Prophylactic Application of Closed-Incision Negative Pressure Therapy in a High-Risk Emergency Laparotomy: A Case Report
Swapnil Tripathi, Avinash Ray, Tanya Dhawan, Mohammed Athif Khan

TL;DR
This case report shows how a new wound therapy helped a high-risk patient recover quickly after abdominal surgery.
Contribution
Demonstrates the practical benefits of closed-incision negative pressure therapy in a high-risk emergency laparotomy case.
Findings
ciNPT with foam dressings prevented infection and dehiscence in a high-risk patient.
The patient recovered quickly and was discharged on postoperative day six.
Imaging confirmed effective wound healing under ciNPT.
Abstract
Surgical site infections (SSIs) and wound dehiscence are common complications following laparotomy, particularly in patients with comorbidities such as diabetes and obesity. Closed-incision negative pressure therapy (ciNPT) is increasingly recognised for its potential to improve surgical site outcomes by reducing infection rates and promoting wound healing. This case report describes the use of ciNPT in a patient with a high-risk surgical incision, highlighting its clinical benefits and practical application. We report the case of a 68-year-old obese female with type 2 diabetes mellitus who underwent emergency laparotomy for perforated diverticulitis. ciNPT with novel foam dressings was used postoperatively. The wound healed without infection or dehiscence. The patient experienced minimal discomfort and was discharged on postoperative day six. The therapy demonstrated effective…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
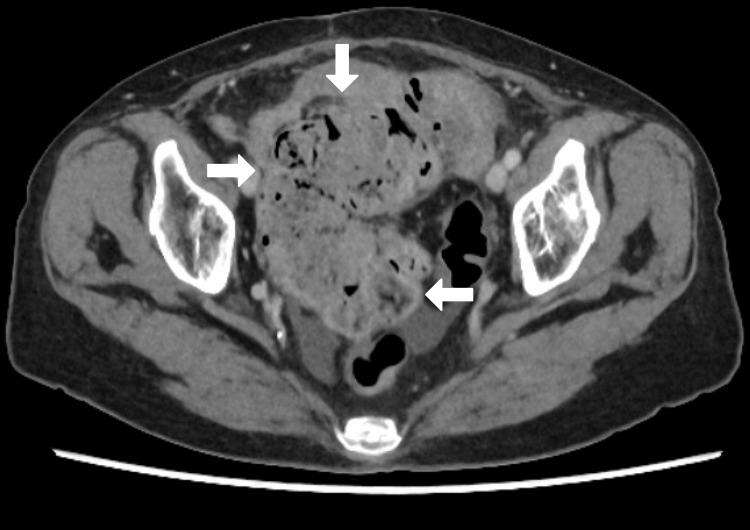 Figure 1
Figure 1 Figure 2
Figure 2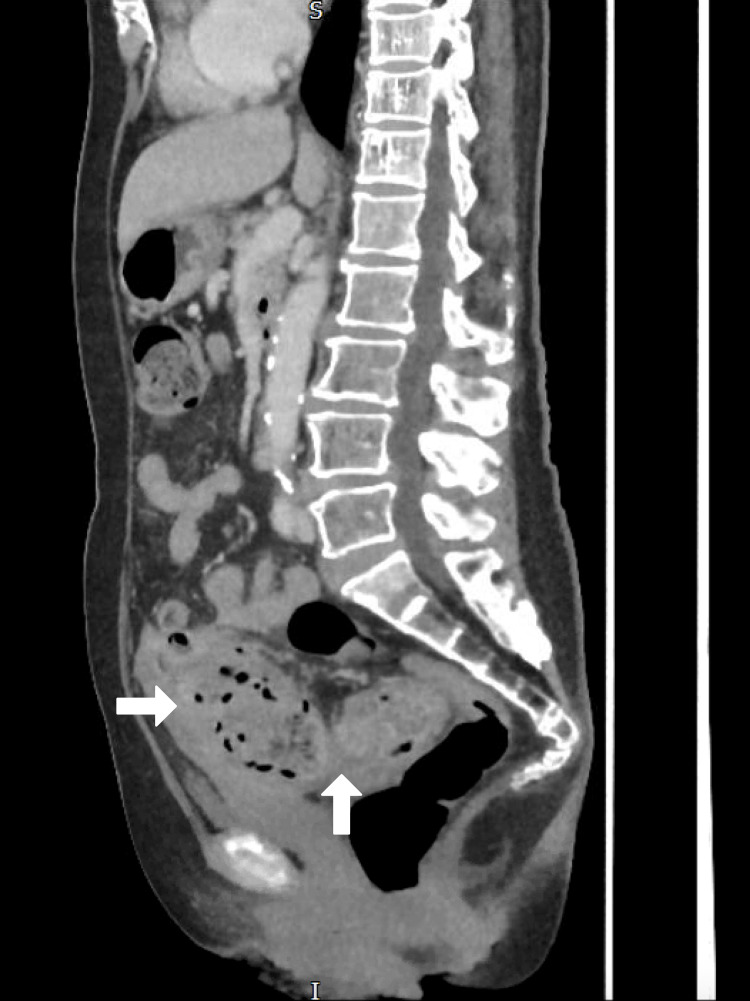 Figure 3
Figure 3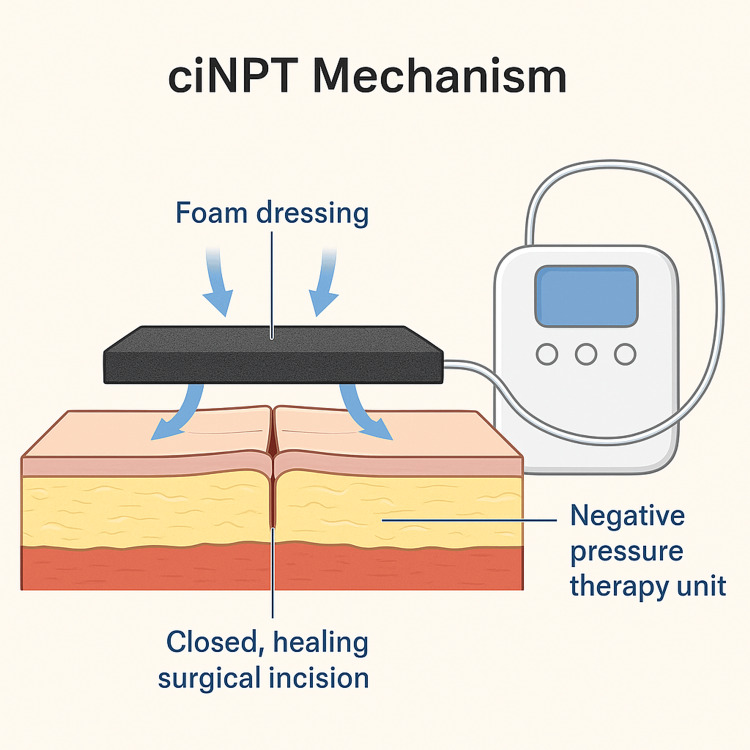 Figure 4
Figure 4| Parameter | Findings |
|---|---|
| Age/Gender | 68-year-old female |
| BMI | 37 kg/m² (Obese) |
| Comorbidities | Type 2 Diabetes Mellitus (HbA1c: 9.2%) |
| Presenting Symptoms | Generalised abdominal pain, fever, vomiting |
| Duration of Symptoms | 2 days |
| Physical Examination | Tenderness and guarding in the lower abdomen |
| Initial Investigations | Elevated WBC (14,800/mm³), CRP 163 mg/L |
| Imaging Findings | CT scan showed Hinchey stage II perforated diverticulitis with localised peritonitis and impacted stool in sigmoid colon |
| Surgical Procedure | Emergency midline laparotomy with Hartmann’s procedure |
| ciNPT Protocol | Single polyurethane foam dressing with -125 mmHg suction applied intraoperatively and maintained for 5 days |
| Postoperative Outcome | No infection or dehiscence, complete wound healing by Day-30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Pelvic and Acetabular Injuries · Abdominal Surgery and Complications
Introduction
Surgical site infections (SSIs) remain among the most common postoperative complications, particularly in abdominal surgeries, leading to increased morbidity, prolonged hospital stays, and healthcare costs [1,2]. Patients with obesity, diabetes mellitus, or undergoing emergency procedures are especially vulnerable [3]. Emergency colorectal procedures and surgeries involving perforation or peritonitis are particularly prone to infection.
Closed-incision negative pressure therapy (ciNPT) has emerged as a novel strategy to enhance healing and reduce wound complications in high-risk patients. The therapy involves the application of a sterile, sealed dressing connected to a negative pressure unit, aiming to reduce tension at the incision site, remove exudate, and improve perfusion [4,5]. It also creates a sealed environment that protects the wound from external contamination.
ciNPT is most commonly indicated in patients at high risk of wound complications, including those undergoing abdominal, vascular, orthopaedic, and cardiothoracic surgeries. Its use is particularly prevalent in obese and diabetic patients, and in procedures with high contamination risk or complex wound closure. Several clinical guidelines and studies have supported its role in reducing postoperative complications in these contexts.
This report presents the successful use of ciNPT with novel foam dressings in a high-risk patient undergoing emergency laparotomy, contributing further evidence for its routine use in select surgical populations.
Case presentation
A 68-year-old female presented with a two-day history of generalised abdominal pain, fever, and vomiting. She had a history of poorly controlled type 2 diabetes mellitus (HbA1c: 9.2%) and obesity (BMI 37 kg/m²). On physical examination, she exhibited diffuse abdominal tenderness and guarding. Laboratory investigations revealed leukocytosis (WBC: 14,800/mm³) and elevated CRP (163 mg/L) (Table 1). CT scan confirmed Hinchey stage II perforated sigmoid diverticulitis with localised peritonitis. Also, hard impacted stool was in the sigmoid colon (Figures 1, 2, 3).
CT Abdomen & Pelvis (Axial View)Perforated sigmoid colon just above the promontory with limited contamination in pelvis, the sigmoid colon severely inflamed and full of hard stool with a 2 cm necrotic patch at the mid sigmoid, site of perforation.
CT Abdomen & Pelvis (Coronal View)
CT Abdomen & Pelvis with Contrast (Saggital View)
After initial stabilisation, the patient underwent emergency midline laparotomy and Hartmann’s procedure. Given her comorbidities and increased risk of wound complications, ciNPT was initiated intraoperatively using a novel polyurethane foam dressing system connected to a negative pressure unit set at -125 mmHg (Figure 4). A single ciNPT system was used and remained in place for five days postoperatively, without any dressing change.
Mechanism of Closed-Incision Negative Pressure Therapy (ciNPT)Illustration showing the application of ciNPT over a closed surgical incision using a novel foam dressing connected to a negative pressure unit. Arrows indicate the directional flow of negative pressure, helping to reduce tension, improve perfusion, and protect against infection.
On postoperative day five, the dressing was removed. The incision was clean, dry, and intact with no signs of infection or dehiscence. The patient reported no pain or discomfort from the dressing. She was discharged on post-operative day six, and follow-up visits at day 14 and day 30 revealed a completely healed wound with no complications.
Discussion
Patients with obesity and diabetes are particularly prone to SSIs and wound complications after abdominal surgery [3]. ciNPT is increasingly recognised as a valuable tool for reducing such risks. It offers multiple theoretical advantages: stabilising the incision, reducing lateral tension, and maintaining a closed, protected environment to prevent bacterial ingress [4].
ciNPT prevents infection by improving perfusion, reducing edema, and creating a sealed barrier that limits bacterial contamination. Additionally, continuous negative pressure removes exudate and keeps the wound environment optimal for healing [4,5].
A multicenter randomised controlled trial demonstrated a significant reduction in SSIs when ciNPT was used in obese women undergoing cesarean section (OR 0.55, 95% CI 0.31-0.97) [6]. Similarly, Sahebally et al. showed reduced infection rates and improved outcomes in colorectal surgeries when ciNPT was applied prophylactically [7].
In this case, the use of ciNPT allowed early mobilisation, no wound-related morbidity, and early discharge. These benefits align with existing literature advocating ciNPT use in general and emergency abdominal surgery [8,9].
Though further large-scale prospective studies are needed to develop formal guidelines, accumulating evidence, including this case, supports broader adoption of ciNPT in high-risk surgical patients. While ciNPT systems do have higher initial costs, these are often offset by reductions in complications, reoperations, and length of hospital stay [8].
Conclusions
This case highlights the utility of ciNPT in preventing postoperative wound complications in high-risk emergency laparotomy patients. The successful outcome supports the growing body of evidence favouring ciNPT, especially in individuals with obesity and diabetes. Surgeons should consider its routine prophylactic use in similar scenarios.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee Infect Control Hosp Epidemiol Mangram AJ Horan TC Pearson ML Silver LC Jarvis WR 2502782019991021987510.1086/501620 · doi ↗ · pubmed ↗
- 2Surgical site infection: incidence and impact on hospital utilization and treatment costs Am J Infect Control de Lissovoy G Fraeman K Hutchins V Murphy D Song D Vaughn BB 3873973720091939824610.1016/j.ajic.2008.12.010 · doi ↗ · pubmed ↗
- 3The economic costs of surgical site infection Surg Infect (Larchmt) Fry DE 0433 Suppl 1200210.1089/sur.2002.3.s 1-3712573038 · doi ↗ · pubmed ↗
- 4Closed incision negative pressure therapy: international multidisciplinary consensus recommendations Int Wound J Willy C Agarwal A Andersen CA 3853981420172717023110.1111/iwj.12612 PMC 7949983 · doi ↗ · pubmed ↗
- 5First experience with a new negative pressure incision management system on surgical incisions after cardiac surgery in high risk patients J Cardiothorac Surg Colli A Camara ML 160620112214564110.1186/1749-8090-6-160PMC 3305521 · doi ↗ · pubmed ↗
- 6Prophylactic incisional negative pressure wound therapy reduces the risk of surgical site infection after caesarean section in obese women: a pragmatic randomised clinical trial BJOG Hyldig N Vinter CA Kruse M 62863512620193006645410.1111/1471-0528.15413 PMC 6586160 · doi ↗ · pubmed ↗
- 7Negative pressure wound therapy for closed laparotomy incisions in general and colorectal surgery: a systematic review and meta-analysis JAMA Surg Sahebally SM Mc Kevitt K Stephens I Fitzpatrick F Deasy J Burke JP Mc Namara D 0153201810.1001/jamasurg.2018.3467 PMC 658307430267040 · doi ↗ · pubmed ↗
- 8Incisional negative pressure wound therapy after high-risk lower extremity fractures J Orthop Trauma Stannard JP Volgas DA Mc Gwin G 3rd Stewart RL Obremskey W Moore T Anglen JO 37422620122180441410.1097/BOT.0b 013e 318216 b 1e 5 · doi ↗ · pubmed ↗