Endoscopic resection of gastric cancer involving pylorus and duodenum using novel anchor ring-shaped thread counter traction
Hirohito Mori, Yasunori Yamamoto, Kazuki Niida, Masaaki Tange, Yoichi Hiasa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
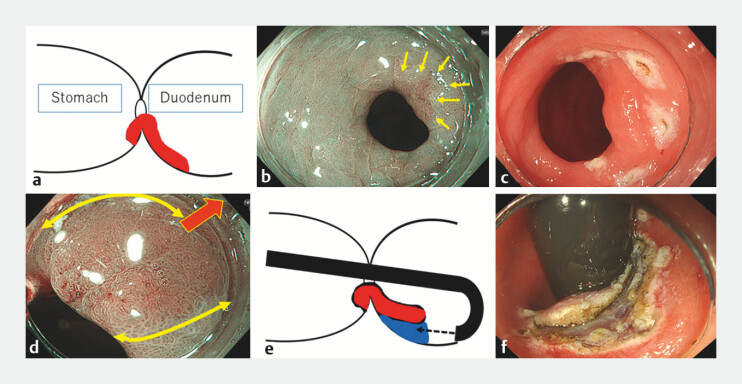 Fig. 1
Fig. 1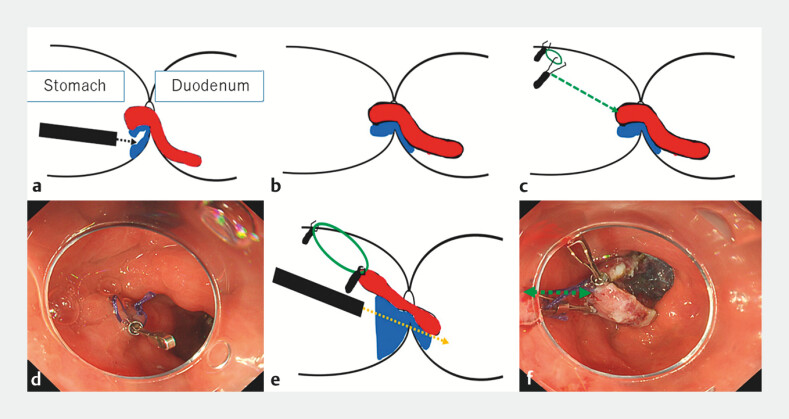 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments
As endoscopic submucosal dissection (ESD) is an established treatment for gastric cancer, it is sometimes very difficult to dissect the lesion depending on its location. Particularly, an expanding lesion from the gastric pylorus into the duodenal bulb is very difficult to perform ESD with a high risk of duodenal perforation 1 . While various traction methods have been reported 2 3 4 5 , we report a novel traction technique without interference with the endoscope.
An 81-year-old man underwent ESD for gastric cancer. The lesion was located on the posterior wall of the pylorus with the proximal part (around 5 mm in diameter) ( Fig. 1 a–c ), and most of the lesion with the distal part (15 mm in diameter) was expanded into the posterior wall of the duodenal bulb ( Video 1 ). All of the lesion was revealed by pushing up the posterior wall of the pyloric ring using an endoscopic attachment ( Fig. 1 d ). Under retroflex view within the duodenal bulb, duodenal ESD was conducted ( Fig. 1 e, f ). Although submucosal dissection was performed from the duodenal side, the lesion shifted into the duodenum, making it more difficult to dissect over the pyloric ring ( Fig. 2 a, b ). A Zeoclip (Zeon Co., Tokyo) with a 5-mm ring-shaped thread was put on the anterior wall of the antrum, opposite side of the lesion, to be used as an anchoring clip ( Fig. 2 c, d ). After another Zeoclip was used to hook the ring thread, the anchor ring-thread clip was pulled to the proximal side of the resected specimen without insufflation ( Fig. 2 e ). With insufflation, the lesion was shifted into the stomach. Submucosal dissection was safely completed under sufficient view by counter-traction ( Fig. 2 f ).
Endoscopic resection of gastric cancer involving pylorus and duodenum by anchor ring-shaped thread counter traction under retroflex view within duodenal bulb. a–c The lesion was located on the posterior wall of the pylorus, with a portion (approximately 5 mm in diameter) involving the posterior wall of the pyloric ring (yellow arrows). The majority of the lesion (around 15 mm in diameter) was observed extending into the posterior wall of the duodenal bulb. d By pressing the posterior wall outward with the endoscope attachment (red bold arrow), the majority of the lesion (around 15 mm in diameter) was observed extending into the posterior wall of the duodenal bulb (yellow curved arrows). e, f Under retroflex view within the duodenal bulb, submucosal dissection was conducted.
ESD of the gastric side was performed in the straightforward view using the anchor ring-shaped thread counter traction method. a, b After ESD of the duodenal lesion, ESD of the gastric side was performed in the straightforward view. c, d A Zeoclip with 5 mm ring-shaped thread was put on the anterior wall of the antrum, opposite side of the lesion, to be used as an anchoring clip. e After another Zeoclip was used to hook the ring thread, the anchor ring-thread clip was pulled to the proximal side of the resection specimen without insufflation. f With insufflation, the blind lesion on the posterior wall of the duodenal bulb pulled by the ring-thread was shifted into the gastric side (green arrow), allowing the remaining duodenal ESD to be easier within the stomach.
Novel anchor ring-shaped thread counter traction for obtaining a direct view of the gastric cancer hidden behind the pylorus.Video 1
The anchor ring-shaped thread counter-traction method was useful to secure the operative field when treating lesions expanding from the pylorus to the duodenal bulb. This technique was also useful for colorectal ESD by obtaining a direct view of lesions hidden behind mucosal folds.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pérez-Cuadrado-Robles E QuénéhervéL Margos WESD versus EMR in non-ampullary superficial duodenal tumors: a systematic review and meta-analysis Endosc Int Open 20186 E 998E 100710.1055/a-0579-905030083591 PMC 6075947 · doi ↗ · pubmed ↗
- 2Goda Y Mori H Kobara H Efficacy of sufficient operation view by ring-shaped thread counter traction for safer duodenal ESD Minim Invasive Ther Allied Technol 20182732733210.1080/13645706.2018.145570629764299 · doi ↗ · pubmed ↗
- 3Tashima T Miyaguchi K Tanisaka Y Successful duodenal endoscopic submucosal dissection using multiple clip-and-thread traction for a large tumor located in the duodenal bulb Video GIE 2021617818010.1016/j.vgie.2020.12.00533898896 PMC 8058531 · doi ↗ · pubmed ↗
- 4Tashima T Jinushi R Ishii N Effectiveness of clip-and-thread traction-assisted duodenal endoscopic submucosal dissection: a propensity score-matched study (with video)Gastrointest Endosc 20229591892834979111 10.1016/j.gie.2021.12.024 · doi ↗ · pubmed ↗
- 5Mori H Kobara H Nishiyama N Novel effective and repeatedly available ring-thread counter traction for safer colorectal endoscopic submucosal dissection Surg Endosc 2017313040304710.1007/s 00464-016-5326-727858210 PMC 5487838 · doi ↗ · pubmed ↗