A rare case of severe acute pancreatitis complicated by gastric fistula and total splenic liquefaction
Xin Huang, Ximei Cao, Yao Wu, Liang Xia, Yin Zhu, Nonghua Lu, Wenhua He

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
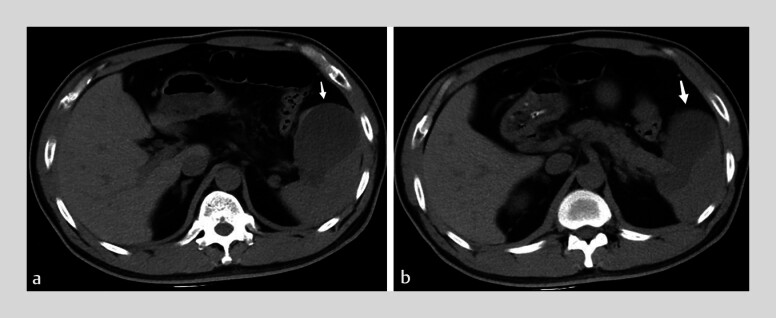 Fig. 1
Fig. 1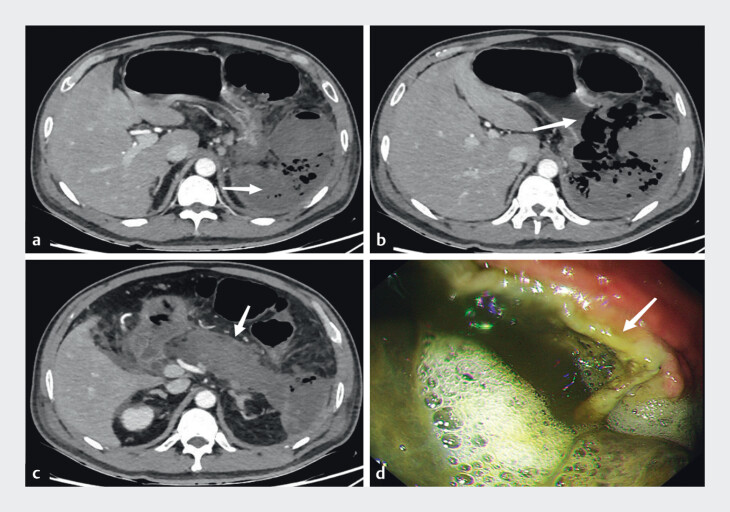 Fig. 2
Fig. 2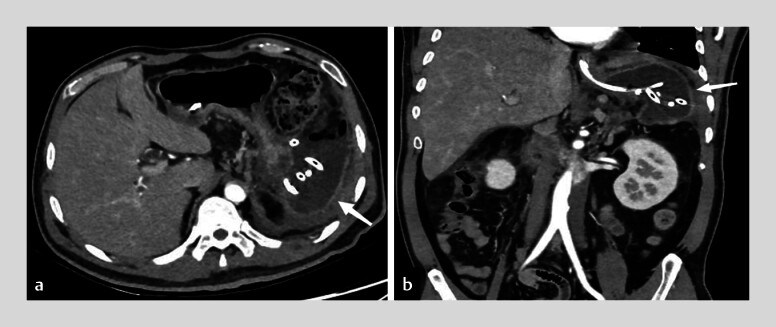 Fig. 3
Fig. 3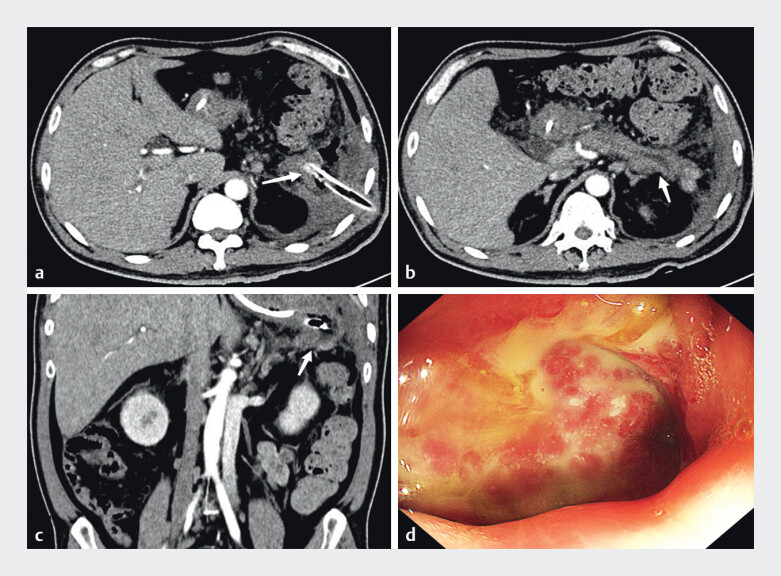 Fig. 4
Fig. 4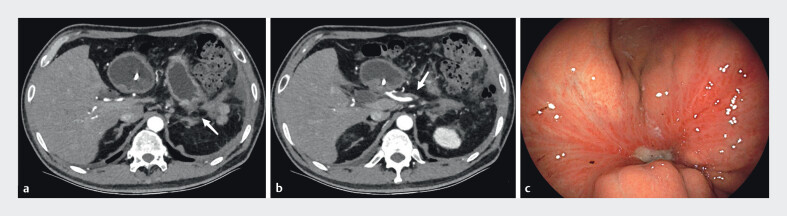 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Biliary and Gastrointestinal Fistulas
A 44-year-old man was admitted in June 2024 with persistent abdominal pain and a history of diabetes with acute pancreatitis 7 months prior. Laboratory tests showed a white blood cell count of 25.13 × 10⁹/L (neutrophils 92.5%), triglycerides 6.58 mmol/L, and amylase 602.4 U/L. Abdominal CT demonstrated acute pancreatitis with a 4-cm pseudocyst at the pancreatic tail ( Fig. 1 ). During hospitalization, the patient developed recurrent fever, abdominal rigidity, and left upper quadrant tenderness. CT performed at 1 week after disease onset revealed necrotizing pancreatitis with complete absence of the spleen, which was replaced by patchy hypodense areas with gas bubbles. Gastric fistula was identified by a discontinuity in the greater curvature of the upper gastric body ( Fig. 2 ). Despite antibiotics and nutritional support, percutaneous drainage of splenic necrosis and pancreatic walled-off necrosis were necessary ( Fig. 3 ). A nasojejunal tube was endoscopically placed distal to the gastric fistula for enteral nutrition. At week 6, endoscopic necrosectomy via the percutaneous sinus tract was attempted but failed due to large necrotic debris. Successful debridement was achieved endoscopically through the gastric fistula ( Video 1 ). Postoperative CT showed resolution of necrosis, and gastroscopy demonstrated fistula shrinkage ( Fig. 4 ). The patient was discharged clinically improved. Two-month follow-up confirmed complete resolution of peripancreatic necrosis and fistula healing ( Fig. 5 ).
CT demonstrates a pseudocyst at the pancreatic tail adjacent to the spleen (arrows) in a 44-year-old man.
a Complete splenic necrosis with absence of splenic parenchyma (arrow). b Discontinuity of gastric wall indicating fistula formation (arrow). c Global pancreatic necrosis with predominant parenchymal involvement (arrow). d Endoscopic view of gastric fistula (arrow).
Percutaneous drainage of pancreatic necrosis (arrows indicate catheter).
Endoscopic necrosectomy procedure for pancreatic necrosis.Video 1
a–c Near-complete resolution of necrotic collections after debridement (arrows mark residual cavities). d Endoscopic image showing improvement of gastric fistula following necrosectomy.
a, b Follow-up CT at 2 months shows complete resolution of necrosis (arrows denote original sites). c Endoscopic confirmation of near-total fistula healing.
This is the first reported case of severe acute pancreatitis with concurrent gastric fistula and total splenic autolysis. Gastrointestinal fistulas in pancreatitis typically involve the duodenum or colon 1 . Gastric fistulas are rare; the one in this case likely resulted from pancreatic enzyme extravasation and local inflammation. Although splenic involvement can occur in severe acute pancreatitis 2 , complete splenic liquefaction is exceedingly rare. It may be attributed to: (1) direct enzymatic autodigestion by trypsin from the ruptured pancreatic pseudocyst (formed during the prior pancreatitis episode); and (2) splenic vein thrombosis causing ischemic necrosis 3 4 .
Endoscopy_UCTN_Code_CCL_1AZ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang D Yue L Tan B Comprehensive management of gastrointestinal fistulas in necrotizing pancreatitis: a review of diagnostic and therapeutic approaches Expert Rev Gastroenterol Hepatol 202510.1080/17474124.2025.246983539968762 · doi ↗ · pubmed ↗
- 2Louis M Ayinde B Gibson B Spontaneous splenic rupture in severe acute pancreatitis: a rare life-threatening complication and its successful management Cureus 202517 e 8035410.7759/cureus.8035440206930 PMC 11981545 · doi ↗ · pubmed ↗
- 3Wang F Zhou B Gong W The risk of splenic rupture in pancreatitis: when the pancreatic tail adheres to the splenic hilum Asian J Surg 202473167316810.1016/j.asjsur.2024.03.03038490872 · doi ↗ · pubmed ↗
- 4Xie CL Zhang M Chen Y Spleen and splenic vascular involvement in acute pancreatitis: an MRI study Quant Imaging Med Surg 2018829130010.21037/qims.2018.03.0429774182 PMC 5941205 · doi ↗ · pubmed ↗