Ozonated water to treat pericoronitis - insights from a randomized triple-blind pilot trial
Célio Leone Ferreira Soares, Dhelfeson Willya Douglas-de-Oliveira, Cássio Roberto Rocha dos Santos, Olga Dumont Flecha, José Cristiano Ramos Glória, Patricia Furtado Gonçalves

TL;DR
This study compares ozonated water and saline solution for treating pericoronitis, finding both similarly effective in reducing pain and inflammation.
Contribution
The study introduces ozonated water as a potential alternative to saline for pericoronitis treatment.
Findings
Both ozonated water and saline significantly reduced pain and edema/erythema within 7 days.
OHIP-14 scores showed improved quality of life at 30 days in both treatment groups.
Ozonated water was found to be as effective as saline in managing pericoronitis.
Abstract
Pericoronitis, a painful inflammation of the soft tissues around a partially erupted tooth, is generally treated with debridement and saline irrigation. Ozone’s antimicrobial and anti-inflammatory properties make it a promising adjunctive therapy. To evaluate the clinical effects and impact on quality of life of treating pericoronitis in lower third molars using ozonated water compared to physiological saline solution. This study involved patients with pericoronitis in lower third molars, following CONSORT guidelines. Ethical approval was obtained from the UFVJM Research Ethics Committee (protocol number 5.922.185). Patients were divided into two groups: irrigation with ozonated water (OZO, n = 5) or saline solution (SAL, n = 5). The pain was assessed using a visual analog scale, and quality of life was evaluated using OHIP-14, OHIP14-PD Br, and SF-36 questionnaires. Evaluations were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
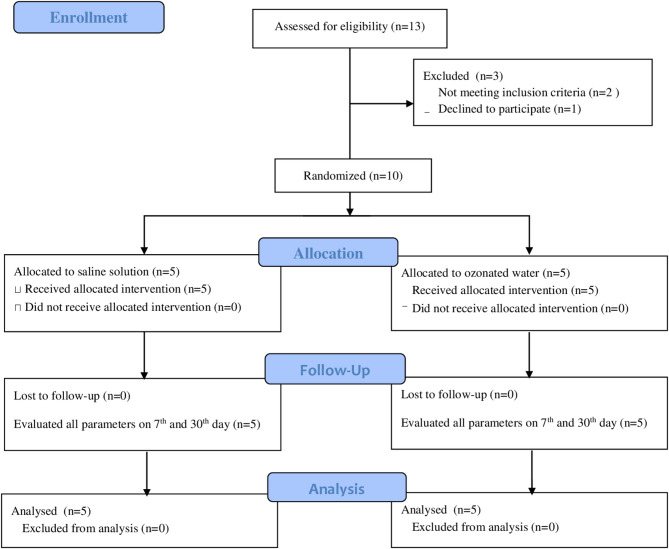 Figure 1
Figure 1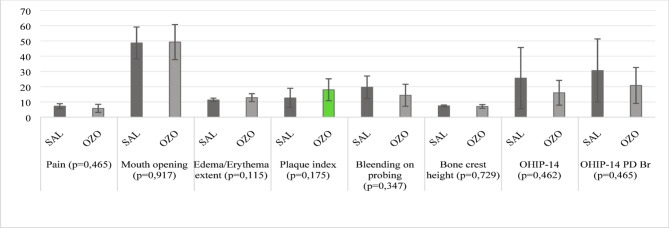 Figure 2
Figure 2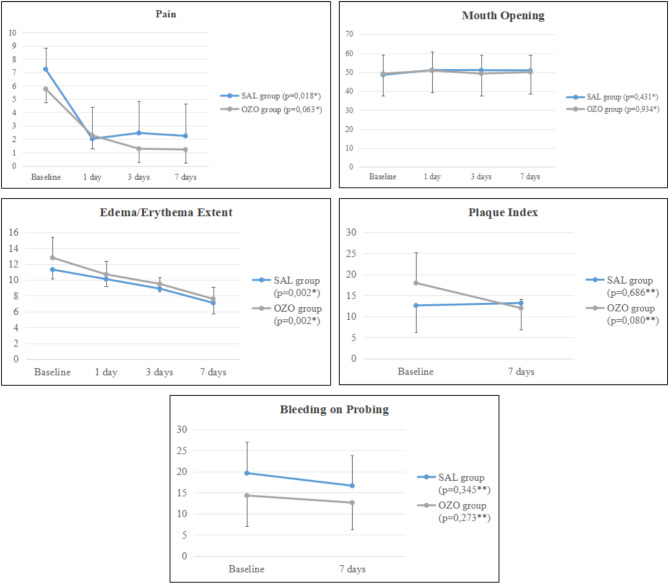 Figure 3
Figure 3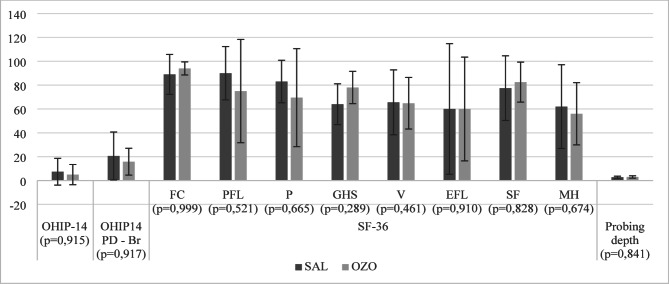 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical and Biological Ozone Research · Laser Applications in Dentistry and Medicine · Dental Anxiety and Anesthesia Techniques
Introduction
Pericoronitis is a painful inflammatory condition commonly associated with erupting lower third molars in young adults, characterized by a complex anaerobic microbial flora [1–3]. Symptoms include pain and swelling in the pseudopocket around the tooth crown. Acute pericoronitis is treated as a dental emergency with local debridement and saline irrigation, sometimes supplemented with antibiotics and analgesics [4–6].
As a consequence of pain, oral health problems have been increasingly recognized as having a negative impact on patient’s quality of life and daily performance. There is also a need to investigate the impact on the quality of life of treated cases of pericoronitis through new clinical trials [7, 8]. Some products with anti-inflammatory and antimicrobial properties, in addition to debridement and local irrigation with saline solution, have been investigated as adjuvants in the treatment of pericoronitis. Among them, ozone, a natural compound with antimicrobial, anti-inflammatory, antifungal, immunomodulatory, and even analgesic effects against microorganisms, has been studied [9–11].
Studies have confirmed the efficacy of ozone in killing gram-negative and gram-positive microorganisms in ozonated water [12], as well as inhibiting the accumulation of experimental biofilm in vitro and being effective against bacteria in dental biofilm. It also reduces post-surgical infectious complications when used as an irrigation agent during the extraction of third molars [13].
This study investigates whether irrigation with ozonated water, compared to saline solution, improves the quality of life and clinical parameters in patients with pericoronitis. Given ozone’s antimicrobial and anti-inflammatory properties, we hypothesize that ozonated water will yield superior results in reducing symptoms and enhancing patient quality of life.
Materials and methods
Study design
This pilot randomized triple-blind clinical trial included two groups of five patients each, with a 30-day follow-up period. The study was approved by the Research Ethics Committee (protocol #5.922.185) of the Federal University of Jequitinhonha and Mucuri Valleys (UFVJM) and was conducted following CONSORT and according to the Helsinki Declaration. This clinical trial was registered at the Brazilian Clinical Trials Registry (http://www.ensaiosclinicos.gov.br/rg/RBR-79pss6w/) on 22/11/2024.
Participants
Patients with symptomatic pericoronitis were recruited at the UFVJM Surgery and Periodontics Clinic from November 2024 to December 2024. Inclusion criteria were patients aged 18 years or older with periodontal health or periodontal status level I and II [14], presenting with spontaneous pain around the lower third molar. Exclusion criteria included recent antibiotic therapy, medical contraindications for periodontal probing, patients with systemic illnesses, or contraindications for analgesics. All participants received written informed consent and were included only after agreeing and signing it.
Settings
This study was carried out at the Surgery and Periodontics Clinic of the UFVJM. A researcher (CLFS) was responsible for carrying out all evaluations, properly calibrated and trained with panoramic radiographs to assess the position of the third molar, and the evaluation of other clinical parameters, including the use of the Florida Probe, through test-retest with a 15-day interval. The intraclass correlation coefficient was kappa of 0.9. Each patient was evaluated in six appointments: baseline, 24 h, 3, 7, 15, and 30 days after the interventions. Another researcher (PFG) was responsible for performing the treatments and providing guidance to the patients.
Randomization and blinding
This triple-blind trial used identical packaging for the liquids, which were transparent, odorless, and tasteless. An independent researcher conducted the randomization and sealed the intervention assignments in opaque envelopes. Patients and researchers remained blinded to the interventions.
One researcher received a standardized, unlabeled irrigation syringe during the procedure. Patients could not distinguish the product, as neither had taste, odor, or color. The evaluator was blinded to the treatment type, which was only revealed after the final statistical analysis.
Interventions
Patients were treated with debridement under a pericironal hood using curettes and under local anesthesia with 2% lidocaine hydrochloride with 1:100,000 epinephrine (Lidocaine 2% DFL ^®^). The test group received ozonated water irrigation, and the control group received saline solution irrigation, both with a standard volume of 20 mL. Both groups received oral hygiene instructions and a standardized oral hygiene kit.
The ozonated water was produced chairside from MilliQ water, using an ozone generator model MedPlus V (Philozon^®^, Santa Catarina, Brazil), coupled with a glass column with a catalyst and microbubble diffuser in a stainless steel tube. The ozone generator was set to 60 µg/mL for five continuous minutes of bubbling in 250 mL of MilliQ water.
Evaluated parameters
The study assessed multiple parameters using specific instruments at various time points. The primary outcomes are pain and quality of life, while the secondary outcomes include other clinical parameters. Pain was measured with the Visual Analog Scale (VAS) [15] and mouth opening with a millimeter ruler [16] at baseline and at 1, 3, 7, 15, and 30 days post-treatment. Edema and erythema were evaluated using dental floss and a millimeter rule [16] at the same intervals. Quality of life was assessed with Oral Health Impact Profile-14 [17], Oral Health Impact Profile-14 Periodontal Disease-Br [18], and Short Form-36 [19] at baseline and 30 days. Plaque index [20], bleeding on probing (WHO probe) [21], and probing depth (Florida probe) [22] were measured at baseline, 7, 15, and 30 days. Bone crest height (Williams Probe) [22] was recorded at baseline and 30 days, while the third molar position was assessed via panoramic radiography [16] at baseline.
Sample size
Sample size was calculated using the Epidemiology and Statistics Laboratory (LEE) tool (http://www.lee.dante.br/pesquisa/amostragem/calculo_amostra.html) based on the following parameters: the standard deviation obtained from pain intensity through the visual analogic scale (9.94 mm) [23]; the difference stipulated between groups, which was 5 mm; a significance level of 95%; and a power of 80%. Thus, 17 participants per group were required for the study. For the pilot study, 25% of the sample size was defined, with an additional 10% to account for potential losses, resulting in a requirement of 5 participants per group.
Statistical methods
Statistical analyses were performed using the statistical package SPSS (Statistical Package for the Social Sciences Inc.) version 26.0. A 95% confidence interval was used, and a 5% level of significance was adopted. The data normal distribution was verified through the Shapiro-Wilk test. The inter- and intra-group comparisons were conducted using the Mann-Whitney and Wilcoxon tests, respectively. For repeated measures, data were subjected to the Friedman test, with Bonferroni post-hoc analysis. Categorical data were evaluated using Fisher’s Exact test.
Results
The number of participants and the reasons for the losses are described in the Flowchart (Fig. 1). Both groups showed similarities regarding sociodemographic data (Table 1) and clinical parameters (Fig. 2). The most frequent position among the teeth included in the study, according to the Pell and Gregory classification, was 2 A (70.0%), followed by 2B (20.0%) and 1 A (10.0%).
Fig. 1. Flow chart depicting the study design
Table 1. Socio-demographic and outcome characteristicsVariable SAL group
OZO group
n
%
n
%
p Tooth0,999 38360,0360,0 48240,0240,0Gender0,490 Female480,0360,0 Male120,0240,0Alcohol0,500 No120,000,0 Yes480,05100,0Smoker0,083 No5100,0240,0 Yes00,0360,0Age25,8 (± 4,02)25,8 (± 3,06)0,999Pell and Gregory Classification 1 A120,000,00,311 2 A240,05100,0 2B240,000,0Data (tooth, gender, alcohol, smoker and Pell and Gregory Classification) were shown as absolute (n) and relative (%) frequencies. Age was shown as mean (± standard deviation)
Fig. 2. Clinical parameters of groups on baseline. The evaluated parameters are presented with the mean, standard deviation, and p-value
There was no statistical difference for the clinical parameters evaluated in the intergroup analysis 7 days after treatment (Table 2). However, in the intragroup analysis, both groups showed improvement in some parameters. The SAL group improved in the parameters of pain and edema/erythema extent (p = 0,018; p = 0,002; respectively), while the OZO group showed improvement only in the edema/erythema extent (p = 0,002), with no improvement in other parameters (Fig. 3).
Table 2. Intergroup analysis 7 days after treatment. The evaluated parameters are presented with the mean, standard deviation (SD), and p-value for both groupsVariable SAL
OZO
Mean
SD
Mean
SD
p Pain2,242,431,221,490,599Mouth opening50,808,4850,088,930,917Edema/erythema extent7,101,397,601,520,456Plaque index13,206,3412,002,100,917Bleending on probing16,667,1812,656,310,465SD: standard deviation
Fig. 3. Intragroup analysis of evaluations up to 7 days after treatment. Data (Pain, Mouth Opening, Edema/Erythema Extent, Plaque Index, Bleeding on Probing) were shown as means ± standard deviation, and p-value for both groups on baseline, 1, 3, and 7 days post-treatment. ^* Friedman Test, Boferroni post−hoc ** Wilcoxon Test^
Regarding quality of life and probing depth in the second molar adjacent to the treated tooth in the study, there was no difference in the intergroup comparison (Fig. 4). In the intragroup analysis, there was a difference for the SAL group in OHIP-14 and OHIP-14 PD Br (p = 0,043; p = 0,042, respectively) and for the OZO group in OHIP-14 and in the GHS domain of the SF-36 (p = 0,041; p = 0,034; respectively); there was no difference in any of the other SF-36 domains or other evaluated parameters (Table 3).
Fig. 4. Intergroup analysis of quality of life and probing depth of the 2nd molar, 30 days after treatment
Table 3. Intragroup analysis of alveolar bone crest height, probing depth of the 2nd molar, and quality of life, 30 days after treatmentVariable Baseline 30 days Mean
SD
Mean
SD
p SAL groupBone crest height7,400,556,400,550,059Probing depth of the 2nd molar4,000,702,800,830,063OHIP1425,6020,077,4011,220,043OHIP14 PD Br30,6020,7220,6020,060,042SF-36FC73,0027,0689,0016,730,197PFL55,0041,0890,0022,360,066P78,5022,1983,0017,800,854GHS61,0018,1764,0017,100,257RE61,6030,8065,6027,220,102EFL60,0054,7760,0054,770,999SF67,5039,1377,5027,100,257MH59,0033,8062,0035,110,461OZO groupBone crest height7,001,226,000,710,102Probing depth of the 2nd molar4,400,893,001,000,066OHIP1416,008,125,008,460,041OHIP14 PD Br20,8011,7815,8011,230,066SF-36FC91,0012,4594,005,480,593PFL75,0043,3075,0043,300,999P69,0036,7769,5041,090,999GHS71,0015,5778,0013,510,034RE56,8026,8964,8021,610,104EFL66,6633,3560,0043,470,713SF62,5031,8782,5016,770,257MH56,0030,2956,0026,080,999SD: standard deviation. The domains assessed by the SF-36 are FC = Functional capacity; PF = Physical functioning limitations; P = Pain; GHS = General health status; RE = Vitality; EF = Emotional functioning limitations; SF = Social functioning; MH = Mental health
Discussion
This study is the first to provide experimental evidence of the effects of ozonated water on clinical parameters and quality of life in patients with lower third-molar pericoronitis. Results suggest that ozonated water improves certain clinical parameters, such as pain and edema/erythema extent, as well as patient quality of life. The study aimed to investigate whether ozonated water treatment as an adjunct improves clinical outcomes and quality of life compared to saline solution treatment, hypothesizing potential patient improvement.
The study hypothesis was partially accepted, as the use of ozonated water as an adjunct to treatment improved pain, edema/erythema extent, and quality of life for patients; however, there was no influence on improving other clinical parameters. This may be related to the sample size, as being a pilot study, it was not of significant size to statistically significant differences between parameters [24, 25].
Previous studies have explored new alternatives for pericoronitis treatment, ranging from novel therapies to comparisons between different drugs. However, when assessing patient pain, none of them showed significant differences compared to the control group [23, 26–28]. Mouth opening, also assessed in some studies as another manifestation related to pericoronitis, showed no significant difference between the study groups [23, 27, 28].
The improvement in pain and edema/erythema extent, evaluated 7 days after treatment, may be related to the early stage of inflammation in the study patients, where symptoms such as pain and local swelling are more noticeable. Additionally, the possibility of an early stage of inflammation may also explain the lack of perceived influence on mouth opening, plaque index, and bleeding on probing, as the pre-treatment time was not sufficient for inflammation to spread to surrounding regions, with no systemic changes observed in the patients [29]. These factors may be related to the quality of patient’s oral hygiene, as cases of less acute pericoronitis are more common in patients with good or moderate oral hygiene [30], as well as related to the “Hawthorne Effect,” where patients behave differently due to being evaluated. The improvement in the edema/erythema extent for clinical use represents an enhancement in patient comfort and a possible reduction in inflammation.
It is known that mechanical debridement contributes to reducing plaque index and bleeding on probing, as evidenced by studies [31, 32], thereby improving patients’ health status and, consequently, their quality of life. Additionally, the improvement in quality of life observed in both groups through the OHIP-14 questionnaire assessment may be related to the reduction in clinical parameters and, consequently, the improvement in patients’ inflammatory conditions.
Previous studies have shown that pericoronitis treatment, either through periodontal care or third molar extraction, improves patients’ quality of life, using the same quality of life assessment questionnaire as this study [6, 32–35]. There was no significant difference in intergroup evaluation, suggesting that the results of ozonated water are similar when used as an adjunct in pericoronitis treatment. An important finding of the study is the improvement in the quality of life of control patients when using a specific periodontal disease questionnaire [18], possibly related to the improvement in their clinical parameters.
Despite the importance of pilot studies in assessing the feasibility of methodologies for main studies, they cannot be relied upon solely to determine the significance of findings in clinical studies [36]. However, they serve as models for methodological improvements in future studies and sample size calculation [24, 37]. Therefore, studies with larger samples should be conducted to seek clarification for these inquiries.
Methodologically, ensuring equality in baseline characteristics between study groups is crucial to avoid initial differences that could confound comparisons throughout the research. Moreover, it becomes a critical factor in ensuring that results can be attributed to the treatment or intervention under study rather than initial group differences [38].
Limitations
It’s challenging to assess various clinical parameters and achieve significant differences using a pilot study methodology, even if it’s triple-blinded and with low chances of biases. Furthermore, the contact time of ozonated water with pericoronitis was too short, considering it only lasted during irrigation treatment. Therefore, studies with larger sample sizes and good methodological quality should be conducted.
Additionally, different groups should be added to the methodology, some with alternatives (such as rinsing with ozonated water after a certain treatment period or using ozonated oil) that allow the affected area to have more contact time with the ozonated substance. Also, challenging patients should be included, such as smokers and diabetics, in whom ozonated water may provide additional benefits.
Clinical implication
In summary, this study proposed a new adjunctive treatment approach for pericoronitis, aiming to compare it with standard treatment in improving clinical parameters and quality of life. The results demonstrated that ozonated water showed similar effects to saline solution, with both also improving patient quality of life. Translating these findings to routine clinical practice, it can be speculated that ozonated water is an alternative irrigant for debridement treatments of pericoronitis cases.
Conclusion
Adjunct treatment with ozonated water or saline solution led to clinical improvement and enhanced quality of life in pericoronitis patients, with no difference between the groups. Therefore, the use of ozonated water can be considered an effective alternative in pericoronitis treatment, although further research is needed to gain a comprehensive understanding of its benefits and potential applications in dentistry.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blakey GH, White RP Jr, Offenbacher S, Phillips C, Delano EO, Maynor G. Clinical/biological outcomes of treatment for pericoronitis. journal of oral and maxillofacial surgery: official journal of the American association of oral and maxillofacial surgeons. 1996;54(10):1150–60. 10.1016/s 0278-2391(96)90339-010.1016/s 0278-2391(96)90339-08859232 · doi ↗ · pubmed ↗
- 2Tang DT, Phillips C, Proffit WR, Koroluk LD, White RP Jr. Effect of quality of life measures on the decision to remove third molars in subjects with mild pericoronitis symptoms. journal of oral and maxillofacial surgery: official journal of the American association of oral and maxillofacial surgeons. 2014;72(7):1235–43. 10.1016/j.joms.20110.1016/j.joms.2014.03.02224836419 · doi ↗ · pubmed ↗
- 3Gomes AS, Abegg C. The impact of oral health on the daily performance of municipal waste disposal workers in Porto Alegre, Rio Grande do Sul State, Brazil. Cad Saude Publica. 2007;23(7):1707–1714, 2007. 10.1590/S 0102-311X 200700070002310.1590/s 0102-311x 200700070002317572821 · doi ↗ · pubmed ↗
- 4Silveira EM da, Galvão EL, M RA, S KH, M OBL, Oliveira DWD de, F OD, V FD, Gonçalves PF. Effect of Oxyflower® gel as an adjunct in pericoronitis treatment: A randomized, Triple-Blind clinical trial. Arch Curr Res Int. 2024;24(4):45–58. 10.9734/acri/2024/v 24i 4659.
- 5Colombo M, Gallo S, Garofoli A, Poggio C, Arciola CR, Scribante A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology. 2021;6;10(7):625. 10.3390/biology 1007062510.3390/biology 10070625 PMC 830117734356480 · doi ↗ · pubmed ↗
- 6Mc Nutt M, Partrick M, Shugars DA, Phillips C, White RP Jr. Impact of symptomatic pericoronitis on health-related quality of life. journal of oral and maxillofacial surgery: official journal of the American association of oral and maxillofacial surgeons. 2008;66(12):2482–7. 10.1016/j.joms.2008.07.00510.1016/j.joms.2008.07.00519022127 · doi ↗ · pubmed ↗