Endoscopic ultrasound-guided hepaticogastrostomy in a patient with complex postsurgical anatomy after subtotal esophagectomy
Kei Yane, Keita Seto, Koki Yoshida, Sota Hirokawa, Kotaro Morita, Yuki Ikeda, Tetsuya Sumiyoshi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
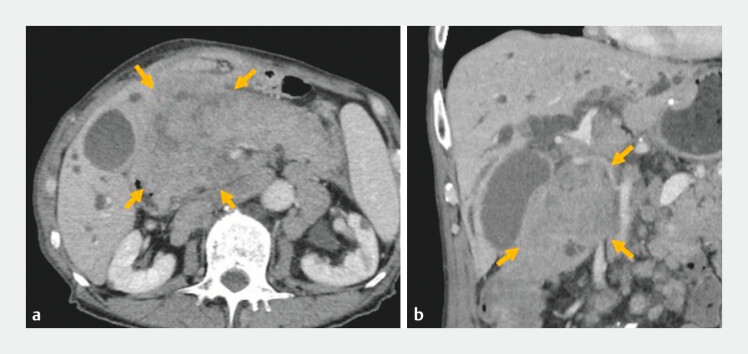 Fig. 1
Fig. 1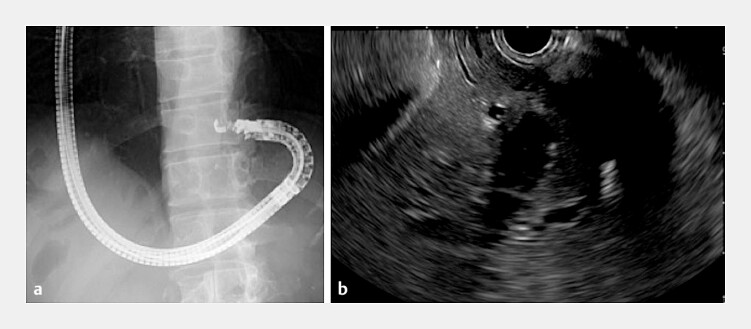 Fig. 2
Fig. 2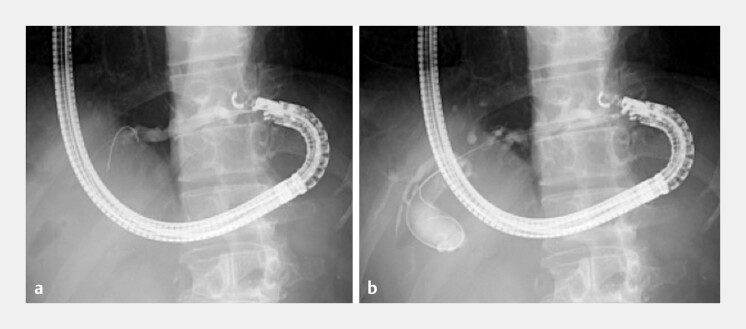 Fig. 3
Fig. 3 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Pancreatic and Hepatic Oncology Research · Esophageal Cancer Research and Treatment
In patients with complex upper gastrointestinal reconstruction, endoscopic biliary drainage is technically challenging. Recently, the usefulness of endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) in patients with surgically altered anatomy has been increasingly demonstrated 1 2 3 4 .
A 75-year-old man with a history of distal gastrectomy with Billroth I reconstruction for a duodenal ulcer and subtotal esophagectomy for esophagogastric junction cancer presented with a recurrent tumor and obstructive jaundice. Esophageal reconstruction was performed using a free jejunal interposition graft via the presternal route. Computed tomography revealed a duodenal obstruction from the tumor recurrence, precluding transpapillary biliary drainage ( Fig. 1 ). Therefore, EUS-HGS was planned to achieve internal biliary drainage.
Computed tomography showing intrahepatic bile duct dilation and duodenal obstruction because of the recurrent tumor (arrows). a Axial image. b Coronal image.
A long colonoscope was used to navigate the interposed jejunal limb, allowing guidewire placement in the stomach. The colonoscope was then exchanged for a curved linear echoendoscope (EG-740UT; Fujifilm, Tokyo, Japan), and the guidewire was followed under fluoroscopic guidance to reach the stomach ( Video 1 ). From a reversed position in the upper gastric body, a dilated intrahepatic bile duct (B2) was identified ( Fig. 2 ). The puncture was performed using a 22-G fine-needle aspiration needle (Expect Slimline; Boston Scientific, Marlborough, Massachusetts, USA), and a 0.018-inch guidewire (Fielder 18; Olympus, Tokyo, Japan) was advanced. The tract was dilated using a double-lumen dilator (MEISSA; Japan Lifeline, Tokyo, Japan) and a 4-mm balloon catheter (REN; Kaneka Medics, Osaka, Japan) ( Fig. 3 ). An 8 × 120-mm covered self-expandable metal stent (Niti-S Biliary S-type; Taewoong Medical, Gyeonggi-do, South Korea) was deployed ( Fig. 4 ).
a A curved linear echoendoscope was advanced into the stomach following the guidewire under fluoroscopic guidance. b From a reversed position in the upper gastric body, a dilated intrahepatic bile duct (B2) was identified.
a Puncture was performed using a 22-G fine-needle aspiration needle, and a 0.018-inch guidewire was advanced. b The tract was dilated using a 4-mm balloon catheter.
An 8 × 120-mm covered self-expandable metal stent was deployed.
Endoscopic ultrasound-guided hepaticogastrostomy in a patient with esophageal reconstruction using a free jejunal interposition graft via the presternal route.Video 1
The total procedure time was 58 minutes. There were no adverse events postoperatively, and jaundice resolved promptly. Stent dysfunction was not observed until the patient’s death from the primary disease.
EUS-HGS is a promising option for biliary drainage in patients with a malignant obstruction and complex surgical anatomy. Thorough preprocedural planning, including an understanding of the surgically altered anatomy and appropriate device selection, is essential for procedural success.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siripun A Sripongpun P Ovartlarnporn B Endoscopic ultrasound-guided biliary intervention in patients with surgically altered anatomy World J Gastrointest Endosc 2015728328910.4253/wjge.v 7.i 3.28325789101 PMC 4360449 · doi ↗ · pubmed ↗
- 2Balducci D Ratone J-P Schaefer MEUS-guided hepaticojejunostomy in patients with history of total gastrectomy: a multicenter retrospective feasibility study (with video)Gastrointest Endosc 202510111712239038522 10.1016/j.gie.2024.07.011 · doi ↗ · pubmed ↗
- 3ASGE Standards of Practice Committee Pawa S Marya NB American Society for Gastrointestinal Endoscopy guideline on the role of therapeutic EUS in the management of biliary tract disorders: summary and recommendations Gastrointest Endosc 202410096797939078360 10.1016/j.gie.2024.03.027 · doi ↗ · pubmed ↗
- 4Spadaccini M Giacchetto CM Fiacca M Endoscopic biliary drainage in surgically altered anatomy Diagnostics (Basel)202313362310.3390/diagnostics 1324362338132207 PMC 10742737 · doi ↗ · pubmed ↗