Endoscopic ultrasound-guided gastroenterostomy through the mesh of a previous enteral stent in a patient with malignant gastric outlet obstruction and refractory ascites
Giuseppe DellʼAnna, Francesco Vito Mandarino, Jacopo Fanizza, Gabriele Altieri, Ernesto Fasulo, Silvio Danese, Gianfranco Donatelli

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
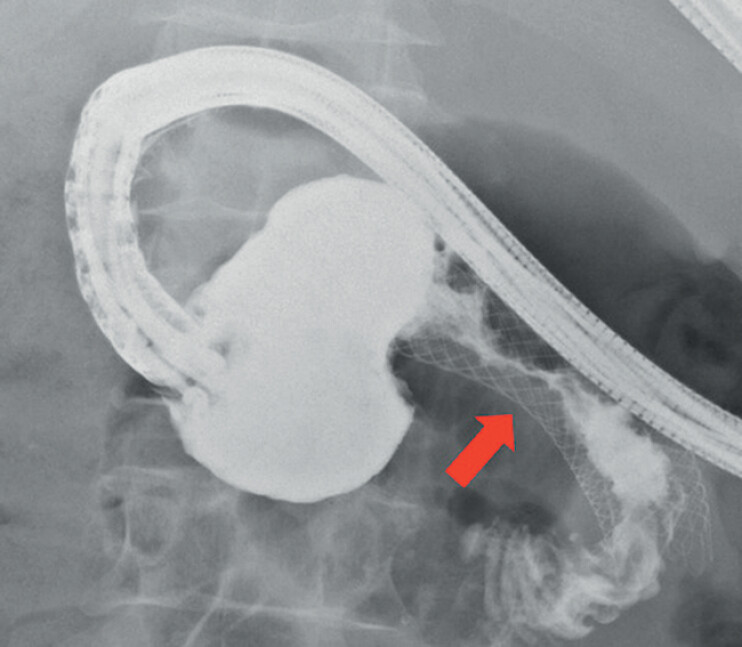 Fig. 1
Fig. 1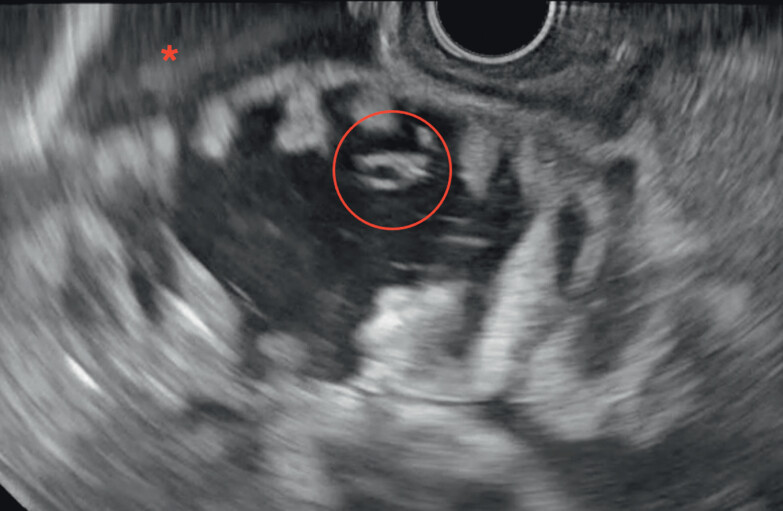 Fig. 2
Fig. 2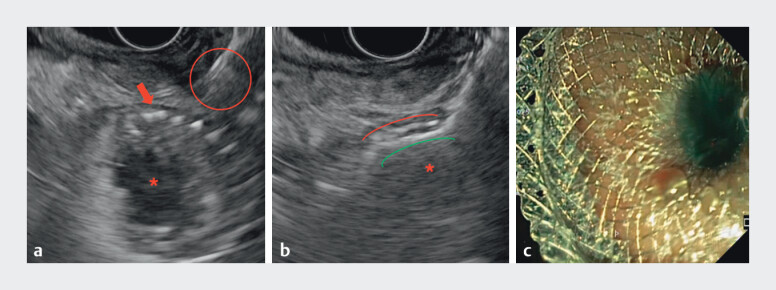 Fig. 3
Fig. 3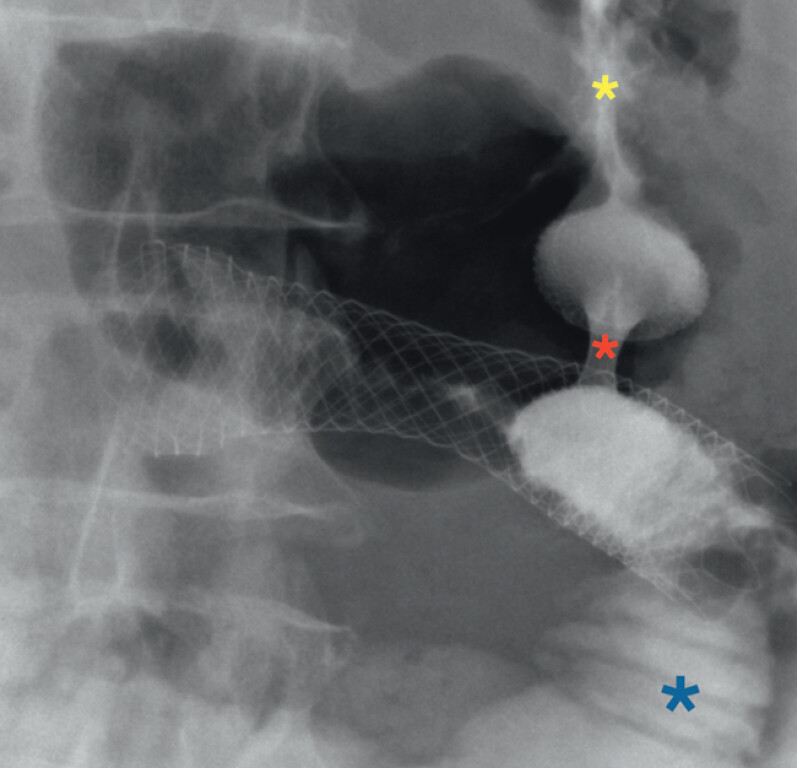 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Gastrointestinal disorders and treatments
Endoscopic ultrasound-guided gastroenterostomy (EUS-GE) is the preferred treatment for malignant gastric outlet obstruction (mGOO) due to its minimally invasive nature and superior long-term efficacy over surgery and enteral stenting (ES). However, massive malignant ascites may constitute technical contraindications to EUS-GE 1 2 3 4 . We treated a 74-year-old man with metastatic pancreatic body adenocarcinoma infiltrating the third duodenal portion 3 months early, who underwent 22 mm × 90 mm ES (Walflex, Boston Scientific, USA) placement in another center and was referred for recurrent mGOO, which led to chemotherapy (CT) interruption. A computed tomography scan revealed massive ascites, refractory to percutaneous drainage. After a multidisciplinary discussion, EUS-GE, according to the wireless simplified technique, was proposed 5 ( Video 1 ). The endoscopic evaluation confirmed ES obstruction due to tissue ingrowth ( Fig. 1 ). During EUS, the first jejunal and adjacent loops, containing the nasogastric tube and distended by the solution, were seen floating in the ascites ( Fig. 2 ). Consequently, under EUS guidance and following the ES, an optimal window for EUS-GE was identified at its distal flange. Under EUS and fluoroscopic guidance, a 20-mm × 10-mm lumen apposing metal stent (LAMS; Hot Axios, Boston Scientific, USA) electrocautery catheter was advanced and deployed through the ES mesh, allowing the immediate intragastric flow of the blue-dyed solution ( Fig. 3 ). The patient was discharged on postoperative day 1 after restarting regular oral feeding the same day. The 2-week scheduled endoscopic control confirmed full LAMS expansion and contrast medium flow from the stomach through the LAMS to the duodenum downstream of the ES distal flange ( Fig. 4 ). After 3 months, the patient remains asymptomatic and continues CT. Although massive ascites is a contraindication to EUS-GE, this case demonstrates its feasibility in expert hands through the mesh of a previously placed ES. In a similar setting, the ES terminal portion could act as a landmark and fixation point, minimizing misdeployment risk while effectively bypassing the stenotic segment 4 .
Endoscopic ultrasound-guided gastroenterostomy through the mesh of the enteral stent.Video 1
Serrated stenosis (red arrow) of the middle portion of the enteral stent due to tissue ingrowth.
The first jejunal and adjacent loops distended with the oro-jejunal tube inside (red circle), floating in the ascites (red asterisk).
a Endoscopic ultrasound (EUS) view of the enteral stent (ES) lumen (red asterisk) and mesh (red flag) with the electrocautery-enhanced tip of the lumen apposing metal stent (ec-LAMS) (red circle). b EUS view of the release of the distal flange of the ec-LAMS (green line) inside the ES (red line) lumen (red asterisk). c Endoscopic view of the intragastric release of the proximal flange of the ec-LAMS with blue solution flow.
The fluoroscopic view of the contrast medium flows from the gastric lumen (yellow asterisk), through the lumen apposing metal stent lumen (red asterisk) into the first jejunal loop lumen (blue asterisk).
Endoscopy_UCTN_Code_TTT_1AS_2AK
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Der Merwe S Wvan Wanrooij RLJ Bronswijk M Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225418520510.1055/a-1717-139134937098 · doi ↗ · pubmed ↗
- 2Kumar A Chandan S Mohan SEUS-guided gastroenterostomy versus surgical gastroenterostomy for the management of gastric outlet obstruction: a systematic review and meta-analysis Endosc Int Open 202210 E 448E 45810.1055/a-1765-403535433208 PMC 9010090 · doi ↗ · pubmed ↗
- 3Teoh AYB Lakhtakia S Tarantino I Endoscopic ultrasonography-guided gastroenterostomy versus uncovered duodenal metal stenting for unresectable malignant gastric outlet obstruction (DRA-GOO): a multicentre randomised controlled trial Lancet Gastroenterol Hepatol 2024912413210.1016/S 2468-1253(23)00242-X 38061378 · doi ↗ · pubmed ↗
- 4Basha J Lakhtakia S Yarlagadda R Gastric outlet obstruction with ascites: EUS-guided gastro-enterostomy is feasible Endosc Int Open 20219 E 1918 E 192310.1055/a-1642-789234917463 PMC 8670992 · doi ↗ · pubmed ↗
- 5van Wanrooij RLJ Bronswijk M Kunda R Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Technical Review Endoscopy 20225431033210.1055/a-1738-678035114696 · doi ↗ · pubmed ↗