Pseudoprogression in Hepatocellular Carcinoma During Atezolizumab Plus Bevacizumab Therapy: A Case Report and a Review of Literature
Mikee Elaine U Wee, Chao-Hung Hung, Ming-Chao Tsai, Chien-Hung Chen, Yuan-Hung Kuo

TL;DR
A rare case of pseudoprogression in liver cancer during immunotherapy is reported, highlighting the importance of combining imaging with clinical markers to avoid stopping effective treatment.
Contribution
This is the first reported case of pseudoprogression in hepatocellular carcinoma during atezolizumab plus bevacizumab therapy in a female patient.
Findings
A 63-year-old woman with advanced HCC showed initial tumor enlargement on imaging but later tumor regression.
Serum alpha-fetoprotein levels decreased significantly, indicating treatment response despite radiological pseudoprogression.
Abstract
Pseudoprogression is an atypical response pattern to immune checkpoint inhibitors (ICIs), characterized by initial tumor enlargement or the appearance of new lesions, followed by subsequent tumor regression. While this phenomenon has been observed in several solid tumors, its occurrence in hepatocellular carcinoma (HCC) is rare and not well understood, presenting diagnostic and therapeutic challenges. We report the first female case of HCC pseudoprogression during atezolizumab and bevacizumab therapy. The patient is a 63-year-old woman with chronic hepatitis B-related advanced HCC. After multiple prior treatments, she was started on combination therapy with atezolizumab and bevacizumab. Following four treatment cycles, imaging revealed tumor enlargement and new small lesions, suggestive of disease progression. However, her serum alpha-fetoprotein (AFP) level had decreased from 45,598…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
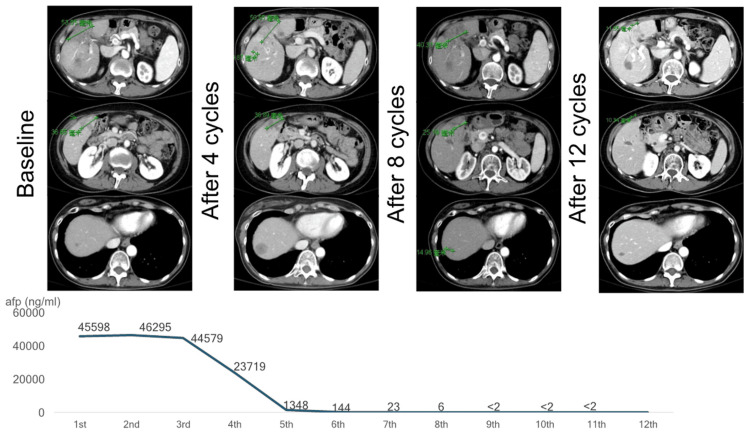 Figure 1
Figure 1| Year | Reference | Profile | Case | Etiology | Prior treatment | Baseline AFP level (ng/mL) | Time of PsP | Type of PsP | AFP level (ng/mL) at the time of PsP | Response (RECIST 1.1) |
| 2021 | [ | 74/male | HCC with lung, bilateral iliac, and pelvic LN metastasis | Alcoholic | TACE | ~4,000 | After the second course | Increased size of the lung, bilateral iliac, and pelvic LN metastatic tumors; increased number of lung metastases | ~6,500 | PR |
| 2022 | [ | 30/male | Fibrolamellar HCC with LN metastasis | Non-viral | None | 9.8 | After the fourth course | Increased size of the LN metastasis | Normalization | PR |
| 2023 | [ | 56/male | BCLC stage B HCC | Alcoholic liver and hepatitis C (SVR) | TACE | ~20 | After the third course | Increased size of tumors | ~80 | CR |
| 2023 | [ | 70/male | HCC with lung metastasis, PV invasion, and RHV invasion | Hepatitis C | TACE, ×2 | 8,416 | After the second course | Increased size of tumor; progression of vascular invasion; increased number of lung metastases | ~8,500 | PR |
| 2024 | [ | 70/male | Moderately differentiated HCC with microvascular invasion | Non-viral | Hepatectomy | 39.1 | After the second course | Increased size of tumors | 6 | PR |
| 2024 | [ | 62/male | HCC with lung metastasis | Non-viral | Hepatectomy | ~9,000 | After the fourth course | Increased size of liver tumor; increased size of lung metastasis | Decreased | CR (lung) and PR (liver) |
| 2025 | [ | 65/male | Poorly differentiated HCC with lung metastasis, with cervical and abdominal LN metastasis | Alcoholic | None | 37,671 | After four days | New liver tumors | Not tested | PR |
| Current case | 63/female | HCC with PV thrombus | Hepatitis B | Hepatectomy, RT, and lenvatinib | 45,598 | After the fourth course | Increased size of one tumor and new lesions | 23,719 | PR | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Colorectal Cancer Treatments and Studies · Cancer Immunotherapy and Biomarkers
Introduction
Pseudoprogression is an atypical tumor response characterized by an initial increase in tumor size or the emergence of new lesions, followed by subsequent regression [1]. This phenomenon is hypothesized to result from T-cells infiltrating into the tumor, leading to temporary lesion enlargement as part of an immune-mediated therapeutic response [2,3]. Unfortunately, this can be misinterpreted as treatment failure, potentially resulting in the premature discontinuation of effective therapies.
With the growing use of immune checkpoint inhibitors (ICIs) in cancer treatment, recent research has focused on better identifying pseudoprogression, leading to the development of immune-related response evaluation criteria (irRECIST) to differentiate it from true tumor progression [1]. However, a retrospective multicenter study suggests that continuing nivolumab treatment in advanced hepatocellular carcinoma (HCC) patients with unconfirmed progressive disease may offer limited clinical benefit due to the low likelihood of pseudoprogression [4]. Currently, for patients with advanced or unresectable HCC, combination therapy with the anti-programmed cell death-ligand 1 (anti-PD-L1) agent atezolizumab and the anti-vascular endothelial growth factor (anti-VEGF) A agent bevacizumab has shown superior progression-free and overall survival compared to sorafenib and is now considered the standard systemic therapy in this setting [5]. Although rare in HCC compared to other solid tumors, pseudoprogression associated with ICIs, particularly atezolizumab plus bevacizumab, remains poorly understood and presents a diagnostic and therapeutic challenge.
Herein, we present a compelling case of pseudoprogression in a patient with HCC treated with atezolizumab plus bevacizumab, followed by a remarkable therapeutic response. We also provide a literature review to enhance the understanding of previously reported cases. This case illustrates the diagnostic complexity of pseudoprogression in HCC during atezolizumab plus bevacizumab therapy, particularly in a female patient, a demographic rarely represented in existing reports. It highlights the limitations of conventional imaging-based response criteria and underscores the importance of integrating clinical status and tumor markers into treatment evaluation.
Case presentation
A 63-year-old Taiwanese woman was referred to our service for continuity of care. She was a case of HCC stage T1N0M0 and Barcelona clinic liver cancer (BCLC) stage A on the background of hepatitis B on tenofovir alafenamide, who underwent lateral segmentectomy and cholecystectomy. Postoperatively, she had experienced multiple episodes of tumor recurrence with tumor thrombus and underwent radiofrequency ablation and radiotherapy on separate episodes, despite starting on lenvatinib and having it discontinued later on due to tumor progression.
Four years post operation, she was again diagnosed with three HCC tumor recurrences seen on CT scan (unidimensional at 5.4 cm, 3.7 cm, and <1.0 cm at segments 4-5, segment 5, and segment 7, respectively), with concurrent serum alpha-fetoprotein (AFP) level of 45,598 ng/mL. The patient was diagnosed with a case of advanced, unresectable HCC. She was advised to undergo immunotherapy (atezolizumab 1,200 mg and bevacizumab 500 mg). After four cycles of immunotherapy, there was a significant increase in the size of one of the tumors (unidimensional from <1.0 cm to ~3.0 cm at segment 7), despite a contradicting significantly decreased AFP level at 23,719 ng/mL. The patient was still advised to continue her current treatment. After eight cycles of immunotherapy, there were a modest decrease in the size of the tumors (unidimensional at 4.0 cm, 2.5 cm, and 1.5 cm) and a drastic decrease in the serum AFP level to 6 ng/mL. As her immunotherapy reached the 12th cycle, there was a notable partial response: progressive decrease in both the size of the tumors of 78%, 73%, and 30% (unidimensional at 1.2 cm, 1.0 cm, and 1.3 cm, respectively) and serum AFP level to <2 ng/mL. By RECIST 1.1 or irRECIST criteria, the patient has exhibited a partial response or an immune-related partial response, respectively. To date, the patient has been continuously receiving atezolizumab and bevacizumab without any minor or major adverse events with close monitoring and follow-up. She has been doing well and was able to perform her usual daily activities (Figure 1).
Patient serum AFP trends and CT imaging while on atezolizumab and bevacizumabAFP: alpha-fetoprotein
Discussion
Pseudoprogression is an atypical response pattern observed in various malignancies, including melanoma (6.4%), non-small cell lung cancer (5%), and genitourinary cancers (7%) among patients receiving ICI therapy [6]. Although pseudoprogression is rarely reported in HCC, the awareness of this phenomenon is increasing as the use of ICIs becomes more widespread. In this report, we describe a 63-year-old woman with hepatitis B-related, advanced, unresectable HCC who was initially treated with lenvatinib as first-line therapy. Following the fourth cycle of atezolizumab plus bevacizumab, imaging suggested disease progression, despite a concurrent decline in serum AFP levels. However, subsequent imaging after the eighth and 12th cycles revealed a marked reduction in both tumor burden and AFP levels, confirming pseudoprogression. This case underscores the importance of cautiously interpreting early imaging results and highlights the need for prolonged monitoring before modifying treatment plans.
A comprehensive literature review using the PubMed database identified seven published case reports of HCC pseudoprogression associated with atezolizumab plus bevacizumab therapy [3,7-12]. These cases are summarized in Table 1. Most patients were older adults, except one case involving a younger individual with fibrolamellar HCC [8]. Notably, our case is the only reported instance involving a female patient. Interestingly, the majority (62.5%) of pseudoprogression cases occurred in patients without underlying hepatitis B or C infection. Only three cases involved viral hepatitis: two with hepatitis C and our current case with hepatitis B [9,10].
The pathogenesis of HCC pseudoprogression remains poorly understood, and its association with underlying etiology is an area of active inquiry. Some evidence suggests that the etiology of HCC may influence the response to ICIs, with potentially reduced efficacy observed in non-viral HCC, particularly those associated with nonalcoholic fatty liver disease [13]. However, current randomized controlled trials have not been stratified by etiology, and such findings derive from post hoc, non-prespecified subgroup analyses [5]. Whether non-viral etiologies are more prone to pseudoprogression remains an open question warranting further investigation.
While studies in other malignancies suggest that tumor markers can help support a diagnosis of pseudoprogression, the utility of AFP and protein induced by vitamin K absence-II (PIVKA-II) in HCC is not yet well established. In our review, although half of the reported cases demonstrated a declining AFP level during pseudoprogression, two cases exhibited increased AFP, and one showed stable levels. These findings suggest that tumor markers alone may not reliably distinguish pseudoprogression from true progression. Nonetheless, clinical improvement alongside declining AFP levels, despite radiologic progression, should raise suspicion for pseudoprogression [3,12]. As a single case report, the findings are inherently limited in generalizability by the absence of biopsy confirmation and long-term follow-up. Emerging techniques such as radiomics and the identification of predictive biomarkers, including immune-related gene signatures or circulating tumor DNA, may offer valuable tools to differentiate pseudoprogression from true progression in HCC [14,15]. Although still in early stages of validation, these approaches warrant further investigation to enhance clinical decision-making during immunotherapy.
Conclusions
To our knowledge, this is the first reported case involving a female patient with hepatitis B-related HCC showing pseudoprogression undergoing treatment with atezolizumab plus bevacizumab. Differentiating pseudoprogression from true disease progression in HCC patients receiving immunotherapy remains a major clinical challenge. Recognizing this phenomenon is critical to prevent the premature discontinuation of potentially effective treatments. Ongoing research and the accumulation of clinical data are essential to enhance our understanding of the incidence, pathogenesis, and clinical relevance of pseudoprogression, as well as to establish optimal diagnostic and management strategies in HCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1i RECIST: guidelines for response criteria for use in trials testing immunotherapeutics Lancet Oncol Seymour L Bogaerts J Perrone A 05218201710.1016/S 1470-2045(17)30074-8PMC 564854428271869 · doi ↗ · pubmed ↗
- 2JAMA Oncology patient page. Immune checkpoint inhibitors JAMA Oncol West HJ 115120152618231510.1001/jamaoncol.2015.0137 · doi ↗ · pubmed ↗
- 3Hepatocellular carcinoma presenting with pseudoprogression in a patient receiving atezolizumab plus bevacizumab combination therapy Intern Med Osuga T Kubo T Miyanishi K 202510.2169/internalmedicine.4710-24PMC 1233132539756877 · doi ↗ · pubmed ↗
- 4Outcome of initial progression during nivolumab treatment for hepatocellular carcinoma: should we use i RECIST?Front Med (Lausanne) Lee DH Hwang S Koh YH 771887820213496675710.3389/fmed.2021.771887 PMC 8710731 · doi ↗ · pubmed ↗
- 5Updated efficacy and safety data from I Mbrave 150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma J Hepatol Cheng AL Qin S Ikeda M 8628737620223490253010.1016/j.jhep.2021.11.030 · doi ↗ · pubmed ↗
- 6Incidence of pseudoprogression during immune checkpoint inhibitor therapy for solid tumors: a systematic review and meta-analysis Radiology Park HJ Kim KW Pyo J Suh CH Yoon S Hatabu H Nishino M 879629720203274920410.1148/radiol.2020200443 PMC 7526949 · doi ↗ · pubmed ↗
- 7A case of pseudoprogression in hepatocellular carcinoma treated with atezolizumab plus bevacizumab J Investig Med High Impact Case Rep Watanabe Y Ogawa M Tamura Y 232470962110584899202110.1177/23247096211058489 PMC 863739934845921 · doi ↗ · pubmed ↗
- 8Atezolizumab and bevacizumab combination therapy and sequential conversion hepatectomy for advanced fibrolamellar hepatocellular carcinoma presenting pseudoprogression Liver Cancer Matsuki R Okano N Hasui N 1801831220233732549610.1159/000527250 PMC 10267524 · doi ↗ · pubmed ↗