User Input in the Development of Digital Sexual Health Tools: A Scoping Review and Guidance for Tool Developers
Alicia King, Ethan Cardwell, Eric Chow, Paul Flowers, Mark Gilbert, Kath Albury

TL;DR
This review summarizes how user input is used in developing digital tools for sexual health, highlighting areas for improvement in design and impact.
Contribution
The study provides guidance for developers by analyzing methods and domains of user input in digital sexual health tool development.
Findings
Usability was the most common domain for user input, followed by satisfaction and acceptability.
User suggestions were made in three out of four projects, but changes were incorporated in less than half.
Qualitative and quantitative methods were combined to gather user feedback.
Abstract
Studies reporting the use of digital tools to promote the prevention and treatment of sexually transmitted and blood borne infections (STBBIs) have proliferated in recent years. Previous reviews highlight variability in the input sought from users in tool development, and its contribution to impact. This scoping review sought to describe approaches to seeking and utilising user input, with the goal of providing guidance for developers. Searches were conducted in MEDLINE, PsycInfo, and the Social Science Citation Index and results screened by two reviewers. The reference lists of included studies and review papers were also checked. Peer reviewed qualitative and mixed methods studies seeking user input on digital tools promoting the prevention and treatment of STBBIs, from prototyping onwards, published from after 2014 in English, were included. Reported methods and findings were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
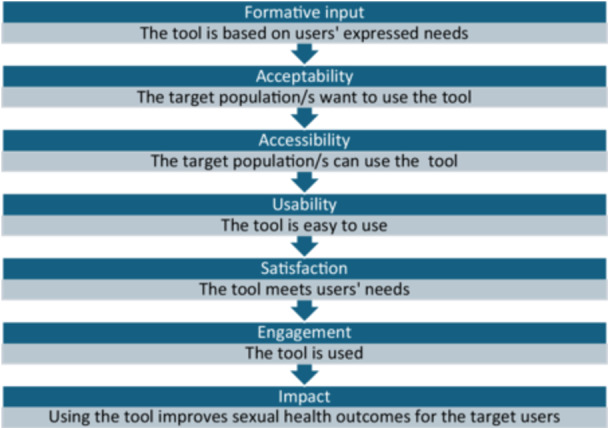 Figure 1
Figure 1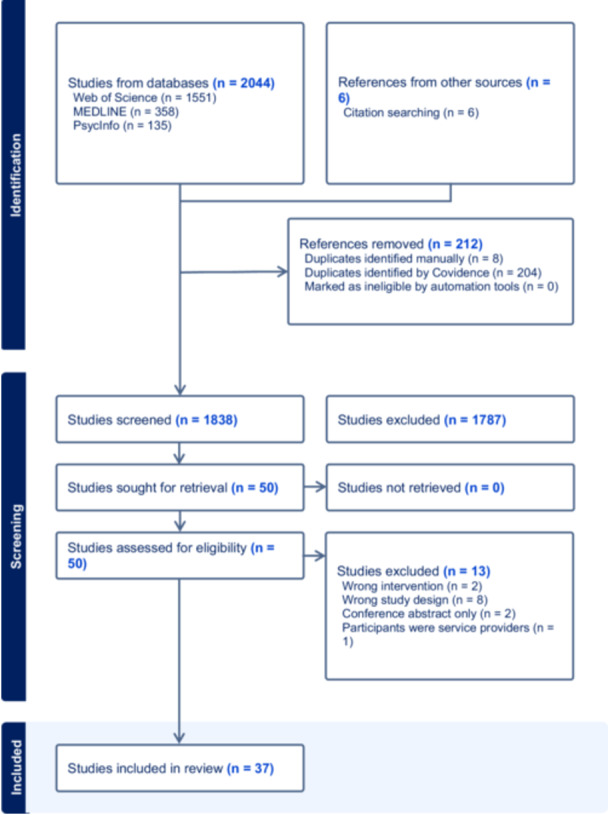 Figure 2
Figure 2| Inclusion criteria | Exclusion criteria |
|---|---|
|
Studies that sought user input on tools to promote the prevention and treatment of sexually transmitted and blood borne viruses by providing automated responses that vary based on user inputs (including prototypes of any fidelity) Qualitative or mixed methods studies Published from 2015 onwards Published in English |
Studies conducted before prototyping Clinicians or caregivers as only research participants Use of existing platforms to promote sexual health outcomes Use of tool to support ongoing engagement with care or treatment adherence of people living with HIV. Tools for use in a clinical or educational setting, except where supporting access for users without a device/internet/private space for use Studies of serious video or smartphone games and digital vending machines Grey literature (e.g., unpublished work, conference abstracts, pre‐prints of manuscripts undergoing peer review) |
| Digital health tools | STIs (including HIV) | Sexual health care and prevention | User views |
|---|---|---|---|
|
Digital health Mobile applications User‐Computer Interface |
Sexually Transmitted Diseases Sexually Transmitted Infections Sexual Transmissible Infections Chlamydia Gonorrhea Gonorrhoea HIV Syphilis Herpes HPV Papillomavirus Infections |
Sexual health Sex Education Sexual behav* Healthcare engagement Healthcare seeking ‘Patient Acceptance of Health Care’ Prevention Primary Prevention Secondary Prevention Condoms Self‐testing HIV Testing PrEP Pre‐Exposure Prophylaxis Anti‐HIV Agents Vaccinat* |
Qualitative Research User experience Patient Participation Mixed method* ‘Survey Codesign Human Centred Design Human Centred Design Universal Design Human computer interaction Participatory research Community‐Based Participatory Research |
| First author/s and year | Name of tool/s | Country | Type of tool/s used | Purpose of tool/s | Tool features and functions | Target population |
|---|---|---|---|---|---|---|
| Adeagbo, 2021 [ | EPIC‐HIV1 (Empowering People through Informed Choices for HIV) | South Africa | Smartphone or tablet application | HIV | Informed consent info presented in story about character chosen by user. | Male youth and men |
| Anderson, 2022 [ | MyPEEPS | USA | Smartphone or tablet application | HIV/STI | Educational content. | Transmasculine adolescents GBMSM |
| Bailey, 2016 [ | The Men's Safer Sex website | UK | Website or web‐based application | Promotion of condom use | Interactive educational content. | Adult men who have sex with women |
| Biello, 2021 [ | LYNX and MyChoices | USA | Smartphone or tablet application | HIV/STI self‐testing, PrEP | Ordering and delivery of HIV/STI self‐test kits and information on PrEP. | Adolescent and youth MSM |
| Braddock, 2023 [ | PrEPBot | USA | Chatbot | HIV self‐testing, PrEP access | AI ‘TelePrEP’ navigator guiding users through online PrEP prescription and delivery. | Sexual and gender minority adolescents and young adults |
| Chandler, 2020 [ | SavvyHER (Sexual/HIV Health Electronic Empowerment Resource) | USA | Smartphone or tablet application | HIV education, service navigation, STI self‐testing. peer support | Health tracking; HIV testing and PrEP clinic locator; STI self‐test, condom and sexual pleasure item ordering; multimedia resources; peer support. | PrEP eligible Black/African American women |
| Cheah, 2024 [ | Haris (chatbot) and MYHIV365 (website) | Malaysia | Chatbot | HIV education, mental health screening, service navigation | HIV self‐test ordering; MSM‐friendly clinic information; screening for depression. | MSM |
| Cordova, 2018 [ | Storytelling 4 empowerment (S4E) | USA | Smartphone or tablet application | Promotion of condom use, HIV/STI and drug use education | Educational content delivered in storytelling in format. | Adolescents and youths |
| Danielson, 2016 [ | Sistas Informing Healing Living Empowering (SiHLE Web) | USA | Website or web‐based application | HIV education | Interactive educational content. | African American adolescent girls |
| Engen, 2021 [ | SH:24 | UK | Website or web‐based application | Diagnosis and treatment of herpes and genital warts | Triage and photo diagnosis of lesions by a sexual health clinician; postal delivery of treatment; referral to in person care. | Not specified |
| Fitzpatrick, 2023 [ | PrEP EmERGE | UK | Smartphone or tablet application | PrEP management and adherence | Access to results, medication reminders, vaccination history, upcoming appointments and one way (clinic‐ user) messaging. | PrEP users |
| Gilbert, 2017 [ | GetCheckedOnline | Canada | Website or web‐based application | HIV/STI self‐testing | Risk assessment; recommendation of tests; printable pathology request. | Not specified |
| Goldenberg, 2015 [ | Not reported | USA | Smartphone or tablet application | HIV education, HIV testing promotion, service navigation and self‐monitoring. | Personalised profile; HIV testing plan; HIV testing locator; event tracker for sexual encounters and HIV testing; HIV prevention tips; interaction credits for donation to HIV/LGBT | MSM |
| Greene, 2016 [ | Keep It Up! (KIU!) | USA | Website or web‐based application | HIV education | Educational modules delivered in multimedia format (e.g., videos, animation, and games). | HIV‐negative, ethnically and racially diverse young MSM |
| Hughes, 2021 [ | Nurx | USA | Website or web‐based application | PrEP access | Counselling, prescription and home‐delivery of medication. | People wishing to access PrEP |
| Ippoliti, 2021 [ | CyberRwanda | Rwanda | Web‐based and smartphone application | SRH | Interactive behaviour change web comic series; FAQ | Adolescents |
| Janssen, 2020 [ | HIVSmart! | South Africa and Canada | Web‐based and smartphone application | HIV self‐testing support | Instructions for completing and interpreting self testing results; HIV information; post‐testing advice. | Self‐testers in Cape Town and Montreal |
| Levy, 2015 [ | Not reported | USA | Smartphone or tablet application | HIV education, service navigation | Survey to populate individualised educational content and information to support healthcare encounters. | Black MSM |
| Li, 2023 [ | Not reported | China | Social media mini app | PrEP promotion, HIV and syphilis self‐testing, health monitoring | Educational content; asynchronous messaging with clinician; HIV/syphilis self‐test ordering; HIV/syphilis testing tracker. | HIV‐negative GBMSM |
| Lindayani, 2021 [ | HIV Info Corner | Indonesia | Smartphone or tablet application | HIV education | Risk assessment; multimedia educational content; in app and email advice messages. | Adolescents |
| Liu, 2024 [ | PrEPmate and DOT Diary | USA | Interactive SMS | PrEP management and adherence |
PrEPmate: Two‐way messaging between user and HCW; medication and appointment reminders; video peer testimonials. DOTDiary: Automated DOT |
HIV‐negative, Spanish‐speaking MSM and English‐ and Spanish‐speaking transgender women |
| Mauka, 2021 [ | Jichunge | Tanzania | Smartphone or tablet application | PrEP management and adherence, HIV education | Pill‐taking diary; feedback on PrEP adherence; timed reminders; two way messaging between user and peer educators or HCP | MSM and female sex workers |
| Nadarzynski, 2021 [ | PAT | UK | Chatbot | SRH and HIV/STI education | AI responses to simple queries regarding SRH and HIV/STI prevention. | Not specified |
| Rael, 2023 [ | SMARTtest | USA | Smartphone or tablet application | HIV and syphilis self‐testing support | Instructions for completing and interpreting self testing results; information on healthcare services; image capture and interpretation. | Not specified |
| Sales, 2019 [ | SELP (Syphilis [H]ELP) | Brazil | Smartphone or tablet application | Congenital syphilis prevention; partner notification and service navigation | Multimedia educational content; health service locator; appointment scheduling; partner notification. | Men who have sex with women |
| Schaaf, 2024 [ | Communication and Tracing App HIV (COMTRAC‐HIV) | Germany | Smartphone or tablet application | PrEP (and ART) management and adherence | Symptom diary; Medications; Video‐call and messaging, including medication prescription. | PrEP and ART |
| Schnoor, 2024 [ | Directlab Online | The Netherlands | Website or web‐based application | HIV/STI self‐testing | Triage; recommendation of tests; self‐test delivery; pathology collection appointment scheduling; results; notification of deviant results to HCP. | Not specified |
| Sharma, 2022 [ | Be in the Know Zambia (BITKZ) | Zambia | Website or web‐based application | SRH education | Interactive behaviour change web comic series; visual guides; sharable SRH information; FAQs; quizzes; gamification. | Adolescents and youths |
| Sun, 2020 [ | Trans Women Connected | USA | Smartphone or tablet application | PrEP promotion, service navigation | Vision board; educational activity; interactive LGBTQ | Transgender women |
| Velloza, 2024 [ | DOT Diary | USA | Smartphone or tablet application | PrEP management and adherence | Automated DOT, information about PrEP protection levels, PrEP pill‐taking reminders, a sexual behaviour diary, and a PrEP dosing and sexual activity calendar. | Young PrEP eligible MSM |
| Visser, 2020 [ | iloveLife. mobi | South Africa | Website or web‐based application | SRH education | Interactive multimedia educational content (i.e., short articles, audio drama, quizzes, self‐assessments, discussion forums).; gamification. | Adolescents and youths |
| Widman, 2016 [ | ProjectHeartForGirls. com | USA | Website or web‐based application | Promotion of condom use | Interactive multimedia educational content (e.g., quizzes, Q&A | Ethnically diverse adolescent girls |
| Wu, 2019 [ | Rainbow Clinic | China | Platform within dating app | Service navigation, mental health support and peer support | ‘Gay‐friendly’ physician finder; online psychological consultation; in‐person appointment scheduling; peer support. | MSM |
| Ybarra, 2019 [ | Guy2Guy | USA | Interactive SMS | HIV/STI education, Promotion of condom use, HIV testing promotion, peer support | Educational content delivered via automated messaging; quizzes; on‐demand advice; peer support; gamification. | Gay, bisexual, and/or queer adolescent boys |
| First author, year | Study design | Methods used and number of user participants | Domains of user input sought | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Formative | Acceptability | Accessibility | Usability | Satisfaction | Engagement | Impact | |||
| Adeagbo, 2021 [ | Mixed methods | Survey ( | Yes | Yes | Yes | Yes | Yes | ||
| Anderson, 2022 [ | Qualitative only | Focus groups ( | Yes | Yes | Yes | Yes | |||
| Bailey, 2016 [ | Mixed methods | Focus groups ( | Yes | Yes | Yes | Yes | |||
| Biello, 2021 [ | Mixed methods | Outcome questionnaire ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Braddock, 2023 [ | Qualitative only | User testing ( | Yes | Yes | |||||
| Chandler, 2020 [ | Mixed methods | Focus groups ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Cheah, 2024 [ | Mixed methods | SUS, outcome questionnaire, think aloud interviews and semi‐structured interviews ( | Yes | Yes | Yes | Yes | Yes | ||
| Cordova, 2018 [ | Mixed methods | Session evaluation form, CSQ | Yes | Yes | Yes | Yes | Yes | Yes | |
| Danielson, 2016 [ | Mixed methods | Think aloud interviews and WAMMI | Yes | Yes | Yes | ||||
| Engen, 2021 [ | Mixed methods | Semi‐structured interviews ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Fitzpatrick, 2023 [ | Mixed methods | SUS and patient‐reported experience measures ( | Yes | Yes | Yes | Yes | Yes | ||
| Gilbert, 2017 [ | Qualitative only | Think aloud interviews ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Goldenberg, 2015 [ | Qualitative only | Focus groups ( | Yes | Yes | Yes | Yes | |||
| Greene, 2016 [ | Mixed methods | Abbreviated Acceptability Rating Profile and self‐report outcome measures (Sexual Health and HIV Risk Behaviours, HIV Knowledge Questionnaire, Condom Use Errors and Problems Questionnaire ( | Yes | Yes | Yes | Yes | |||
| Hughes, 2021 [ | Mixed methods | Semi‐structured interviews and chart review ( | Yes | Yes | Yes | Yes | |||
| Ippoliti, 2021 [ | Qualitative only | Prototyping, in‐depth interviews, focus groups and engagement data ( | Yes | Yes | Yes | Yes | Yes | ||
| Janssen, 2020 [ | Qualitative only | Semi‐structured interviews ( | Yes | Yes | Yes | Yes | Yes | ||
| Levy, 2015 [ | Mixed methods | Survey ( | Yes | Yes | Yes | ||||
| Li, 2023 [ | Mixed methods | In‐depth interviews ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Lindayani, 2021 [ | Mixed methods | Think aloud interviews, SUS, Intrinsic Motivation Inventory and global rating ( | Yes | Yes | |||||
| Liu, 2024 [ | Mixed methods | Focus groups ( | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mauka, 2021 [ | Mixed methods | Pre‐ and post‐pilot focus groups and engagement data ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Nadarzynski, 2021 [ | Qualitative only | Semi‐structured interviews ( | Yes | Yes | Yes | Yes | |||
| Rael, 2023 [ | Mixed methods | Computer assisted self interview of user experience and outcomes and in‐depth interviews ( | Yes | Yes | Yes | Yes | Yes | ||
| Sales, 2019 [ | Mixed methods | Usability questionnaire and interview ( | Yes | Yes | Yes | Yes | Yes | ||
| Schaaf, 2024 [ | Qualitative only | Focus groups and Think aloud interviews ( | Yes | Yes | Yes | ||||
| Schnoor, 2024 [ | Qualitative only | Focus groups ( | Yes | Yes | Yes | ||||
| Sharma, 2022 [ | Mixed methods | Pre‐ and post‐pilot self‐report outcome measures ( | Yes | Yes | Yes | Yes | Yes | ||
| Sun, 2020 [ | Mixed methods | Think aloud interviews, ratings of difficulty, appearance, perceived usefulness and educational value, and open questions ( | Yes | Yes | Yes | Yes | Yes | ||
| Velloza, 2024 [ | Qualitative only | Semi‐structured, in‐depth interviews ( | Yes | Yes | Yes | Yes | Yes | Yes | |
| Visser, 2020 [ | Mixed methods | Knowledge, attitudes, practices and behaviours survey ( | Yes | Yes | Yes | Yes | |||
| Widman, 2016 [ | Qualitative only | Think aloud interviews ( | Yes | Yes | Yes | Yes | |||
| Wu, 2019 [ | Mixed methods | Focus groups and questionnaire ( | Yes | Yes | Yes | Yes | |||
| Ybarra, 2019 [ | Mixed methods | Post‐intervention survey ( | Yes | Yes | Yes | Yes | |||
| Number of projects seeking this domain of input | 24 | 25 | 17 | 31 | 27 | 11 | 22 | ||
- —A.J.K.'s position during the conduct of this review was funded by an Australian NHMRC Emerging Leadership Investigator Grant (GNT1172873) held by Professor Eric Chow and an Australian NHMRC Leadership
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMobile Health and mHealth Applications · Social Media in Health Education · Sexuality, Behavior, and Technology
Introduction
1
Digital tools to promote the prevention and treatment of sexually transmitted and blood‐borne infections (hereafter referred to as ‘digital sexual health tools’) are a growing part of the sexual health landscape. Examples include sexual and reproductive health (SRH) education platforms, self‐testing websites, smartphone applications and, more recently, AI‐powered chatbots and photo diagnosis applications. Their value in impacting their intended outcomes, however, has yet to be conclusively proven. In the past decade, no less than six systematic and scoping reviews on digital sexual health (DSH) tools have been published [1, 2, 3, 4, 5, 6]. Almost universally, they report mixed or ‘preliminary’ results [1, 2, 4] and even the potential to produce outcomes counter to their purpose [3]. Limitations in the design of research into DSH tools have been identified, particularly the rigour of evaluations [2, 6], but also the variability in seeking and incorporating user input (i.e., perspectives, suggestions and feedback from potential users) during the design process.
Reviews of DSH tools have highlighted inadequate tailoring of tools to meet the needs of users as a potential barrier to their effectiveness [2, 5]. Seeking user input may result in the translation of tool effectiveness to real world impact by supporting uptake and repeated use [7]. Veronese et al. [1] found that DSH technologies that benefited from user input in the design process had a greater impact. Differences in approaches to seeking user input across the technology and public health sectors are evidenced in the heterogenous methods used in tool development and evaluation [8]. While patient and public involvement, including co‐design, is increasingly recommended in the development of health products and services, there are few studies linking processes undertaken to seek user input with outcomes [9, 10]. With reference to DSH tools, Balaji et al. [4] identified the need for additional user experience constructs beyond ‘current technology acceptance models’. Building on these findings, this review sought to take a broader scope on the DSH literature to explore how user input in the design of tools might be improved.
In this review, we describe the methods used in the development of DSH tools to seek input from end users of tools, the domains of input reported, and evidence of their incorporation into tool design. Consistent with these aims, we chose a scoping review method to map qualitative and mixed methods research studies of DSH tools and answer the following questions: (1) What approaches have been used to seek the views of potential users of DSH tools? (2) To what extent does the reporting of user input in publications suggest their input is meaningfully shaping the development of DSH tools?.
Methods
2
This review followed the process described by Arksey and O'Malley [11] and further refined by O'Brien, Colquhoun [12]. It is reported with reference to the Preferred Reporting Items for Systematic reviews and Meta‐Analyses extension for Scoping Reviews (PRISMA‐ScR) [13]. No protocol was published, and the review was not registered.
Eligibility Criteria
2.1
Consistent with our focus on user input we limited our review to qualitative or mixed methods studies that sought user views on purpose‐built DSH tools, including early prototypes of any fidelity (e.g., paper mock ups, wireframes) through to pilot studies of developed tools. After an initial search, we opted to limit our search to the previous 10 years as few tools, except websites, were reported before 2015. Studies conducted before prototyping (i.e., in the formative stages of development) were not included, as we were interested in exploring the use of user input over time, but mention of earlier studies in later studies was captured in data charting. We chose to exclude serious video games from our review as the gamification of health interventions requires a methodological approach that is quite different from other digital health interventions, and an evidence map was recently published of these interventions [14]. We also chose to exclude digital vending machines as descriptions we found in published studies did not meet our criterion of providing information and services tailored to user inputs. As described by Arksey and O'Malley [11], the focus of our study was iteratively refined as we developed an understanding of the breadth of research in the field, resulting in the final inclusion and exclusion criteria shown in Table 1, that were applied during study selection.
Information Sources
2.2
Peer reviewed publications were sourced from database searches in MEDLINE (Ovid), PsycInfo (Ovid), and the Social Science Citation Index (Web of Science). At the time of searching, auto alerts for all three searches were created and checked until 12 September 2024 and relevant studies subjected to the same screening process described below. No grey literature was included.
Search
2.3
Search terms were chosen to capture each of four key concepts in the review questions. Terms were searched as identical key words in all databases and similar related subject headings specific to each database. An example of the terms used in MEDLINE is provided in Table 2. Key word and subject headings for each concept were combined using the ‘or’ Boolean operator then the search results for each concepts combined using ‘and’ (Files [Link], [Link], [Link]).
Selection of Sources
2.4
Search results were uploaded to Covidence systematic review software (Veritas Health Innovation). Duplicates were removed by the automated function of this application and manually during screening, by sorting the uploaded citations by author and marking duplicates not identified by Covidence. All titles and abstracts were screened by A.J.K. and E.T.C. and conflicts resolved in discussion with K.A. The same process was applied at full‐text review. Additional studies were identified for screening by checking the references lists of studies included following full text review and any review papers found in our search results. Potential references found through citation searching were reviewed by A.J.K. and E.T.C. and any conflicts resolved by K.A.
Data Charting Process
2.5
Data charting was conducted in Excel. A.J.K. and E.T.C. each extracted data from half of the included studies by copying relevant text verbatim into predefined fields of a shared sheet. Fields of interest were drafted by A.J.K. and E.T.C. and refined in discussion with K.A. and P.F. A.J.K. and E.T.C. checked a random selection of the other's allocated studies and met to discuss differences in their extraction approach.
Data Items
2.5.1
The fields used for data charting are provided in File S4. For most items, verbatim text was input into the field with the following exceptions. Where not clearly stated in the description of the tool, the purpose was determined based on the introduction of the paper. Where the research aim was not clearly stated, the domains of user input captured by research tools were entered (e.g., usability if System Usability Scale used).
Approach to Synthesising Results
2.6
To answer our research questions, we reviewed the data extracted from the included studies and applied the following methods of data synthesis.
Domains of User Input Explored in Studies
2.6.1
A.J.K. and E.T.C. reviewed the data extracted from the Research details and User input fields in File S4 with reference to the following questions describing seven domains of user input. The questions were developed following familiarisation with the data set during charting and revised in consultation with co‐authors working in the DSH field (K.A., M.G., P.F.).
- Were potential users invited to make a formative contribution to design and scoping, before prototype development? (defined in this paper as formative input).
- Were potential users asked if they would be willing to use it or if they would prefer it to alternatives? (defined as acceptability)Were users asked about aspects of the tools that might prevent them or others from using the tool due to individual factors (e.g., low literacy, physical, sensory or cognitive impairment, English language proficiency)? (defined as accessibility).
- Were users asked how easy‐to‐use or user friendly the tool was? (defined as usability).
- Were users asked about their satisfaction or experience of using the tool at any stage (including if they would recommend it to others)? (defined as satisfaction).
- Did the study measure users’ spontaneous and/or in situ use of the tool or features of the tool beyond user testing (i.e., as the need for sexual health information or advice arose)? (defined as engagement).
- Were participants asked what impact the tool had or might have on the intended outcome (e.g., knowledge, healthcare seeking, HIV/STI testing, condom use)? (defined as impact).
A.J.K. and E.T.C. reviewed the stated aims and reported findings of each of the included studies and made a qualitative decision as to which domains were explored within the project, guided by the questions shown for each domain. Figure 1 depicts the domains of input reviewed in our data synthesis in a provisional theory of change [15] suggesting the potential role each type of input may have in achieving a tool's intended impact.
Domains of user input and their potential role in achieving impact.
Reporting of Impact of User Input on Tool Development
2.6.2
The impact of user input on the development and refinement of tools was synthesised by reviewing data extracted from individual studies in relation to:
- Participant suggestions for changes or additional features.
- Planned or executed changes to the tool in response to user input.
Examples of participant suggestions being incorporated into tools are reported in the results that follow.
Results
3
Selection of Sources of Evidence
3.1
The process of study selection and the number of sources screened for inclusion is shown in Figure 2. In brief, 1838 unique titles and abstracts were screened, included three studies found through auto alerts after our initial searches and six from the reference lists of included studies and reviews. Fifty peer‐reviewed publications were subjected to full text review resulting 37 included studies.
PRISMA flow diagram showing the process of study selection.
Description of Included Studies
3.2
An overview of projects (n = 34) described in included studies (n = 37) is provided in Table 3. Six studies related to different phases of the same three projects, so the findings of these studies are reported together in the tables below. Thus, the attributes of 37 individual studies are reported in relation to 34 projects using individual DSH tools (n = 31) or multiple tools in combination (n = 3).
Domains of User Input and Methods Used to Explore Them
3.3
A summary of the methods used, and the domains of user input sought in the development and refinement of DSH tools is provided in Table 4. In roughly two‐thirds of studies (n = 23), qualitative methods such as interviews, focus groups and free‐text responses to surveys were complemented by quantitative measures such as self‐report measures and engagement analytics. Further description of the range of methods used to explore various domains of user input is provided in the text that follows.
Formative Input
3.3.1
Twenty‐four of thirty‐four projects reported seeking user input in the development of the prototype or tools they evaluated. This included conducting interviews or focus groups with end users on their sexual health needs or consulting with advisory groups. A further seven studies did not report on this aspect of development, and three reported tool development by subject matter experts without user input.
Those studies that sought formative user input created tools that were more closely aligned with the suggestions made by users providing feedback at later stages of development in other tools. For example, a crowdsourcing call reported in Wu et al.'s study [51] resulted in the development of a physician finder tool that men who have sex with men could use to find gay‐friendly doctors. Similar suggestions were made by focus group participants in the formative stages of the SavvyHER application, which incorporated a feature identifying local HIV testing locations: ‘… something where you could get a directory of… Female Black doctors in your area. I think that would be very, very helpful because I have no idea of any Black women doctors in Atlanta’. [Focus group participant] [18]. Similar requests for information about the location of sexual healthcare providers were made by teenage girls in later stages of tool development in Widman et al.‘s [50] and Levy et al.'s [36] studies, but it was unclear whether this suggestion was taken up by the developers.
Acceptability
3.3.2
The acceptability of tools to users was explored in twenty‐five of the thirty‐four projects. Quantitative measures of this domain included a mix of those designed for the specific study [22, 28, 47, 52] and standardised measures. The latter included the Abbreviated Acceptability Rating Profile [24, 39]. Qualitative feedback indicated features that impacted the acceptability of tools, such as anonymity, privacy, convenience and appearance.
Black women in Chandler et al.'s [22] study commented on the representativeness of a tool designed with formative input. In contrast, a self‐testing tool that had not had formative input from transgender users received negative feedback on its acceptability.Put the [transgender pride] flag up in a corner… and maybe a girl with long hair, and a hand with long fingernails. Tonterias [silly things] like that… that'll make you laugh and giggle…. You don't want it to seem–… I'm… doing an institutional thing–I feel like I got the Feds hearing me.[Interview participant] [42]
Participants also speculated about the acceptability of specific application features to other users: ‘It's a matter of privacy with the reminders. I personally don't care if people see my phone when the notification is going to come up. But some people don't want that kind of stuff visible’ [Focus group participant] [30].
Qualitative descriptions of acceptability also compared digital tools to in person care: ‘I understand that as being the trade‐off. For like, the ease and simplicity, vs. like, having that like, specific person to contact and like, them being like, readily available’ [Interview participant] [32].
Accessibility
3.3.3
User input relevant to accessibility was reported in only half of included projects, and most often in general terms rather than intentional consideration of users with special needs. No quantitative measures were identified capturing feedback on accessibility. However, qualitative feedback from users reflected potential barriers to use for some users.
Mixed feedback from participants on comprehension of text in some studies [18, 28] suggests consideration of accessibility for people with low literacy or English language proficiency. For example, Biello et al.'s [19] study of a tool for self‐testing indicated the instructions provided were not accessible for some users: ‘…what am I supposed to—I didn't know why I got confused honestly, but… I just… kept putting them off, because I was, like… I don't want to do this wrong’ [Interview participant]. Similarly, user input suggesting or appreciating the use of voiceovers, video, and visual guides are relevant to the accessibility of text‐based content [20, 23, 32, 42, 45, 49].
User input relevant to accessibility to people with visual impairments included the size of ‘buttons’ [43], contrast of text [16], concern about working on a small screen [25], modification of visual presentation [43], and sounds [38, 47].
Usability
3.3.4
Use of methods to assess the usability (also referred to as ‘ease‐of use’) of tools was the most frequently reported (n = 31) domain of user feedback. The most frequently used standardised measure, of any user feedback domain, was the System Usability Scale which was used in six projects [22, 23, 28, 37, 38, 39] but the Website Analysis and MeasureMent Inventory was also used by Danielson et al. [25]. A commonly used (n = 7) qualitative method to assess usability was ‘think aloud’ interviews, which enabled researchers to identify usability problems while users were using the tool [23, 25, 29, 38, 44, 47, 50]. Other forms of qualitative feedback described how usability could impact user satisfaction and their future uptake: ‘… the amount of times that I had to try to take those pictures and to get them online, I thought that was one of the biggest cons’’ [Interview participant] [26].
Satisfaction
3.3.5
Satisfaction (also referred to as user experience) was the next most common (n = 27) domain of user feedback sought by tool developers. Quantitative measures of satisfaction included a mix of those designed for the specific study [22, 28, 47, 52] and standardised measures. The latter included the Client Satisfaction Questionnaire [24, 39], and the Intrinsic Motivation Inventory [38]. Six studies measured satisfaction by asking users if they would recommend the tool to a friend [23, 24, 28, 40, 47, 52]. Qualitative feedback allowed participants to describe factors impacting their satisfaction that might not be captured in quantitative data: ‘I ‘ain't want to say that's aggressive either, but the way she [person in educational video] talking sound aggressive’ [Interview participant] [25].
Engagement
3.3.6
Given that not all included projects had progressed to user testing, data relating to whether participants spontaneously used tools was reported in less than a third of the tools evaluated (n = 11). In studies that involved a pilot period of user testing, quantitative measure of engagement were more frequently extracted from the tool [33, 39, 40, 47] than self‐reported by participants [37]. In addition to how often and for how long they used tools, qualitative feedback on engagement described how and when they might be used.I used the HIV self‐test kit and read some articles…. Once after I know all about this [PrEP], I don't use it often. If I suddenly forget about something [about PrEP] or not sure of something, I will go back [to the mini‐app]. Or when I am really sick or need to look up something. If others ask me [about PrEP], I would just refer them to the mini‐app, or share some of the articles to them.[Interview participant] [37]
Qualitative feedback also captured unexpected engagement with tools that might not have been reflected in quantitative measures of engagement. For example, an interview participant without internet access in Mauka et al.'s [40] study was prompted to take her PrEP dose by seeing the application logo on her phone: ‘I have never received the message but, since I like to use the phone, once I see the app's logo, I remember to take medicine’.
Impact
3.3.7
Users’ feedback on the potential or actual impact of tools on their sexual health knowledge or behaviours was commonly reported (n = 22). Self‐report outcome questionnaires were used in several studies to assess impacts on sexual health knowledge and engagement with prevention (e.g., condom use, PrEP use) and HIV/STI testing. These questionnaires were often designed for the study [16, 18, 23, 42, 47, 49, 52]. Standardised measures of impact on knowledge and behaviour, such as the HIV Knowledge Questionnaire, Sexual Health and HIV Risk Behaviours, and the Condom Use Errors and Problems Questionnaire [31], and confidence, such as the PrEP Adherence Self‐Efficacy Scale [39], were used rarely. Qualitative methods captured impacts on similar outcomes to those measured in self‐report measures, providing more nuanced description of changes that occurred: ‘The iloveLife.mobi site gave me knowledge to confront my fear of knowing my HIV status. I have been to the clinic and tested for HIV’ [Survey participant] [49].
Reported Incorporation of User Input
3.4
User centred research and design approaches cited in studies included ‘human centred design’ [26, 44], ‘codesign’ [28, 33], ‘human computer interaction person‐based’ [16], ‘community‐engaged’ [21], ‘community based participatory research’ [24], ‘user centred design’ [39], participatory design of interaction [43], ‘user‐driven’ [47], and ‘crowdsourcing’ [51]. However, references to such approaches were not consistently supported by evidence of changes to tools based on user input. Suggestions for changes or additional features were reported in many studies (n = 25). These suggestions, sometimes reflected a mismatch between the needs of users, as perceived by tool developers, and the reported needs of users which might be met by different technological solutions, information content or tool features. For example, a survey participant in Greene et al.'s [31] evaluation of a website promoting condom use suggested they: ‘take into consideration the new PrEP [HIV pre‐exposure prophylaxis] medicine and also give realistic happenings without condom use’. Most studies (n = 20) failed to report changes made or planned to tools in response to these suggestions.
Discussion
4
Summary of Evidence
4.1
This scoping review of published qualitative and mixed methods studies of DSH tools sought to describe the approaches taken to seeking and incorporating user input. Studies were reviewed in relation to the domains of input sought from potential users, and the degree to which user contributions were incorporated into the development and refinement of tools.
In relation to our first aim – identifying the types of user input sought ‐ projects included in this review most often sought input on usability. Formative input and input regarding the acceptability of tools and their features was not sought in a third of projects. Crucially, few studies reported asking users whether they saw a need for the tool, in the first place, or what type of tool would best meet their needs. Only half of projects reported findings relevant to accessibility, and often without purposefully seeking this input in their research design. Usability may be irrelevant if a tool is not useful, appealing or accessible to the population it is designed to target.
In relation to our second aim, reported incorporation of user input was similarly variable. In part, this may reflect the earlier developmental stage of some tools at the time of publication. However, where user input was clearly incorporated into iterative tool development, subsequent feedback from users reflected a high degree of satisfaction, suggesting potential for further engagement and impact, as proposed in our theory of change (Figure 1). This assertion is supported by Veronese et al.'s [1] recent review of digital interventions to improve HIV testing that found tools incorporating user input were more impactful. While the engagement of target populations in the development of complex health interventions is increasingly mandated in health policy and research practice [53], evaluations linking processes of seeking user input with health intervention outcomes are limited [9, 10]. Future research in the DSH space might benefit from evaluating theories of change [15], such as the one we have proposed in Figure 1. Moreover, combining explanatory models from both the digital (e.g., unified theory of acceptance [54], privacy calculus [55]) and experience‐based co‐design (EBCD) [56] literature (e.g., theoretical explanatory model of change for co‐design and co‐production in healthcare improvement [57]) may provide insight into mechanisms of change. In comparing approaches from technology and community‐focussed research, Chen et al. [8] argue that integrating human‐centred design (HCD) and community‐based participatory research (CBPR) approaches may result in improved impact of public health interventions. While both are ‘people‐centred’ approaches focussed on iterative co‐creation of solutions, each approach has unique and complementary strengths that may be leveraged in the design of DSH tools. Aspects of EBCD, HCD, CBPR, and crowdsourcing approaches will be discussed in relation to the review findings in the following guidance for developers of DSH tools, while acknowledging that other approaches to seeking user input may be equally relevant and valid.
Suggested Guidance for Developers of Digital Sexual Health Tools
4.2
Involve End Users Early
4.2.1
Seeking input from end users earlier in the development process, allowed the developers of DSH tools to establish the need for a tool, and incorporate user suggestions into their tools, such as the type of tool and its features. In contrast, suggestions made at later stages of development were not consistently reported as being incorporated into tools. Moreover, authors who had only included clinician perspectives in formative work reflected on the limitations of this approach.The app's design solution used in this study was initially based on the view of HIV experts. Subsequently involving patients is essential, as they identify needs not mentioned by the experts. We therefore recommend early consideration of clinical perspectives and patient needs and discussing them with experts [44].
The findings of our study suggest that the choice of method for seeking input is less important than the choice to prioritise users’ needs from the outset of tool development. Consistent with the information gathering stage of experience‐based co‐design [56], interviews, focus groups and surveys have been successfully used in the early stages of online sexual health services to gain valuable insights into perceptions and likely uptake [58]. Beyond traditionally used methods, methods from other fields offer inspiration for developers. Crowdsourcing methods from the field of behavioural economics have been used successfully to generate ideas from target populations [50, 59]. In the field of technology, HCD is described by Chen et al. [8] as a highly a creative approach which may support the generation of novel technological solutions rather than use of existing technologies to meet a healthcare need identified through participatory research.
Engage Your Target Population, Including ‘Extreme Users’
4.2.2
While many included studies reported use of person‐centred approaches, users engaged in the development of tools were not always representative of the populations who might most benefit from tools. For example, participants in some studies of tools targeting a general population were mostly female [26, 41], white [41] or born in the country of study [29]. Some tools targeting adolescent and youth populations excluded participants under 18 years [16, 50]. Some included studies seeking user input on tools promoting PrEP recruited almost exclusively male [28, 44] participants and those over 30 years of age [44].
DSH tools are often promoted as a means of improving access to sexual health information and services for populations experiencing barriers to in person care. However, exclusion of users with access needs (e.g., people with limited English language proficiency or low literacy, people with disabilities) from formative research may serve to deepen health inequalities by providing convenient access for those already able to access information and services in other ways. Chen et al. [8] recommend researchers adopt the HCD approach of working ‘extreme’ users to ensure public health interventions are accessible to a wider audience. However, HCD approaches tend to focus on scalability rather than the localised approach of participatory research which may be better suited to populations with specific needs. In relation to DSH tools, developers should seek to ensure their target audience is represented in those they seek input from as this has been correlated with improve impact on outcomes [1]. Moreover, to ensure accessibility, behavioural science approaches, such as the behaviour change wheel, may be helpful in systematically identifying and addressing barriers to, and facilitators of, use [60].
Create Opportunities for Unexpected Input
4.2.3
While this review excluded studies where only quantitative user input was sought, comparison of the quantitative and qualitative data presented in mixed methods studies suggest that the inclusion of qualitative data in formative evaluations of DSH tools is essential to capture more nuanced and open input. This was particularly true of studies which employed interview or focus group methods and, to a lesser degree, open text responses to questionnaires. Where quantitative data was collected regarding acceptability, satisfaction or engagement, qualitative data provided explanation of quantitative findings. Given the mixed findings of several reviews of quantitative studies of DSH tools it may be time to recognise the value of qualitative data in tool development [1, 2, 4].
Involve Users More Than Once
4.2.4
Projects that included users throughout the development process were more likely to report making changes to their planned approach and positive feedback from users on prototypes or final products. Chen et al. [8] suggest conducting rapid and repeated rounds of prototyping towards tangible outputs that users can test. This contrasts with other forms of qualitative and participatory research which can be slow in generating outputs.
Close the Feedback Loop
4.2.5
A notable gap in reporting was changes made to tools in response to user input. An essential aspect of co‐design processes is transparency in how input was used, as prioritised in the relational approach of participatory research [8, 57]. Reporting in research publications demonstrates commitment to responding to user input. In addition to reporting how feedback was used, the revised Guidance for Reporting Involvement of Patients and the Public provides a benchmark for reporting [61].
Strength and Limitations
4.3
This review undertook a rigorous process of searching, screening, data extraction and synthesis of peer reviewed studies of DSH tools. The diverse disciplinary and regional perspectives amongst coauthors further supported a holistic approach to data analysis. While several literature reviews of DSH applications have been published, this is the first to focus on the methods used and domains of input sought by researchers.
The review is limited in that we did not search in languages other than English, preprints or the proceedings of conferences, or other grey literature. Given the fast moving and competitive digital field, it seems likely that many more applications are developed through market, rather than health, research. Moreover, as we were using published research from various stages of tool development, our data extraction and analysis may have omitted aspects of projects not, or not yet, reported by authors. Similarly, our choice to exclude purely formative research may have limited our ability to assess this domain, if these studies were not referenced in later publications. Limitations in the reporting of included studies further limited the scope of our analysis. For example, researchers did not make explicit commercial interests that may have influenced the reporting of negative feedback or the limitations in accessibility of tools due to cost. Qualitative findings in included studies also tended to be reported as themes rather than exploring relationships between factors and outcomes.
A significant limitation of the review is the omission of Arksey and O'Malley's [11] suggested sixth stage of stakeholder consultation, which, due to resourcing limitations, we were unable to undertake. Seeking the views of potential users of DSH tools would have added depth and nuance to our interpretation of the findings. While we adhered to established scoping review methodology and the Preferred Reporting Items for Systematic reviews and Meta‐Analyses extension for Scoping Reviews (PRISMA‐ScR) [54] no protocol was published and, thus, our methods not subjected to peer review and revision.
Conclusions
5
This review found inconsistent user input into the development of DSH tools which may, in part, explain their mixed effectiveness in improving sexual health outcomes, as reported in previous systematic reviews [1, 2, 3, 4]. If DSH tools are to achieve their promise, we must move beyond evaluating the functionality of design solutions and meaningfully engage users as partners in co‐design. Future research should seek to ensure fidelity to established principles of co‐design and build the evidence base for the impact of these approaches on outcomes.
Author Contributions
Alicia King: conceptualisation, methodology, formal analysis, investigation, validation, data curation, writing – original draft, visualisation, project administration. Ethan Cardwell: conceptualisation, methodology, formal analysis, investigation, data curation, writing – review and editing. Eric Chow: funding acquisition, writing – review and editing, supervision. Paul Flowers: conceptualisation, methodology, writing – review and editing. Mark Gilbert: methodology, writing – review and editing. Kath Albury: conceptualisation, methodology, validation, writing – review and editing, supervision.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
UserInputinDSH_Supplement_1.
UserInputinDSH_Supplement_2.
UserInputinDSH_Supplement_3.
UserInputinDSH_Supplement_4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. Veronese , K. E. Ryan , C. Hughes , M. S. Lim , A. Pedrana , and M. Stoové , “Using Digital Communication Technology to Increase HIV Testing Among Men Who Have Sex With Men and Transgender Women: Systematic Review and Meta‐Analysis,” Journal of Medical Internet Research 22, no. 7 (2020): e 14230.32720902 10.2196/14230 PMC 7420634 · doi ↗ · pubmed ↗
- 2D. F. Conserve , L. Jennings , C. Aguiar , G. Shin , L. Handler , and S. Maman , “Systematic Review of Mobile Health Behavioural Interventions to Improve Uptake of HIV Testing for Vulnerable and Key Populations,” Journal of Telemedicine and Telecare 23, no. 2 (2016): 347–359.27056905 10.1177/1357633 X 16639186 PMC 5102818 · doi ↗ · pubmed ↗
- 3A.‐F. Abdulai , A. F. Howard , and L. M. Currie , “Stigmatizing and De‐Stigmatizing Properties of Web Apps for Sexual Health‐Related Conditions: A Scoping Review,” International Journal of Sexual Health 34, no. 1 (2022): 144–159.38595685 10.1080/19317611.2021.1949655 PMC 10903607 · doi ↗ · pubmed ↗
- 4D. Balaji , L. He , S. Giani , T. Bosse , R. Wiers , and G. J. de Bruijn , “Effectiveness and Acceptability of Conversational Agents for Sexual Health Promotion: A Systematic Review and Meta‐Analysis,” Sexual Health 19, no. 5 (2022): 391–405.35863761 10.1071/SH 22016 PMC 7613710 · doi ↗ · pubmed ↗
- 5G. T. Aboye , M. Vande Walle , G. L. Simegn , and J. M. Aerts , “Current Evidence on the Use of m Health Approaches in Sub‐Saharan Africa: A Scoping Review,” Health Policy and Technology 12, no. 4 (2023): 100806.
- 6D. Gilbey , H. Morgan , A. Lin , and Y. Perry , “Effectiveness, Acceptability, and Feasibility of Digital Health Interventions for LGBTIQ+ Young People: Systematic Review,” Journal of Medical Internet Research 22, no. 12 (2020): e 20158.33270039 10.2196/20158 PMC 7746499 · doi ↗ · pubmed ↗
- 7C. Herkommer and S. S. Laine , “Smooth Sailing: An Exploratory Study Navigating the Acceptance of Digital Health Solutions and the Impact on Seafarer Well‐Being” (master's thesis. Jönköping International Business School, Jönköping University, 2023), 82, https://www.diva-portal.org/smash/get/diva 2:1760627/FULLTEXT 01.pdf.
- 8E. Chen , C. Leos , S. D. Kowitt , and K. E. Moracco , “Enhancing Community‐Based Participatory Research Through Human‐Centered Design Strategies,” Health Promotion Practice 21, no. 1 (2020): 37–48.31131633 10.1177/1524839919850557 · doi ↗ · pubmed ↗