Recombinant Human GH in Managing Refractory Hypoglycemia in a Young Patient With Embryonal Rhabdomyosarcoma
Aditya V Belamkar, Viral N Shah, Palak Patadia, Avery Abfall, Adelina Priscu

TL;DR
A young patient with a rare tumor and severe hypoglycemia was successfully treated with recombinant human growth hormone.
Contribution
Demonstrates the potential use of rhGH in managing hypoglycemia in non-resectable tumors with atypical IGF-2/IGF-1 ratios.
Findings
rhGH treatment resolved hypoglycemia in a patient with embryonal rhabdomyosarcoma and NICTH.
The IGF-2/IGF-1 ratio was 3.6, below the classic threshold but still indicative of IGF-2-mediated hypoglycemia.
rhGH allowed for tapering of corticosteroids and dextrose fluids without recurrence of hypoglycemia.
Abstract
Non-islet cell tumor hypoglycemia (NICTH) is a rare paraneoplastic syndrome associated with various malignancies, mediated by the overproduction of IGF-2. We describe a 24-year-old male with metastatic embryonal rhabdomyosarcoma who presented with severe symptomatic hypoglycemia. Workup confirmed suppressed insulin and ketone levels, with an IGF-2/IGF-1 ratio of 3.6 (<3). Hypoglycemia was initially managed with corticosteroids and dextrose-containing fluids without success. Since surgical debulking was not feasible due to tumor burden, recombinant human GH (rhGH) was considered. Somatropin was initiated at 1 mg daily and uptitrated to 2 mg daily over 2 days, resulting in resolution of hypoglycemia with progressive tapering of dextrose-containing fluids and steroid doses. He was discharged on rhGH 2.7 mg daily with no further hypoglycemic episodes. This case highlights the challenges of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
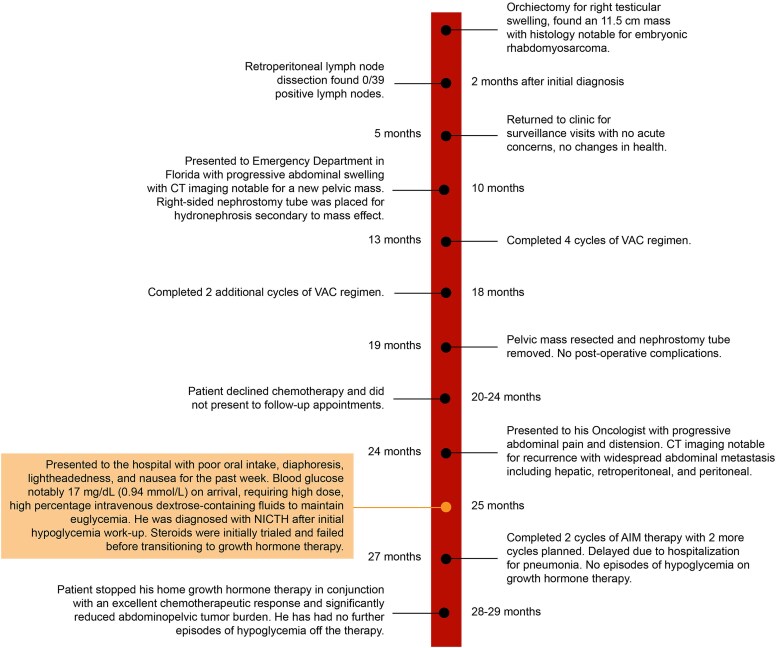 Figure 1
Figure 1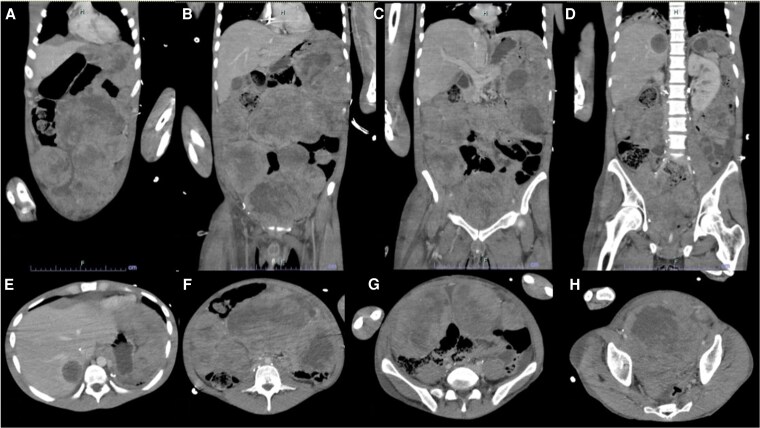 Figure 2
Figure 2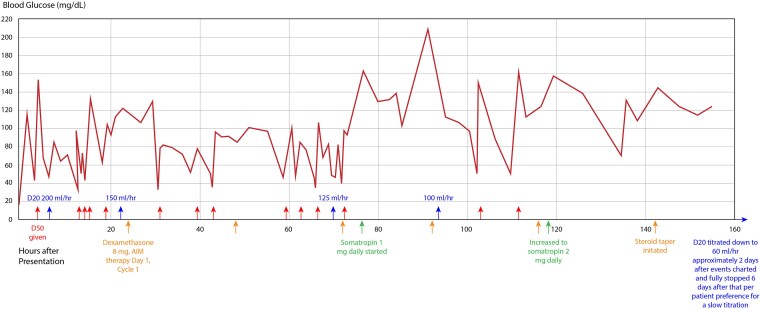 Figure 3
Figure 3| Lab | Result | Reference range |
|---|---|---|
| Serum glucose | 30 mg/dL (SI: 1.67 mmol/L) | 70-100 mg/dL [SI: 3.89-5.55 mmol/L] |
| Insulin | 0.50 μU/mL (SI: 3.47 pmol/L) | 4.00-30.00 μU/mL [SI: 27.78-208.35 pmol/L] |
| Proinsulin | <2.0 pmol/L (SI: <2.0 pmol/L) | ≤7.2 pmol/L [SI: ≤7.2 pmol/L] |
| C-peptide | 0.1 ng/mL (SI: 0.03 nmol/L) | 1.1-4.4 ng/mL [SI: 0.36-1.46 nmol/L] |
| Insulin antibody | <0.4 units/mL (SI: <0.4 units/mL) | 0.0-0.4 units/mL [SI: 0.00-0.40 units/mL] |
| Sulfonylurea panel | Negative | |
| β-hydroxybutyrate | 0.04 mmol/L (SI: 0.04 mmol/L) | 0.02-0.27 mmol/L [SI: 0.02-0.27 mmol/L] |
| TSH | 4.850 μU/mL (SI: 4.85 μU/mL) | 0.400-4.200 μU/mL [SI: 0.40-4.20 μU/mL] |
| Free T4 | 1.1 ng/dL (SI: 14.16 pmol/L) | 0.6-1.5 ng/dL [SI: 7.72-19.30 pmol/L] |
| Cortisol (8 | 12.3 μg/dL (SI: 339.36 nmol/L) | 8-25 μg/dL [SI: 220.72-689.75 nmol/L] |
| Cortisol (4 | 16.2 μg/dL (SI: 446.96 nmol/L) | 4-20 μg/dL [SI: 110.36-551.80 nmol/L] |
| ACTH | 6.7 pg/mL (SI: 1.48 pmol/L) | 7.2-63.0 pg/mL [SI: 1.59-13.87 pmol/L] |
| IGF-1 | 45 ng/mL (SI: 5.90 nmol/L) | 155-432 ng/mL [SI: 20.30-56.59 nmol/L] |
| IGF-2 | 162 ng/mL (SI: 21.22 nmol/L) | 180-580 ng/mL [SI: 23.58-75.98 nmol/L] |
| IGF-2/IGF-1 ratio | 3.6 | <10 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
|
| 83 yo F | Retroperitoneal fibrous tumor | Hypoglycemic coma, 3-month history of symptomatic hypoglycemia | Human GH 4 units in the morning, 6 units in the evening | Improved glucose, insulin, C-peptide, IGF-1; decreased IGF-2 after 2 months of therapy | Patient passed during debulking surgery |
|
| 2 yo F | Neuroblastoma | Hypoglycemic seizures | GH 0.05 mg/kg titrated up to 0.2 mg/kg divided into 2 doses | Improved glucose, IGF-1, IGFBP-3; decreased IV dextrose requirement, IGF-2 | Changes maintained after 6 months of GH therapy |
|
| 67 yo F | Pleural fibroma | Hypoglycemia requiring glucose infusion and regular oral carbohydrate intake | 3 phases: maintenance therapy of prednisone 10 mg, and rhGH 1.3 mg daily | Improved glucose, insulin, C-peptide, GH, IGF-1, IGFBP-3 | Patient had no hypoglycemic episodes 6 months after initiating treatment at which she passed from respiratory failure related to NICTH |
|
| 61 yo F | Gastrointestinal stromal tumor | Refractory symptomatic hypoglycemia for 4 months | GH 1 mg/day | Resolved hypoglycemia | Long-term outcomes not reported |
|
| 74 yo F | Inconclusive histology, suspect solitary fibrous tumor of the pleura | Neuroglycopenia | Subcutaneous rhGH 2 units nightly, oral prednisolone 30 mg daily, bendrofluazide 5 mg daily | Octreotide failed initially in controlling hypoglycemia, but switching to prednisolone abolished these events; notable reduction in IGF-2; restoration of insulin secretion | Prednisolone dose was reduced to 15 mg daily without further episodes of hypoglycemia; patient lived independently for 9 months at home before passing suddenly of unknown causes |
|
| 80 yo F | Medullary thyroid cancer | Severe, protracted fasting hypoglycemia | hGH: 12 units days 1 and 2, 24 units day 3, 36 units day 4 | hGH therapy increased glucose; no effect on insulin production, increased IGF-1; variable effect on IGF-2; increased IGFBP-3 | |
| 83 yo F | Pleural fibroma | hGH: 4 units daily for 4 days, 8 units daily for 11 days, 12 units daily for 3 days | ||||
| 64 yo M | Hepatoma | hGH: 6 units daily for 27 days | ||||
| 69 yo F | Lung carcinoma | hGH: 4 units daily for 3 days, 10 units daily for 2 days, 12 units daily for 2 days, 24 units daily for 7 days | ||||
| 30 yo M | Hemangiopericytoma | Dexamethasone: 4 mg thrice daily for 3 months, 4 mg twice daily for 4 months | Glucocorticoid therapy increased glucose, insulin production, IGF-1, IGFBP-3 and decreased IGF-2 | |||
| 92 yo F | Pleural fibroma | Prednisolone: 30 mg daily for 6 weeks | ||||
| 74 yo F | Pleural fibroma | Prednisolone: 30 mg daily for 4 months | ||||
| 81 yo F | Lung carcinoma | Prednisolone: 30 mg daily for 4 months | ||||
|
| 74 yo M | Hemangiopericytoma | Neuroglycopenic symptoms of confusion and lightheadedness | Initially trialed dexamethasone at 1 mg orally twice daily and uptitrated to 2 mg twice daily, which had limited efficacy; weaned dexamethasone to 1 mg twice daily and added rhGH 0.45 units daily | Resolution of hypoglycemia, increase in IGF-1 and IGFBP-3, and reduction of IGF-2 | Improved quality of life for many months without hypoglycemia |
|
| 27 yo F | Ovarian yolk sac tumor | Symptomatic hypoglycemia, passed out | Trialed dexamethasone at 4 mg twice daily and uptitrated to 16 mg twice daily to prevent recurrence of hypoglycemia; however, due to recurrence of symptoms, rhGH 0.4 units/kg/day was initiated allowing dexamethasone to be titrated down | Maintained normoglycemia | Therapy allowed patient to travel to her home country where she passed away with her family after a few days |
|
| 75 yo M | Leydig cell tumor | Found unconscious, severely hypoglycemic | Initially treated with IV D10 and dexamethasone 2 mg 4 times daily but was unable to come off the IV D10; he was started on rhGH 8 units that increased to 32 units daily, allowing for the dextrose infusion to be stopped gradually | Had no more hypoglycemic episodes | Opted for conservative approach; passed away 10 days after admission due to deteriorating renal function |
|
| 46 yo F | Renal cell carcinoma | Confusion and expressive dysphagia, hypoglycemic | Started on diazoxide 100 mg thrice daily with continued symptomatic nocturnal hypoglycemia; added cornstarch at night without improvement; subsequently prednisolone 20 mg was added with symptomatic improvement; however, this lasted only 10 days before another episode of severe symptomatic hypoglycemia, prompting the addition of bendrofluazide 5 mg daily and GH 2 units nightly | Symptoms did not improve on GH and patient was switched to octreotide 100 units nightly and increased prednisolone to 40 mg daily | Patient continued to have symptomatic hypoglycemia and trialed a variety of carbohydrate administration; after 1 month her condition deteriorated and patient passed away |
|
| 64 yo M | Hepatoma | Unconscious; found to be hypoglycemic | Initially trialed high-calorie diet, followed by GH 2 units daily, GH was uptitrated to 2 units thrice daily | Even with uptitration, octreotide 50 micrograms was added without benefit, leading to administration of IV dextrose for discharge | Remained free from hypoglycemia for 24 months after his initial presentation before subsequently passing away |
|
| 65 yo M | Benign pleural tumor | Acute confusional state resulting from hypoglycemia | rhGH 6 units daily | Increased mean plasma glucose, IGF-1, IGFBP-3 | Attempted debulking surgery; patient developed pneumonia and died on postoperative day 12 |
| 54 yo M | Pleural fibrosarcoma | Not arousable and sweating due to hypoglycemia | Hypoglycemia worsened by octreotide 100 mcg; rhGH 8 units daily successfully alleviated hypoglycemia | Increased mean plasma glucose, IGF-1, and IGFBP-3 | Prevented hypoglycemia for 5 months after initially starting rhGH before development of respiratory failure and recurrent hypoglycemia requiring 12 units daily; passed away at this time due to respiratory failure | |
|
| 2 yo F | Neuroblastoma | Hypoglycemic seizure | GH 0.2 mg/kg/day twice daily | Alleviated hypoglycemia; able to fast 12 hours without hypoglycemia | Discharged and after 5 months decreased GH to 0.1 mg/kg/day twice daily; maintained on this treatment for 1 year without side effects and improved growth |
|
| 43 yo M | Adrenocortical carcinoma | Severe nonketotic, noninsulin-mediated hypoglycemia, also ACTH-dependent Cushing's syndrome | rhGH 3 mg/daily, increased to 4 mg/daily | Significant reduction of severity and frequency of hypoglycemia | Opted for palliative chemotherapy; however, passed away due to illness while receiving this treatment |
|
| 56 yo F | Pleural mesothelioma | Confusion, diaphoresis, weakness | Trialed prednisone 30 mg uptitrated to 100 mg daily without success as well as adding diazoxide; successful treatment occurred with dexamethasone 16 mg/day and rhGH 2.65 mg/day | Stabilization of average blood glucose level with range within normal limits | Died due to complications related to mesothelioma week after starting final therapy; no further episodes of hypoglycemia |
|
| 28 yo F | Solitary fibrous tumor | Unresponsive with severe hypoglycemia | Complete tumor resection and retroperitoneal lymph node dissection | Symptoms resolved after resection | Euglycemic with no evidence of tumor recurrence 1 year after surgery |
| 54 yo F | Hemangiopericytoma | 2-week history of intermittent confusion, decreased responsiveness, and speech difficulty occurring overnight while fasting | Steroids resulted in psychiatric adverse effects, no improvement with octreotide 100 mcg, switched to rhGH 0.67 mg daily and titrated up to 1.67 mg daily in combination with dexamethasone 1 mg daily | Prevented nocturnal hypoglycemia and allowed for dextrose to be discontinued | Hypoglycemia was prevented with rhGH and low-dose dexamethasone; passed away 6 months later under palliative care | |
|
| 70 yo F | Gastrointestinal stromal tumor | Left-sided vasomotor symptoms including reduced muscle tone, weakness, and slurring of speech, progressive over past 3 months | Diazoxide failed initially, prednisolone 20 mg daily was successful in controlling symptoms and weaning IV dextrose; however, to minimize steroid side effects, rhGH was added with tapering of prednisolone dosing | Prevented hypoglycemic episodes; symptoms resolved | Imatinib significantly improved symptoms as well as tumor burden and allowed for rhGH to be discontinued; patient is doing well 8 years following diagnosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Growth Hormone and Insulin-like Growth Factors · Hyperglycemia and glycemic control in critically ill and hospitalized patients
Introduction
Non-islet cell tumor hypoglycemia (NICTH) is a rare phenomenon associated with various malignancies. This process is mediated through IGF-2, which, in normal physiology acts as a minor growth factor with a secondary role to IGF-1 [1]. IGF-1 is typically regulated by the hypothalamus-pituitary axis mediated by GH, while IGF-2 is not normally responsive to GH [2]. However, in NICTH, IGF-2 is grossly overexpressed by tumor cells, especially of mesenchymal and epithelial origin, exerting an insulin-like effect on the body, promoting hypoglycemia by binding both IGF receptors and insulin receptors. The pathophysiology of NICTH is centered on overproduction of IGF-2 with suppression of both insulin and IGF-1 [3, 4]. The interaction between IGF and insulin signaling pathways and their role in cancer progression has been previously documented [2]. This often presents as symptomatic fasting hypoglycemia, endogenous insulin and ketones suppression, and an elevated IGF-2/IGF-1 ratio. Other mechanisms of malignant hypoglycemia include wasting due to deficiency of gluconeogenic precursors and overconsumption of glucose by the tumor, often in the setting of hepatic glycogen depletion [5]. Overall, treatment of this condition is centered around reducing tumor burden, providing high carbohydrate nutrition, and medical management. These have been described with varying efficacy in the literature; however, the data is limited due to the scarcity of cases and limited long-term prognosis of many of these patients. In this case, we describe a young man with new-onset hypoglycemia in the setting of progressive, metastatic malignant disease necessitating trial of rhGH.
Case Presentation
A 24-year-old male with a prior diagnosis of metastatic embryonal rhabdomyosarcoma complicated by deep vein thrombosis and atrial thrombi managed with aspiration thrombectomy, apixaban, and an inferior vena cava filter and a history of gunshot wounds to the chest and abdomen presented with diffuse abdominal pain and altered mental status. His malignancy was diagnosed 3 years earlier following an orchiectomy for testicular swelling, with pathology of the 11.5 cm mass confirming a diagnosis of embryonal rhabdomyosarcoma (Fig. 1). He had 6 cycles of vincristine, dactinomycin, and cyclophosphamide, achieving initial oncologic improvement. However, his disease course was complicated by pelvic recurrence 2½ years after diagnosis and 4 months prior to his current presentation, requiring percutaneous nephrostomy tube placement, surgical resection, and retroperitoneal lymph node dissection. He subsequently declined additional chemotherapy and missed multiple follow-up appointments. Imaging 3 months postresection revealed widespread abdominal recurrence, including hepatic metastases. At this time, he was scheduled to begin additional chemotherapy, but prior to this, he presented to the hospital reporting progressive diffuse abdominal pain, 20-pound weight loss over 3 months, difficulty urinating, and altered mental status. He presented with a weight of 51.9 kg (<5th percentile for race and age) and a body mass index of 15.5 (<5th percentile), which was a significant downtrend from weights ranging in the 5th to 10th percentile in the past 6 months.
Timeline of patient's oncologic history.
On admission, the patient was hemodynamically stable but hypothermic to 34.3 °C and severely hypoglycemic (17 mg/dL (SI: 0.94 mmol/L) (reference range, 70-100 mg/dL [SI: 3.89-5.55 mmol/L]) with loss of consciousness. He had no prior history of diabetes or hypoglycemia. Abdominal and pelvic computed tomography demonstrated extensive, heterogeneously enhancing masses consistent with progressive malignant disease, moderate right-sided hydronephrosis due to mass effect, and progressive hepatic lesions consistent with prior noted metastases (Fig. 2A-2B). Persistent hypoglycemia required dextrose 50% IV pushes and dextrose 20% IV fluid at 200 mL/hour (12.85 mg/kg/min), prompting endocrinology consultation. Figure 3 describes his glycemic course including hypoglycemic management within the first 160 hours following presentation. Pertinently, he reported experiencing diaphoresis, nausea, and confusion associated with low blood glucose, which improved with glucose treatment. He endorsed social alcohol consumption and recreational marijuana use. His appetite was recently diminished due to abdominal pain and constipation, but he consumed 2 to 3 protein shakes daily along with occasional solid foods.
(A-H) Abdomen and pelvis computed tomography from presentation notable for significant abdominopelvic and hepatic lesions consistent with known metastatic embryonal rhabdomyosarcoma. There is also moderate right renal hydronephrosis due to mass effect that did not require decompression.
Glycemic course over the initial 160 hours following presentation including hypoglycemic events and glycemic medication and fluid treatments. Abbreviations: D20, dextrose 20%; D50, dextrose 50%; IAM, doxorubicin, ifosfamide, and mesna therapy.
Diagnostic Assessment
As the patient met criteria for Whipple triad, guideline-directed workup was initiated [6, 7]. Table 1 details notable lab work performed after pausing dextrose-containing fluids. The IGF-2/IGF-1 ratio was calculated to be 3.6, which did not align with the typical pattern of IGF-2-mediated hypoglycemia, where this ratio is expected to be greater than 10. However, it is important to note the normal ratio is 3, and IGF-1 was suppressed (Table 1) [4]. He had no evidence of renal failure even in the setting of hydronephrosis, therefore, IGF binding protein 3 level was not measured. A glucagon stimulation test was not conducted due to the significant drop in glucose.
Treatment
Given his extensive disease burden, debulking surgery and enteral feeding interventions were not feasible. Total parenteral nutrition was not considered due to the higher risk for infection associated with planned chemotherapy. A literature review identified potential management options, including corticosteroids, rhGH, and somatostatin analogs. The patient was already receiving IV dexamethasone 8 mg (prednisone equivalent 53.3 mg) daily per oncology chemotherapeutic protocols in addition to IV dextrose 20% fluids at rates between 150 and 200 mL/hour (9.63-12.85 mg/kg/min) without improvement in his hypoglycemia (Fig. 3). He was initiated on subcutaneous somatropin 1 mg, with subsequent titration to 2 mg daily, which allowed for slow tapering of IV dextrose fluids over 12 days and weaning off corticosteroids (Fig. 3). The patient experienced a cessation of hypoglycemic episodes with this uptitration.
Outcome and Follow-up
He was discharged on somatropin 2.7 mg subcutaneously after a 37-day hospital course including 2 cycles of doxorubicin, ifosfamide, and mesna chemotherapy. He continued to be free of hypoglycemic episodes 3 months after starting this therapy, at which point he discontinued it in conjunction with computed tomography imaging evidence of a significant decrease in abdominopelvic tumor burden, demonstrating excellent response to chemotherapy. His weight improved to 52.3 kg (<5th percentile) at the time of discontinuation and further trended up to 56.2 kg (<5th percentile) in the subsequent months. He is scheduled for surgical resection of the remaining tumor burden in the near future. Notably, he has not had any hypoglycemic episodes since discontinuing therapy. Unfortunately, as he independently discontinued treatment and had a challenging early oncologic course, follow-up IGF levels were not obtained during therapy. Once off therapy, further testing was deemed an unjustified use of resources given his clinical status.
Discussion
This case describes a new-onset hypoglycemia in the setting of significant abdominopelvic tumor burden with hepatic metastases managed with somatropin after failing corticosteroids and IV dextrose-containing fluids. Differential diagnosis of hypoglycemia in patients without diabetes includes insulinoma, noninsulinoma pancreatogenous hypoglycemia, postbariatric hypoglycemia, insulin autoimmune hypoglycemia, and insulin secretagogue pathways. Alternative diagnoses including infection, poor nutritional intake, and hepatic failure were considered. In this case, the diagnosis of NICTH was complicated by an IGF-2/IGF-1 ratio less than 10 but above normal limits. The overall workup correlated with the clinical picture of IGF-2-mediated hypoglycemia with suppressed insulin, C-peptide, and proinsulin with a serum glucose less than 55 (Table 1) [6, 7]. Most importantly, ketone production was suppressed, indicating activation of insulin-mediated pathways in the setting of appropriate insulin suppression, likely through IGF-2 mediation. Ketones would be expected to be elevated if this was a non-insulin, non-IGF-mediated pathway [6]. As a result, we hypothesize the laboratory assay may not appropriately detect high molecular weight IGF-2 that is most commonly expressed by tumor cells [7]. Another possibility is steroid administration prior to blood draws may have suppressed IGF-2 production [4, 8]. Finally, this may be multifactorial secondary to above normal IGF-2 production, reduced hepatic glycogen stores, and gluconeogenesis in the setting of metastases and poor nutrition, and excessive consumption from significant abdominopelvic tumor metabolic burden.
Diazoxide was not appropriate for this patient's hypoglycemia as initial laboratory data indicated suppression of endogenous insulin as well as concern that his blood pressures would not tolerate diazoxide-mediated vasodilation. Similarly, somatostatin analogs were not considered as these primarily suppress insulin secretion. Given the patient's clinical picture, oncology was in agreement with a trial of rhGH, acknowledging the risk for tumor growth being outweighed by the benefits of preventing hypoglycemia.
The consensus for managing NICTH is for initial IV dextrose management via central venous catheter, followed by surgical resection, and finally medical management [5]. Studies suggest glucagon infusion, corticosteroids, rhGH, and somatostatin analogs as potential options. A recent systematic review looking at 172 studies, primarily case reports, included 233 patients with NICTH. Surgical resection was the most common initial treatment modality, performed in 47.2% of patients [9]. Embolization and radiotherapy were both used in 6% of cases [9]. Corticosteroids were the most frequently administered first-line medical therapy (39.1%), followed by octreotide (7.7%) and diazoxide (6.9%) [9]. No patients in the study received rhGH [9]. Importantly, the study noted only those patients who received surgical intervention had significantly improved odds of recovering, while those who received corticosteroids or octreotide were significantly less likely to improve [9]. Presumably the patients who did not undergo surgical interventions were more complex and poor surgical candidates. Thus, medical management of NICTH may be seen as a palliative measure. Overall, the consensus of the literature is that surgical resection, when possible, is the most effective treatment, followed by other tumor burden reduction modalities and finally medical management [10]. The Endocrine Society Clinical Practice Guidelines do not describe the management of hypoglycemia in patients without diabetes [6].
The use of rhGH has been reported in literature despite concerns regarding its potential to promote tumor growth (Table 2) [7]. The exact mechanism by which it prevents hypoglycemia remains unclear. However, it is hypothesized that at supraphysiologic doses, rhGH suppresses peripheral glucose uptake and increases IGF-1 levels, which may help normalize IGF-2 binding dynamics by promoting the formation of binary and ternary complexes [4]. Additionally, rhGH may enhance hepatic glucose production through stimulation of glycogenolysis, gluconeogenesis, and lipolysis. The literature also suggests that glucocorticoids are effective in this context by lowering IGF-2 levels and increasing IGF-1 concentrations [4].
Embryonal rhabdomyosarcoma is a rare cause of NICTH with only 1 other case being noted in a pediatric patient [27]. More common causes are fibrous tumors classically associated with Doege-Potter syndrome (53.2%), followed by nonfibrous tumors of hepatic origin (9%), hemangiopericytomas (8.5%), and mesotheliomas (4.7%) [9]. Overall, this is a rare paraneoplastic syndrome that can occur in a wide variety of malignancies.
In summary, this case report discusses a 24-year-old male with metastatic embryonal rhabdomyosarcoma that presented with new-onset symptomatic hypoglycemia requiring significant IV dextrose support. After failing corticosteroids per oncologic protocols, somatropin was started at 1 mg, then uptitrated to 2 mg, to wean the patient off IV dextrose. He was discharged on somatropin 2.7 mg daily and maintained euglycemia for 3 months in association with improvement in tumor burden with chemotherapy. The use of rhGH appears to be an effective therapy for preventing hypoglycemia in patients with high suspicion for NICTH who do not respond to other conventional therapies. While there is a theoretical possibility of tumor growth, in this limited case report, it does not appear that this risk affects the potential for chemotherapeutic reduction in tumor burden.
Learning Points
NICTH is a rare paraneoplastic syndrome classically associated with fibrous tumors but may be associated with a whole range of malignancies.Although NICTH is typically diagnosed with an IGF-2/IGF-1 ratio greater than 10, a ratio below this threshold does not exclude the diagnosis, particularly in the presence of fasting hypoglycemia with suppressed insulin and ketones, findings consistent with IGF-2 mediated effects.Somatropin represents an effective alternative to dextrose-containing fluids and corticosteroids for the prevention of hypoglycemia. However, it is important to note that patients may still respond favorably to chemotherapy, despite concerns regarding potential tumor-promoting effects.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davda R, Seddon BM. Mechanisms and management of non-islet cell tumour hypoglycaemia in gastrointestinal stromal tumour: case report and a review of published studies. Clin Oncol (R Coll Radiol). 2007;19(4):265‐268.17433971 10.1016/j.clon.2006.12.008 · doi ↗ · pubmed ↗
- 2De Marco P, Cirillo F, Vivacqua A, Malaguarnera R, Belfiore A, Maggiolini M. Novel aspects concerning the functional cross-talk between the insulin/IGF-I system and estrogen signaling in cancer cells. Front Endocrinol (Lausanne). 2015;6:30.25798130 10.3389/fendo.2015.00030 PMC 4351617 · doi ↗ · pubmed ↗
- 3Dynkevich Y, Rother KI, Whitford I, et al Tumors, IGF-2, and hypoglycemia: insights from the clinic, the laboratory, and the historical archive. Endocr Rev. 2013;34(6):798‐826.23671155 10.1210/er.2012-1033 · doi ↗ · pubmed ↗
- 4Bodnar TW, Acevedo MJ, Pietropaolo M. Management of non-islet-cell tumor hypoglycemia: a clinical review. J Clin Endocrinol Metab. 2014;99(3):713‐722.24423303 10.1210/jc.2013-3382 PMC 5393479 · doi ↗ · pubmed ↗
- 5Phillips LS, Robertson DG. Insulin-like growth factors and non-islet cell tumor hypoglycemia. Metabolism. 1993;42(9):1093‐1101.8412760 10.1016/0026-0495(93)90265-p · doi ↗ · pubmed ↗
- 6Cryer PE, Axelrod L, Grossman AB, et al Evaluation and management of adult hypoglycemic disorders: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2009;94(3):709‐728.19088155 10.1210/jc.2008-1410 · doi ↗ · pubmed ↗
- 7Kittah NE, Vella A. MANAGEMENT OF ENDOCRINE DISEASE: pathogenesis and management of hypoglycemia. Eur J Endocrinol. 2017;177(1):R 37‐R 47.28381450 10.1530/EJE-16-1062 · doi ↗ · pubmed ↗
- 8Vu A, Chik C, Kwong S. IGF-2-mediated hypoglycemia: a case series and review of the medical therapies for refractory hypoglycemia. Endocrinol Diabetes Metab Case Rep. 2024;2024(1):23-0089.10.1530/EDM-23-0089 PMC 1095905338432069 · doi ↗ · pubmed ↗