, and impact of insertion location on drug sensitivity Cancer Cell Elamin YY Robichaux JP Carter BW 7547674020223582039710.1016/j.ccell.2022.06.006PMC 9667883 · doi ↗ · pubmed ↗
- 7HER 2 exon 20 insertion mutations in lung adenocarcinoma with leptomeningeal metastasis: a case report and response to poziotinib Ann Palliat Med Fan Y Qin J Han N Lu H 158215881120223411883110.21037/apm-21-213 · doi ↗ · pubmed ↗
- 8Zongertinib in previously treated HER 2-mutant non-small-cell lung cancer N Engl J Med Heymach JV Ruiter G Ahn MJ 2321233339220254029318010.1056/NEJ Moa 2503704 · doi ↗ · pubmed ↗