Anchoring wire technique for additional stent placement after endoscopic ultrasonography-guided hepaticogastrostomy
Kazuki Endo, Haruo Miwa, Ritsuko Oishi, Yuichi Suzuki, Kazuya Sugimori, Kazushi Numata, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
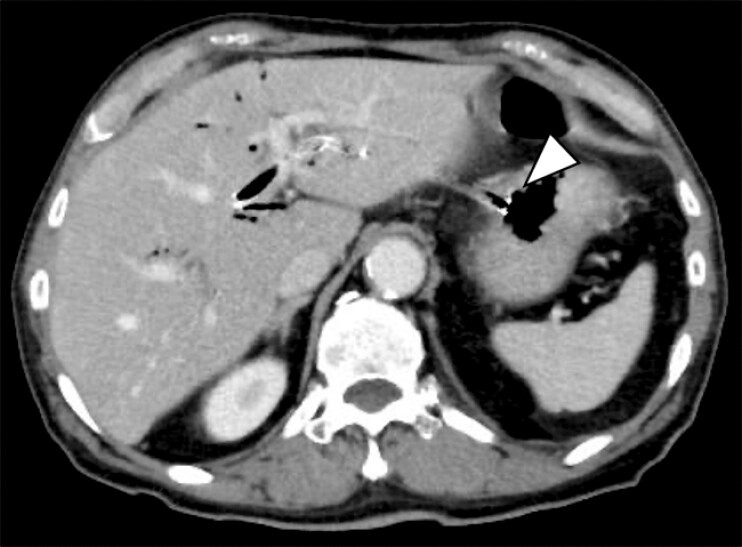 Fig. 1
Fig. 1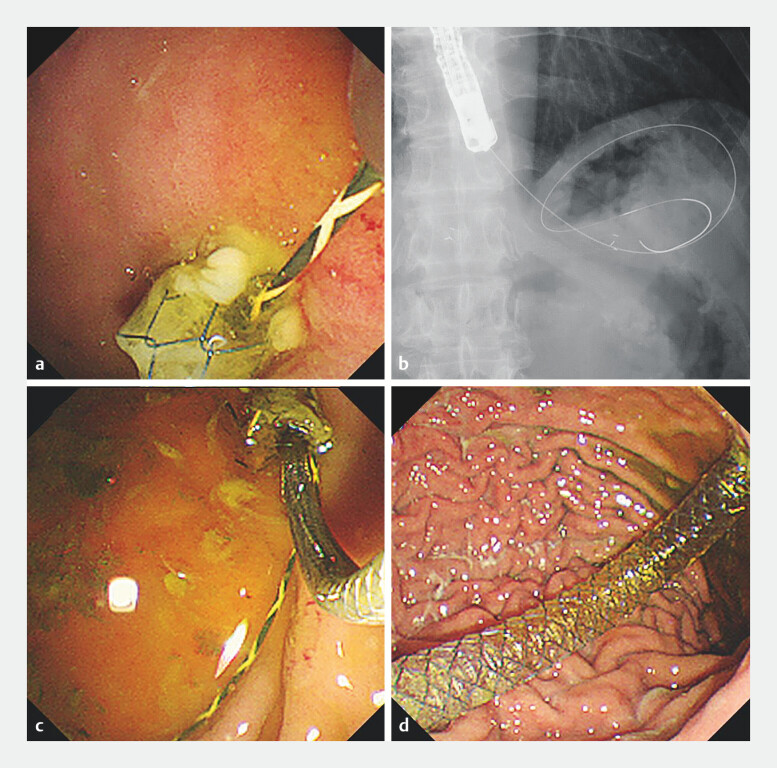 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Cholangiocarcinoma and Gallbladder Cancer Studies · Pediatric Hepatobiliary Diseases and Treatments
Endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS) has been reported to have a high technical success rate; however, severe complications occasionally occur 1 . Among these, migration of a self-expandable metal stent (SEMS) into the abdominal cavity during and after EUS-HGS is a potentially fatal complication 2 3 . In cases where the SEMS becomes partially dislodged toward the abdominal cavity, resulting in a shortened intragastric length, additional SEMS placement has been reported 4 ; however, it carries the risk of pushing the SEMS into the abdominal cavity. Herein, we report a novel anchoring wire technique during additional SEMS placement after EUS-HGS ( Video 1 ).
An additional SEMS was safely placed using the anchoring wire method for the partially dislodged SEMS after EUS-HGS.Video 1
A 71-year-old man with unresectable ampullary carcinoma was admitted for cholangitis due to occlusion of SEMS. Endoscopic retrograde cholangiopancreatography was performed; however, additional SEMS placement failed due to tumor invasion in the second portion of the duodenum. Therefore, EUS-HGS was performed after nasobiliary drainage, and a fully covered SEMS (HANARO Benefit, 8-mm, 12-cm; Boston Scientific, Marlborough, Massachusetts, USA) was deployed in B3. The following day, computed tomography images revealed that the gastric side of the SEMS had partially dislodged toward the abdominal cavity ( Fig. 1 ). An emergency endoscopic reintervention was performed for additional SEMS placement. The stent cover was penetrated using a tapered catheter, and the sufficient length of a 0.025-inch guidewire (VisiGlide 2, Olympus medical systems, Tokyo, Japan) was inserted through the mesh gap and left in the stomach as an anchoring wire. Subsequently, a second guidewire was advanced into the SEMS from the gastric end, and an additional SEMS, identical to the previous stent, was successfully deployed without stent migration ( Fig. 2 ).
Computed tomography on the day after EUS-HGS reveals that the gastric side of the SEMS is partially dislodged toward the abdominal cavity (arrowhead).
Additional SEMS placement using anchoring wire method. a Silicon cover of the SEMS is penetrated using a tapered catheter and a 0.025-inch guidewire is inserted through the mesh gap. b A sufficient length of the guidewire is left in the stomach. c A delivery system of the additional SEMS is inserted from the gastric end. d The anchoring wire is removed just before the additional SEMS placement and the additional SEMS is successfully placed.
To the best of our knowledge, this is the first report of novel anchoring wire technique to prevent SEMS migration during reintervention after EUS-HGS. This method is useful as a rescue technique for additional SEMS placement.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Binda C Dajti E Giuffrida P Efficacy and safety of endoscopic ultrasound-guided hepaticogastrostomy: a meta-regression analysis Endoscopy 20245669470510.1055/a-2282-335038447958 · doi ↗ · pubmed ↗
- 2Martins FP Rossini LG Ferrari AP Migration of a covered metallic stent following endoscopic ultrasound-guided hepaticogastrostomy: fatal complication Endoscopy 20104202 E 126E 12710.1055/s-0029-124391120405376 · doi ↗ · pubmed ↗
- 3Okuno N Hara K Mizuno N Stent migration into the peritoneal cavity following endoscopic ultrasound-guided hepaticogastrostomy Endoscopy 20154701 UCTNE 31126115390 10.1055/s-0034-1392314 · doi ↗ · pubmed ↗
- 4Ogura T Kurisu Y Masuda D Novel method of endoscopic ultrasound-guided hepaticogastrostomy to prevent stent dysfunction J Gastroenterol Hepatol 2014291815182110.1111/jgh.1259824720511 · doi ↗ · pubmed ↗