Endoscopic ultrasound-guided lauromacrogol embolization for suspected Zollinger–Ellison syndrome: a novel approach
Fangfang Guo, Bo Li, Lingfang Shi, Hongtan Chen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
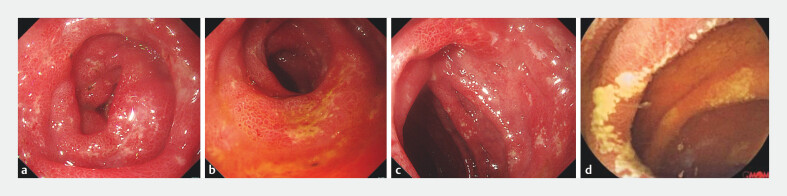 Fig. 1
Fig. 1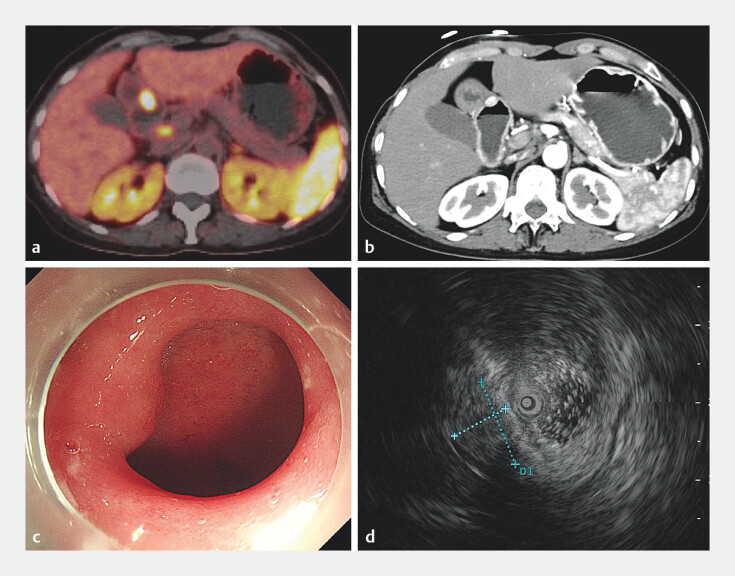 Fig. 2
Fig. 2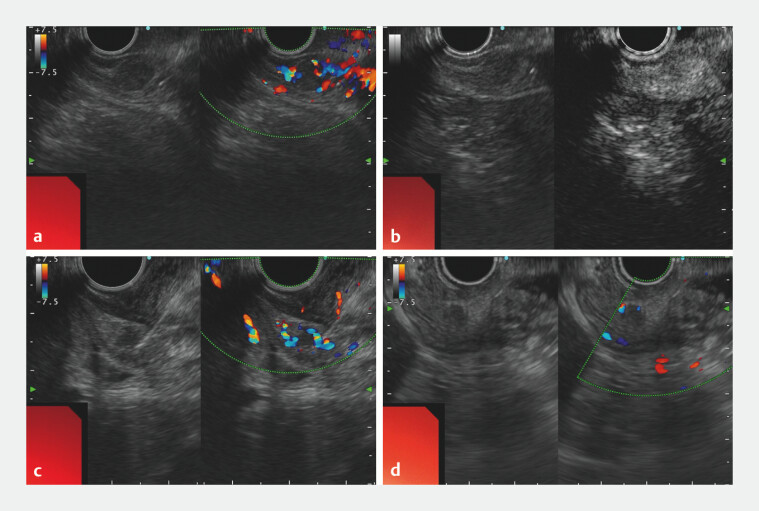 Fig. 3
Fig. 3- —National Natural Science Foundation of China10.13039/501100001809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Tuberous Sclerosis Complex Research · Fibroblast Growth Factor Research
Zollinger–Ellison syndrome is a rare condition caused by gastrin-secreting neuroendocrine tumors, leading to severe gastric acid hypersecretion, peptic ulcers, and diarrhea 1 . Accurate diagnosis remains challenging, requiring characteristic clinical symptoms, hypergastrinemia, and tumor localization through advanced imaging techniques 2 . Though conventional treatments include high-dose proton pump inhibitors, somatostatin analogs, or surgery 3 , we present a groundbreaking case of suspected Zollinger–Ellison syndrome successfully managed with endoscopic ultrasound (EUS)-guided lauromacrogol embolization, offering a minimally invasive yet highly effective therapeutic alternative.
A 58-year-old woman presented with a 5-month history of refractory watery diarrhea (up to 20 episodes daily) and weight loss of 10 kg. Previous hospitalizations showed partial response to octreotide but no improvement with antispasmodics or probiotics. Laboratory investigations revealed markedly elevated fasting serum gastrin (913.0 pg/mL). Upper endoscopy demonstrated multiple atypical duodenal and jejunal ulcers ( Fig. 1 ), and ¹⁸F-octreotide positron emission tomography and computed tomography identified a 1.5-cm hypermetabolic nodule (maximum standardized uptake value 77.7) in the gastric antrum, suggestive of a gastrinoma. Subsequent EUS evaluation confirmed a hypoechoic, hypervascular submucosal mass originating near the pyloric orifice ( Fig. 2 ). Although EUS-guided fine-needle aspiration yielded no malignant cells, the collective clinical, biochemical, and radiological findings strongly supported a diagnosis of Zollinger–Ellison syndrome.
Gastroscopy and capsule endoscopy images of the patient. a–c Gastroscopy images showed multiple ulcer lesions in the duodenum. d Capsule endoscopy revealed atypical jejunal ulcers.
Imaging studies of the suspected tumor in the gastric antrum. a, b ¹⁸F-octreotide positron emission tomography and computed tomography (CT) ( a ) and contrast-enhanced CT ( b ) identified a 1.5-cm hypermetabolic nodule (maximum standardized uptake value 77.7) in the gastric antrum. c gastroscopy did not reveal any ulcer or submucosal tumor in the antrum. d Endoscopic ultrasound revealed a hypoechoic submucosal mass near the pyloric orifice.
Given the patient’s personal preference against invasive intervention, we performed EUS-guided embolization ( Video 1 ). A 22-gauge needle punctured the vessels feeding the lesion, followed by sequential injections of lauromacrogol. Post-procedural imaging confirmed complete occlusion ( Fig. 3 ). Remarkably, the patient’s symptoms resolved rapidly, and serum gastrin levels normalized upon discharge. At 4-month follow-up, she remained asymptomatic with no evidence of recurrence or procedure-related complications.
Endoscopic ultrasound-guided lauromacrogol embolization for suspected Zollinger–Ellison syndrome.Video 1
Endoscopic ultrasound (EUS)-guided lauromacrogol embolization for suspected gastrinomas in the gastric antrum. a EUS with color Doppler showed a hypoechoic, hypervascular submucosal mass originating near the pyloric orifice. b Contrast-enhanced harmonic EUS revealed intense arterial-phase enhancement. c A 22-gauge needle punctured the arteries feeding the lesion, followed by sequential injections of lauromacrogol. d EUS with color Doppler showed complete occlusion of target lesion.
EUS-guided lauromacrogol embolization represents an innovative and effective approach for the definitive ablation of suspected antral Zollinger–Ellison syndrome, offering a minimally invasive yet precise therapeutic option for small sporadic gastrinomas. Further prospective studies are needed to validate its long-term efficacy in managing functional neuroendocrine tumors.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Campana D Piscitelli L Mazzotta E Zollinger–Ellison syndrome. Diagnosis and therapy Minerva Med 20059618720616175161 · pubmed ↗
- 2Rossi RE Elvevi A Citterio D Gastrinoma and Zollinger Ellison syndrome: a roadmap for the management between new and old therapies World J Gastroenterol 2021275890590734629807 10.3748/wjg.v 27.i 35.5890 PMC 8475006 · doi ↗ · pubmed ↗
- 3Chatzipanagiotou O Schizas D Vailas M All you need to know about gastrinoma today | gastrinoma and Zollinger–Ellison syndrome: a thorough update J Neuroendocrinol 202335 e 1326737042078 10.1111/jne.13267 · doi ↗ · pubmed ↗