Tumor-to-Tumor Metastasis in a Patient With Hemangioblastoma Unrelated to von Hippel-Lindau Disease: A Case Report and Review of the Literature
Kyoichi Tomoto, Kentaro Watanabe, Takahiro Ogawa, Hisao Sano, Hiroki Suetsugu, Ryoto Wachi, Michihiro Tanaka, Yuichi Murayama, Toshihide Tanaka

TL;DR
A rare case of tumor-to-tumor metastasis involving breast cancer in a hemangioblastoma unrelated to von Hippel-Lindau disease is reported.
Contribution
This is the first reported case of TTM involving metastatic breast cancer to a sporadic hemangioblastoma unrelated to VHL.
Findings
A 61-year-old woman had TTM with metastatic breast cancer in a hemangioblastoma.
No evidence of von Hippel-Lindau disease was found in the patient.
The case emphasizes the need to consider TTM in CNS tumor differential diagnoses.
Abstract
Tumor-to-tumor metastasis (TTM) is a rare phenomenon in which one malignant tumor ("donor") metastasizes to another benign tumor ("recipient"). In the central nervous system (CNS), meningioma is considered one of the most frequent recipients, while hemangioblastoma (HGB) has also been reported, typically in association with von Hippel-Lindau (VHL) disease. A 61-year-old woman with a history of bilateral breast cancer treated 17 years earlier presented with right-sided ataxic hemiparesis. Magnetic resonance imaging revealed a gadolinium-enhanced mass in the right cerebellum, initially diagnosed as a metastatic brain tumor. Despite stereotactic radiotherapy, symptoms persisted and the lesion enlarged. Surgical resection was performed via the occipital trans-tentorial approach. Intraoperative findings revealed a reddish, vascular tumor with a xanthochromic area. Complete resection was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
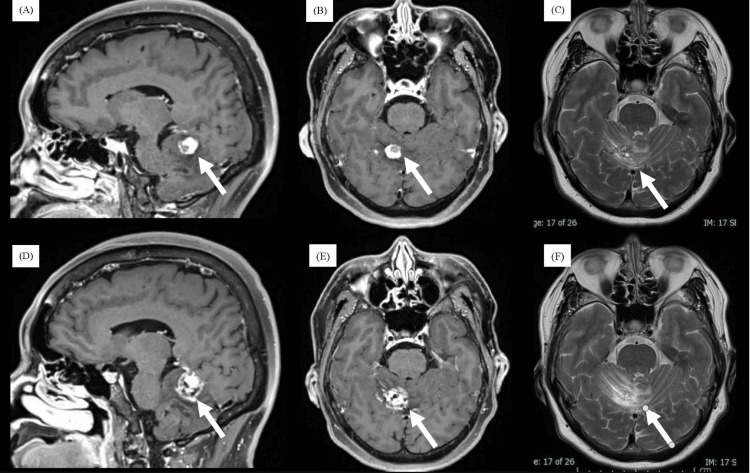 Figure 1
Figure 1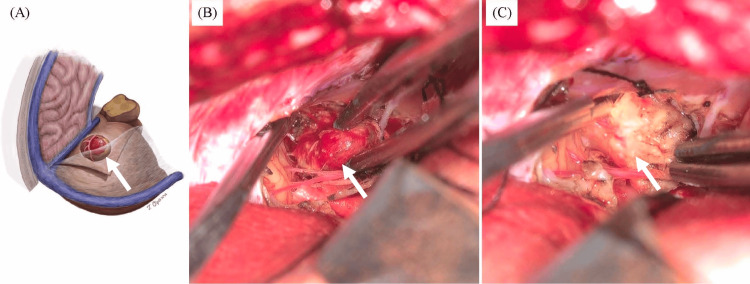 Figure 2
Figure 2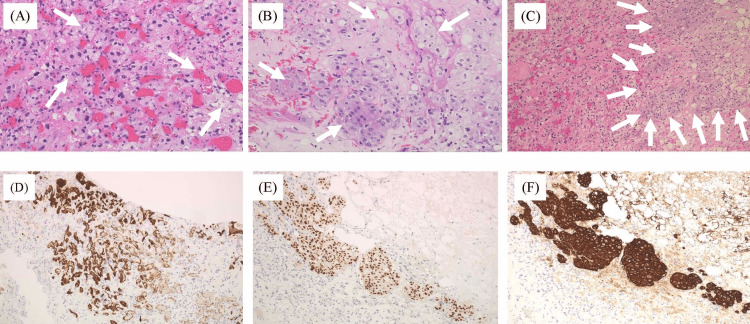 Figure 3
Figure 3| Number | Publication | Location | Primary tumor (donor) | Association with VHL |
| 1 |
Crockard et al., 1988 [ | Cerebellum | Prostate carcinoma | Not associated |
| 2 |
Jamjoom et al., 1992 [ | Cerebellum | RCC | Associated |
| 3 |
Bret et al., 1999 [ | Cerebellum | RCC | Associated |
| 4 |
Mottolese et al., 2001 [ | Cerebellum | RCC | Associated |
| 5 |
Hamazaki et al., 2001 [ | Cerebellum | RCC | Associated |
| 6 |
Hamazaki et al., 2001 [ | Spinal cord (thoracic) | RCC | Associated |
| 7 |
Fakih et al., 2001 [ | Spinal cord (cervical) | RCC | Associated |
| 8 |
Abou-Hamden et al., 2003 [ | Spinal cord (cervical) | RCC | Associated |
| 9 |
Altinoz et al., 2005 [ | Spinal cord (thoracic) | RCC | Associated |
| 10 |
Jarrell et al., 2006 [ | Cerebellum | RCC | Associated |
| 11 |
Jarrell et al., 2006 [ | Cerebellum | RCC | Associated |
| 12 |
Jarrell et al., 2006 [ | Spinal cord (thoracic) | RCC | Associated |
| 13 |
Jarrell et al., 2006 [ | Spinal cord (thoracic) | RCC | Associated |
| 14 |
Jarrell et al., 2006 [ | Spinal cord (sacrum) | RCC | Associated |
| 15 |
Jarrell et al., 2006 [ | Cerebellum | Pancreatic neuroendocrine tumor | Associated |
| 16 |
Polydorides et al., 2007 [ | Spinal cord (cervical) | RCC | Associated |
| 17 |
Martin et al., 2010 [ | Cerebellum | RCC | Associated |
| 18 |
Xiong et al., 2010 [ | Medulla oblongata | RCC | Associated |
| 19 |
Ichikawa et al., 2011 [ | Cerebellum | Mixed germ cell tumor | Not associated |
| 20 |
Reynolds et al., 2015 [ | Medulla oblongata, spinal cord (cervical) | Pancreatic neuroendocrine tumor | Associated |
| 21 |
Dessauvagie et al., 2015 [ | Cerebellum | RCC | Associated |
| 22 |
Dessauvagie et al., 2015 [ | Spinal cord (cervical) | RCC | Associated |
| 23 |
Rai et al., 2015 [ | Eye | RCC | Associated |
| 24 |
Tran et al., 2021 [ | Spinal cord (cervical) | RCC | Associated |
| 25 |
Wakita et al., 2021 [ | Spinal cord (thoracic) | RCC | Associated |
| 26 |
Holanda and Lopes, 2022 [ | Spinal cord (cervical) | RCC | Associated |
| 27 |
Xie et al., 2023 [ | Cerebellum | RCC | Associated |
| 28 |
Lou et al., 2023 [ | Ventricular triangle | RCC | Associated |
| 29 |
Wang et al., 2024 [ | Cerebellum | RCC | Associated |
| 30 | Present case | Cerebellum | Breast carcinoma | Not associated |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Hypoxia, and Metabolism · Medical Imaging and Pathology Studies · Head and Neck Surgical Oncology
Introduction
A condition in which an individual shows two tumors at the same time is referred to as double cancer and is relatively rare. In some cases, one malignant tumor (the “donor”) metastasizes to another benign tumor (the “recipient”), in a phenomenon known as tumor-to-tumor metastasis (TTM; also called “collision tumor”). The first report of TTM in the central nervous system (CNS) was in 1930 [1], and approximately 150 cases have been documented since then. Meningioma is the most common primary tumor site, and breast cancer is one of the most frequent metastatic brain tumors causing TTM in the CNS [2,3]. The second most common recipient site is hemangioblastoma (HGB), with renal cell carcinoma, which was related to von Hippel-Lindau (VHL) disease, probably due to its vascularity with a favorable microenvironment to grow the different tumor clones in the same place. In contrast, TTM in non-VHL HGB is exceptionally rare, and mechanisms may differ from VHL-associated cases. Here, we present the first case of TTM in the CNS from breast cancer in a patient with sporadic HGB that was unrelated to VHL disease.
Case presentation
Clinical course
A 61-year-old woman with a history of bilateral breast cancer treated 17 years earlier presented to our hospital with right-sided ataxic hemiparesis. The breast cancer had been positive for estrogen and progesterone receptors but showed low expression of human epidermal growth factor receptor 2. Following bilateral breast surgery, she had received additional radiotherapy and chemotherapy and was subsequently placed under regular follow-up. Although she had experienced a recurrence of breast cancer with supraclavicular lymph node and multiple bone metastases four years earlier, she had no other significant medical history. She also had no contributory family history.
Magnetic resonance imaging (MRI) revealed a small, gadolinium-enhanced mass lesion on the tentorial side of the right cerebellum (Figure 1A). A non-enhancing area was observed in the anteromedial portion of the tumor, demonstrating perifocal edema. Oncologists initially diagnosed the lesion as a metastatic brain tumor and recommended stereotactic radiotherapy (SRT) without confirmation of histology. The patient underwent SRT (35 Gy in five fractions), but symptoms persisted and the tumor continued to grow along with increasing perifocal edema (Figure 1B). Characteristics of the non-enhancing area differed from those seen prior to SRT.
Pre-SRT (A-C) and post-SRT (D-F) MRI images(A-C) Pre-SRT MRI, showing a sagittal gadolinium-enhanced image (A), axial gadolinium-enhanced image (B), and axial T2-weighted image (C). A tumor with gadolinium enhancement is observed on the superior surface of the right cerebellum.(D-F) Post-SRT MRI (4 months later), showing a sagittal gadolinium-enhanced image (D), axial gadolinium-enhanced image (E), and axial T2-weighted image (F).SRT: stereotactic radiotherapy; MRI: magnetic resonance imaging
Given the lack of improvement and the growth of the non-enhancing area after SRT, we suspected the lesion represented HGB rather than a metastatic brain tumor from breast cancer. Eight months after the SRT, a cerebellar tumor containing reddish and yellowish components was removed via an occipital trans-tentorial approach (OTA) (Figure 2A). The reddish component formed a round and solid tumor with abundant blood supply (Figure 2B) and was resected en bloc. The surrounding yellowish component was clearly demarcated from the reddish component and was soft and poorly vascularized. The yellowish component was also distinctly different from adjacent normal cerebellar tissue (Figure 2C). Both components were completely removed.
Illustration (A) and intraoperative photographs (B, C) during tumor resection via a right occipital trans-tentorial approach(A) Illustration of the reddish tumor and yellowish component before resection via the occipital trans-tentorial approach.(B) The reddish tumor emerging on the surface of the cerebellum during resection. The macroscopic appearance is suggestive of hemangioblastoma.(C) After removal of the reddish tumor, a yellowish component is resected. The boundary between the lesion and normal cerebellar tissue is clearly demarcated.
Postoperatively, neurological symptoms improved completely, and the patient was discharged nine days after surgery. Postoperative imaging showed the total removal of the tumor.
Pathological findings
Histopathological examination confirmed the reddish mass as HGB and the peritumoral yellowish lesions as metastatic brain tumor with necrotic tissues originating from the previous breast cancer (Figure 3). The tumor turned out to have two components. First, most of the tumor tissue comprised HGB, revealing proliferation of cells with clear, foamy cytoplasm surrounding a well-developed capillary network (Figure 3A).
Histological findings of the surgical specimens(A) Hemangioblastoma component showing numerous foamy stromal cells and a rich capillary network (H&E staining, ×200).(B) Metastatic breast carcinoma component with hyperchromatic nuclei, eosinophilic cytoplasm, and some vacuolated cells (H&E staining, ×200).(C) Sharp boundary between hemangioblastoma (left) and metastatic breast carcinoma (right) (H&E staining, ×100).(D-F) Immunohistochemistry showing focal positivity for CD31 in hemangioblastoma (D) and for GATA3 (E) and AE1/AE3 (F) in metastatic breast carcinoma.
The second component of the tumor was identified as metastatic breast carcinoma (Figure 3B). These cells showed hyperchromatic, enlarged nuclei and eosinophilic cytoplasm, with some displaying vacuolation.
The boundary between these two components was clearly depicted (Figure 3C), with the left side corresponding to HGB and the right to metastatic breast cancer. Based on these findings, the tumor was diagnosed as a TTM with HGB.
Immunohistochemically, tumor cells with clear, foamy cytoplasm were focally positive for CD31 (Figure 3D), leading to the confirmation of the diagnosis. The Ki-67 labeling index was approximately 1%-2%, indicating low proliferative activity in the reddish component. We finally diagnosed the reddish compartment of the tumor as HGB in the CNS. Further investigations did not demonstrate a diagnosis of VHL disease. Tumor cells in the yellow component showed positivity for pancytokeratin AE1/AE3 (Figure 3E) and the common breast cancer markers GATA3 and GCDFP-15 (Figure 3F). Genetic sequencing was performed to definitively exclude VHL.
Discussion
Here, we have presented the first description of TTM involving breast cancer metastasizing to HGB. Various reports have described TTM, but this pathology remains relatively rare in the CNS. So far, 29 metastases from other cancers to HGB in the CNS have been documented (Table 1) [4-25].
Among these, HGBs were located in the cerebellum in 13 cases, the spinal cord in 13 cases, the medulla oblongata in two cases, and the eye and trigone of the lateral ventricular in one case each. The most common donor tumor is renal cell carcinoma, accounting for 25 cases. Other donors include pancreatic neuroendocrine tumor (two cases), as well as prostate carcinoma and mixed germ cell tumor (one case each). Of these 29 cases, only those involving prostate carcinoma or mixed germ cell tumor were unrelated to VHL disease. The remaining 27 cases were all associated with VHL disease. The present case represents the first to show TTM with HGB as the recipient tumor and breast cancer as the donor tumor.
The mechanisms underlying TTM have been discussed in various studies but remain unclear. Meningioma and HGB appear reasonable to consider as frequent donor sites due to their rich vascularity, but high vascularity alone does not fully explain this phenomenon. A well-nourished and slow-growing element is necessary in the recipient tumor to provide a favorable microenvironment for the donor tumor. This reasoning helps explain why gliomas are rarely reported as recipients despite their vascularity [26]. With respect to recipient tumors, meningiomas are often supplied by extra-cranial arteries, which disregard the protective effects of the blood-brain barrier and enable other tumors to metastasize. In contrast, HGBs are primarily supplied by blood flow from intracranial arteries, challenging this theory. Unlike meningiomas, which may be influenced by tumor vascularity, tumor vessels toward HGBs were derived from the intra-axial tumor.
In addition, for TTM involving meningiomas and breast cancer or VHL-related HGB, hormonal or genetic factors have been suggested as contributing mechanisms [25,27]. However, in the present case, we propose that an entirely different mechanism may be responsible. TTM should be considered in patients with a history of breast cancer and atypical CNS lesions, even without VHL.
Given the rarity of TTM involving non-VHL-related HGB, the accumulation of further cases is essential to clarify the underlying mechanisms. Understanding these mechanisms may not only provide insights into the pathophysiology of TTM but also help improve diagnostic and therapeutic strategies for such rare conditions.
Conclusions
We encountered a rare case of TTM in which metastatic breast cancer metastasized to HGB in the CNS unrelated to VHL disease. This case expands the spectrum of donor tumors in TTM and underscores the importance of histopathological confirmation in atypical CNS lesions. TTM involving benign brain tumors such as meningioma is rare but should be considered among the differential diagnoses during clinical practice. Further accumulation of similar cases is needed to better understand the mechanisms underlying TTM to HGB not associated with VHL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Metastatic inoculation of a meningioma by cancer cells from a bronchiogenic carcinoma Am J Pathol Fried BM 475261930 https://pubmed.ncbi.nlm.nih.gov/19969886/19969886 PMC 2007275 · pubmed ↗
- 2Tumor-to-tumor metastasis of the central nervous system Turk Neurosurg Erdogan H Aydin MV Tasdemiroglu E 1511622420142483135410.5137/1019-5149.JTN.8317-13.1 · doi ↗ · pubmed ↗
- 3Metastases to meningioma-review and meta-analysis Acta Neurochir (Wien) Turner N Kaye AH Paldor I 69970916320213338912510.1007/s 00701-020-04661-7 · doi ↗ · pubmed ↗
- 4Metastasis of carcinoma to hemangioblastoma cerebelli: case report Neurosurgery Crockard HA Barnard RO Isaacson PG 382384231988322651910.1227/00006123-198809000-00020 · doi ↗ · pubmed ↗
- 5Metastasis of a renal carcinoma to a cerebellar haemangioblastoma in a case of von Hippel-Lindau disease Neurosurg Rev Jamjoom A Kane N Nicoll J 231234151992140761310.1007/BF 00345942 · doi ↗ · pubmed ↗
- 6Metastasis of renal carcinoma to a cerebellar hemangioblastoma in a patient with von Hippel Lindau disease: a case report Br J Neurosurg Bret P Streichenberger N Guyotat J 4134161319991061657210.1080/02688699943565 · doi ↗ · pubmed ↗
- 7Metastasis of clear-cell renal carcinoma to cerebellar hemangioblastoma in von Hippel Lindau disease: rare or not investigated?Acta Neurochir (Wien) Mottolese C Stan H Giordano F Frappaz D Alexei D Streichenberger N 1059106314320011168561410.1007/s 007010170012 · doi ↗ · pubmed ↗
- 8Metastasis of renal cell carcinoma to central nervous system hemangioblastoma in two patients with von Hippel-Lindau disease Pathol Int Hamazaki S Nakashima H Matsumoto K Taguchi K Okada S 9489535120011184406810.1046/j.1440-1827.2001.01298.x · doi ↗ · pubmed ↗