Association between keloids and cardiovascular disease in Black and Asian individuals
Karishma S. Shah, Michelle S. Min

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
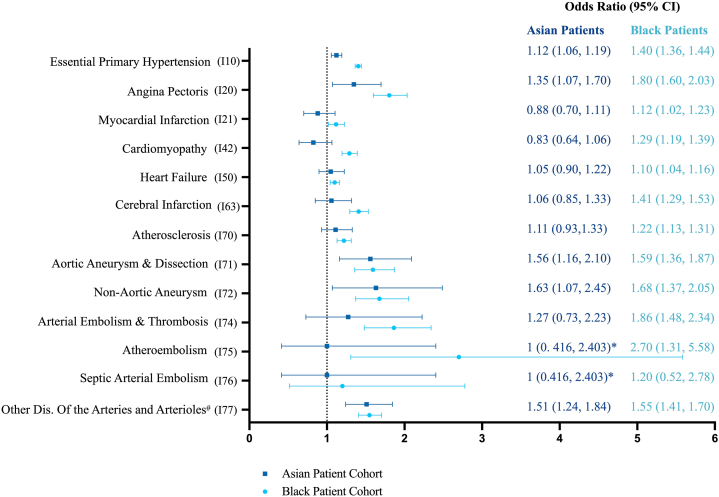 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research
To the Editor: Keloids are defined as scars that grow beyond their initial wound boundaries and are particularly prevalent among Black and Asian populations. Overactive fibroblasts lead to an increased ratio of type I collagen (COL1) to type 3 collagen (COL3) in keloids, but both are overexpressed in keloids compared to normal skin.1 Notably, COL1 and COL3 also provide structural support as part of myocardial extracellular matrices (ECM). While COL1 is found in most ECM, COL3 is also found in vasculature and hollow organs. Given collagen's role in the skin and cardiovascular system, we aimed to investigate the relationship between keloids and cardiovascular disease (CVD) in genetically at-risk populations.
Black and Asian patients, aged 18 years and up, with an International Classification of Diseases (ICD-10) code for hypertrophic scar/keloid (ICD-10, L91.0) from 2004 to 2024 were extracted from the TriNetX database, a global network comprising deidentified patient data. These cohorts were 1:1 matched by age, sex, race, ethnicity, tobacco use (Z72.0), alcohol use (F10), hyperlipidemia (E78.5), type 2 diabetes mellitus (E11), and overweight/obesity (E66) to controls without keloids. The primary outcome of interest was a CVD diagnosis, defined by 13 diseases affecting the myocardium/vasculature based on ICD codes (Table I). Analysis consisted of univariate logistic regression and chi-squared tests with P-value < .05 considered statistically significant.Table IDemographic data and differences in the presence of cardiovascular disease for Black and Asian patients with keloids and matched control patientsBlack patientsAsian patientsKeloidsControlPKeloidsControlPPatients after matching (n)43,02943,02913,42313,423Age at index (mean in years ± SD)∗41.8 ± 16.841.8 ± 16.7.7540.7 ± 16.640.7 ± 16.6.79Female (n, %)∗27,989 (65.1%)27,922 (64.9%).638743 (65.1%)8732 (65.1%).89Hispanic† (n, %)∗667 (1.6%)666 (1.6%).98121 (0.9%)125 (0.9%).80Cardiovascular risk factors∗ Hyperlipidemia (n, %)7094 (16.5%)7088 (16.5%).971806 (13.5%)1848 (13.8%).45 Type 2 diabetes mellitus (n, %)6059 (14.1%)6119 (14.2%).561178 (8.8%)1195 (8.9%).71 Alcohol ue (n, %)1215 (2.8%)1218 (2.8%).95118 (0.9%)102 (0.8%).28 Tobacco use (n, %)991 (2.3%)1059 (2.5%).1374 (0.6%)74 (0.6%)1.0 Overweight/obesity (n, %)10,278 (23.9%)10,215 (23.7%).61914 (6.8%)851 (6.3%).12CVD, ICD-10 codes Essential primary hypertension, I10 (n, %)15,928 (37.1%)12,699 (29.5%)<.0012790 (20.8%)2543 (19.0%)<.001 Angina pectoris, I20 (n, %)746 (1.7%)417 (1.0%)<.001172 (1.3%)128 (1.0%).01 Myocardial infarction, I21 (n, %)953 (2.2%)855 (2.0%).02142 (1.1%)161 (1.2%).27 Cardiomyopathy, I42 (n, %)1547 (3.6%)1210 (2.8%)<.001135 (1.0%)145 (1.0%).55 Heart failure, I50 (n, %)2917 (6.8%)2668 (6.2%)<.001337 (2.5%)322 (2.4%).55 Cerebral infarction, I63 (n, %)1318 (3.1%)944 (2.2%)<.001167 (1.5%)158 (1.4%).62 Atherosclerosis, I70 (n, %)1544 (3.6%)1275 (3.0%)<.001264 (2.0%)238 (1.8%).24 Aortic aneurysm and dissection, I71 (n, %)389 (0.9%)245 (0.6%)<.001115 (0.9%)74 (0.6%).003 Nonaortic aneurysm, I72 (n, %)251 (0.6%)150 (0.4%)<.00157 (0.4%)35 (0.3%).022 Arterial embolism and thrombosis, I74 (n, %)210 (0.5%)113 (0.3%)<.00128 (0.2%)22 (0.2%).40 Atheroembolism, I75 (n, %)27 (0.1%)10 (0.02%).005210 (0.07%)10 (0.07%)1.00 Septic arterial embolism, I76 (n, %)12 (0.03%)10 (0.02%).6710 (0.07%)10 (0.07%)1.00 Other arterial disease, I77 (n, %)1090 (2.5%)710 (1.7%)<.001248 (1.9%)165 (1.2%)<.001CVD, Cardiovascular disease; ICD-10, International Classification of Disease; SD, standard deviation.∗Cohorts were 1:1 propensity score matched based upon these variables.†Individuals who identified themselves as racially Black or Asian and ethnically Hispanic or Latino.
A total of 56,452 patients were included in our analysis (Table I). A majority of CVD diagnoses were significantly associated with keloids in Black patients (Fig 1). Atheroembolism had the highest significant odds ratio in Black patients with an odds ratio (OR) of 2.70 (95% confidence interval [CI]: 1.31-5.58). In Asian patients, non-aortic aneurysm had the highest significant odds ratio (OR: 1.63 (1.07-2.45). The most significant myocardial disease was angina pectoris in both Black (OR: 1.80, CI: 1.60-2.03) and Asian (OR: 1.35, CI: 1.07-1.70) patients.Fig 1. Keloids and cardiovascular disease. Odds ratios for various cardiovascular conditions in the setting of keloids in Black and Asian patients. ∗Denotes that there were <10 outcomes for analysis. #Dis. serves as an abbreviation for diseases.
Our study expands on emerging data suggesting that keloids are not an isolated dermatologic condition. Joint pain, uterine leiomyomas, and irritable bowel syndrome have been associated with keloids.2 Several independent studies have also linked hypertension with keloids,3 corroborating our findings. We now add other CVDs as potential associations. These findings suggest that aberrant collagen synthesis seen in keloids might not be limited to the dermis. Prior research has confirmed that disruption and subsequent accumulation of COL1/3 in the myocardial ECM play a crucial role in heart remodeling and the development of many CVDs, eventually resulting in heart failure.4 Additionally, COL3 influences vascular tensile strength and facilitates platelet adhesion.5 It is possible that hyperactive fibroblasts compromise vascular integrity and promote hypercoagulability. Interestingly, data suggest that statins have antifibrotic properties; thereby, statins could address both CVD and keloids,6 but future studies are warranted.
Study limitations include retrospective design and lack of differentiation between hypertrophic scars and keloids based on ICD code. Additionally, several confounders, such as major cardiovascular surgeries, could not be explored within this database.
Overall, awareness of the heightened risk of CVD in patients with keloids can lead to better understanding, counseling, and screening.
Conflicts of interest
MSM is on the advisory boards of BMS and Horizon. She is an investigator for Amgen, BMS, BI, and Priovant.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jumper N.Paus R.Bayat A.Functional histopathology of keloid disease Histol Histopathol 30920151033105710.14670/HH-11-62425900252 · doi ↗ · pubmed ↗
- 2Ung C.Y.Warwick A.Onoufriadis A.Comorbidities of keloid and hypertrophic scars among participants in UK Biobank JAMA Dermatol 1592202317218110.1001/jamadermatol.2022.560736598763 PMC 9857738 · doi ↗ · pubmed ↗
- 3Arima J.Huang C.Rosner B.Akaishi S.Ogawa R.Hypertension: a systemic key to understanding local keloid severity Wound Repair Regen 232201521322110.1111/wrr.122725728259 · doi ↗ · pubmed ↗
- 4Nikolov A.Popovski N.Extracellular matrix in heart disease: focus on circulating collagen type I and III derived peptides as biomarkers of myocardial fibrosis and their potential in the prognosis of heart failure: a concise review Metabolites 124202229710.3390/metabo 1204029735448484 PMC 9025448 · doi ↗ · pubmed ↗
- 5Kuivaniemi H.Tromp G.Type III collagen (COL 3A 1): gene and protein structure, tissue distribution, and associated diseases Gene 707201915117110.1016/j.gene.2019.05.00331075413 PMC 6579750 · doi ↗ · pubmed ↗
- 6Chello C.Nenna A.Chello M.Statin treatment and hypertrophic scarring after cardiac surgery Wound Repair Regen 291202112913310.1111/wrr.1287833236817 · doi ↗ · pubmed ↗