Submucosal abscess at the esophagogastric junction successfully treated by endoscopic submucosal dissection: A rare case report
Lihua Guo, Jiaxin Ge, Jinfeng Wen, Lijiang Huang, Fang Huang, Mengpei Zhang, Guo-Liang Ye

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
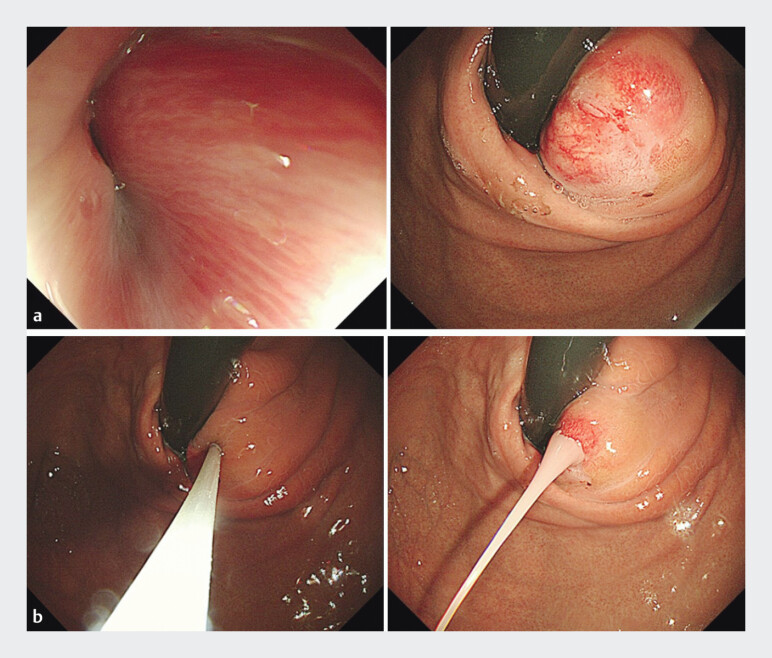 Fig. 1
Fig. 1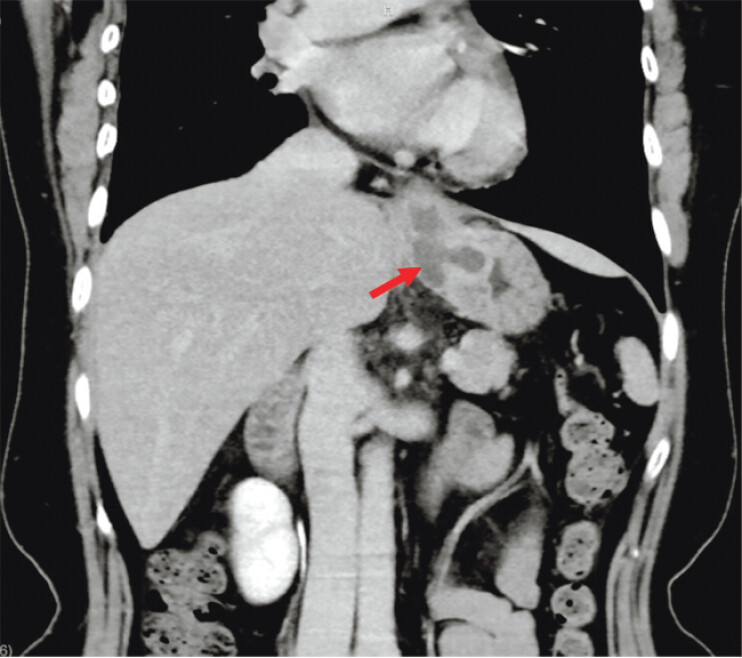 Fig. 2
Fig. 2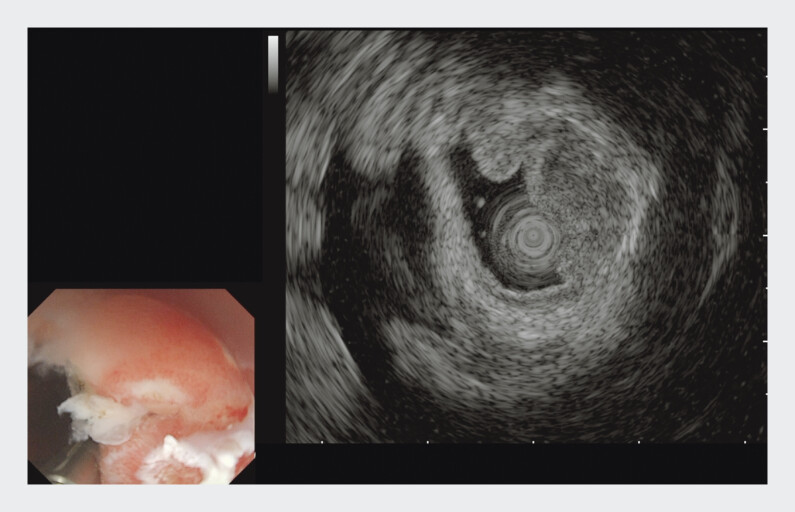 Fig. 3
Fig. 3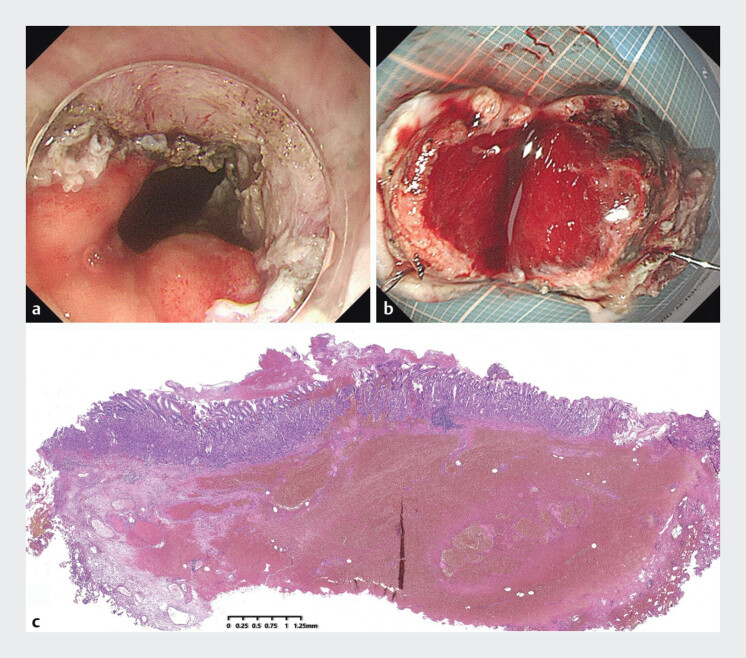 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Eosinophilic Esophagitis · Gastric Cancer Management and Outcomes
A 53-year-old woman was admitted to the hospital two days ago presenting with fever, upper abdominal pain, and dysphagia. Six months ago, she was admitted to the local hospital, where a gastroscopy revealed a submucosal abscess of the esophagogastric junction ( Video 1 ). Following endoscopic needle aspiration for pus drainage, her condition improved ( Fig. 1 ). Two days ago, her aforementioned symptoms recurred and worsened, accompanied by a fever with a peak temperature of 38.1 °C. The laboratory tests indicated an elevated inflammatory response.
Endoscopic submucosal dissection successfully treated a submucosal abscess at the esophagogastric junction.Video 1
a Endoscopic examination revealed a submucosal abscess at the esophagogastric junction. b Fine-needle aspiration was conducted to promote effective drainage.
A contrast-enhanced computed tomography (CT) scan of the abdomen revealed thickening of the lower esophagogastric wall along with a low-density focus, which may indicate the potential formation of an abscess ( Fig. 2 ). Antibiotic therapy was initiated with 2 g cefoperazone-sulbactam every 8 hours (intravenous drip). White-light endoscopy revealed a mucosal bulge in the esophagogastric junction. Endoscopic ultrasonography (EUS) revealed a submucosal hypoechoic mass measuring approximately 13 mm in diameter, with the muscular layer integrity remaining intact ( Fig. 3 ). The patient then underwent endoscopic submucosal dissection (ESD) of the suspected abscess. The excised lesion specimens from the wound were fixed with pins and subsequently sent for pathological examination. The patient was discharged with no further symptoms after 5 days of treatment. Pathology revealed a suppurative inflammation and reactive changes in focal squamous epithelium ( Fig. 4 ). On follow-up endoscopy three months later, there was healing mucosa without submucosal lesions.
Contrast-enhanced computed tomography of the abdomen with coronal reconstruction demonstrated wall thickening at the esophagogastric junction and the potential formation of an abscess (red arrow).
Endoscopic ultrasound revealed a suspected abscess at the esophagogastric junction.
a The lesion was completely removed. b A hematoma was observed following incision of the lesion. c The pathological findings indicated the presence of purulent inflammation with hemorrhage.
The formation of a submucosal abscess in the esophagus or stomach is typically associated with foreign bodies or a condition of iatrogenic etiology 1 2 . Prompt diagnosis and early therapy are needed to prevent death and prolonged serious illness; the key to diagnosis is an awareness of frequent atypical presentations 3 . The results showed that endoscopic puncture and drainage of esophagogastric junction abscesses could only temporarily relieve the symptoms, while ESD could cure submucosal abscesses of the esophagogastric junction.
Endoscopy_UCTN_Code_TTT_1AO_2AN
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
Endoscopy_UCTN_Code_CCL_1AB_2AD_3AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Onana Ndong P Piche T Vanbiervliet G Comprehensive endoscopic management of recurrent esophageal wall abscess revealing concomitant eosinophilic esophagitis Endoscopy 202456 E 510E 51110.1055/a-2325-277038866058 PMC 11168795 · doi ↗ · pubmed ↗
- 2Wang P Liu F Endoscopic treatment of esophageal intramural abscess caused by embedded metal clip: a rare delayed complication of endoscopic submucosal dissection Endoscopy 201850 E 134E 13510.1055/a-0584-632329566401 · doi ↗ · pubmed ↗
- 3Zhang J Wang H Liu D Treatment of a spontaneous intramural esophageal abscess by endoscopic mucosal incision: an easy and effective therapy Endoscopy 202254 E 937E 93810.1055/a-1882-542235835156 PMC 9736806 · doi ↗ · pubmed ↗